I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Random blinded allocation (1:1) to either 30 mg lansoprazole (n=172) twice daily or matched placebo (n=174) twice daily for 16 weeks of patients with persistent throat symptoms.
Eligible patients had persistent (>6 weeks) unexplained throat symptoms—principally hoarseness, throat pain, globus sensation, throat clearing, postnasal secretions or excess mucus, cough, or choking sensation
Primary outcome was symptomatic response at 16 weeks measured using the total reflux symptom index (RSI) score.
Key finding:
No evidence was found of benefit from PPI treatment in patients with persistent throat symptoms. RSI scores were similar between the lansoprazole and placebo groups after 16 weeks of treatment and at the 12 month follow-up.
Improvements (reduction in RSI score) were observed in both groups—score at 16 weeks: lansoprazole 17.4 (15.5 to19.4) and placebo 15.6 (13.8 to 17.3). No statistically significant difference was found between the treatment arms. Furthermore, “no trends were in favour of lansoprazole.”
Limitation: “Our trial could be criticised for lacking any objective measure of GORD within the methodology or for employing any such test as an inclusion criteria. However, we did address the use of PPIs in an empirical setting, which was a near universal practice at the time of our study.”
My take (borrowed in part from authors): “No evidence supports the empirical use of PPIs to treat persistent throat and voice symptoms.” Despite this finding, “old habits die hard” and I predict that it will be a long time before this finding is widely adopted into clinical practice.
This prospective study followed the natural history of NAFLD in children with timed liver biopsy reassessment in children (n=122) using the placebo arms of 2 large multicenter clinical trials; patients received standard of care lifestyle advice. The study population had a mean age of 13 years; 71% were Hispanic participants
Key findings:
At enrollment, 31% of the children had definite NASH, 34% had borderline zone 1 NASH, 13% had borderline zone 3 NASH, and 21% had fatty liver but not NASH
Over a mean period of 1.6 ± 0.4 years, borderline or definite NASH resolved in 29% of the children, whereas 18% of the children with fatty liver or borderline NASH developed definite NASH
Fibrosis improved in 34% of the children but worsened in 23%
Progression was more likely with increasing ALT, increasing GGT, type 2 diabetes/increasing HgbA1c
Overall, one-third had histologic features of progression within 2 years, in association with increasing obesity and serum levels of aminotransferases and loss of glucose homeostasis.
The study conclusions are limited by selection bias, potential liver biopsy sampling errors, limited enrollment of non-Hispanic children, and relatively short duration of follow-up
A terrific review of sickle cell disease (SCD) associated liver problems: F Lacaille et al. JPGN 2021; 72: 5-10. The Liver in Sickle Cell Disease
While the most frequent liver-related problem in individuals is cholelithiasis (>25% after age 5 yrs), a host of other problems can develop –this article is a good reference.
~6% of children and 10% of adults develop severe liver complications of SCD
With sequestration, indications include pain with acute drop in hemoglobin (>2 g/dL)
Acute hepatic crisis is often signaled by elevated conjugated bilirubin
With severe liver disease/liver ischemia, authors advocated for exchange transfusion which “more efficiently decreases HbS percentage, faster restoring the blood flow than simple transfusion.” Consider after excluding biliary complication if INR is >1.4 with increased conjugated bilirubin (>3 mg/L). “Simple transfusion should be discussed in other cases.”
Cholangiopathy and autoimmune liver disease
Although autoimmune sclerosing cholangitis/autoimmune hepatitis are rare, it may account for 8% of children with SCD referred for hepatic dysfunction
Liver biopsy, needed for diagnosis, “is a dangerous procedure in SCD, which cannot be performed without at least a transfusion”
“Steroids can induce sickle crisis”
Look for ANA, SMA, LKM, and ANCA
Iron Overload
“It is not usually a significant concern in children…In our patients, the median ferritin level was about 3000 ng/mL, and none had a severe overload on MRI”
Infections/Drug toxicity
Need to consider hepatitis B, hepatitis C, and hepatitis E in particular
Inquire about herbal medicines and recreative drugs
Liver transplantation
Results are often poor.
Problems include sickle cell crisis in the transplanted liver, and drug toxicity which can add to the neurological and renal morbidities of SCD
Stem cell transplantation
Consider for severe complications of SCD including hepatic complications
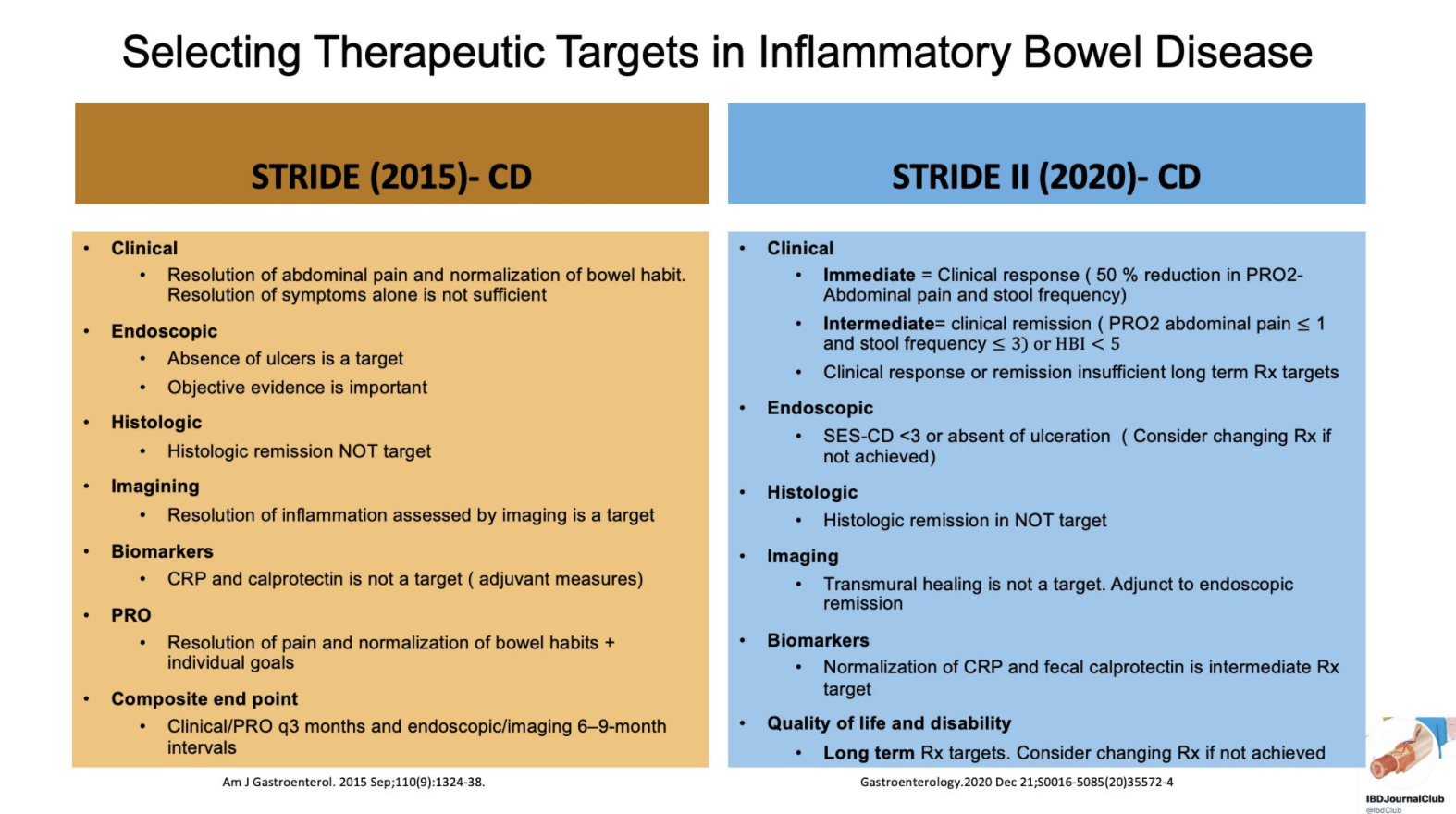
From Tauseef Ali’s Twitter Feed — a summary slide of Crohn’s disease targets for both pediatric and adult patients and a slide showing typical response/remission/healing times to medications.
Recommendations were based on a systematic review of the literature and iterative surveys of 89 IOIBD members, recommendations were drafted and modified in two surveys and two voting rounds.
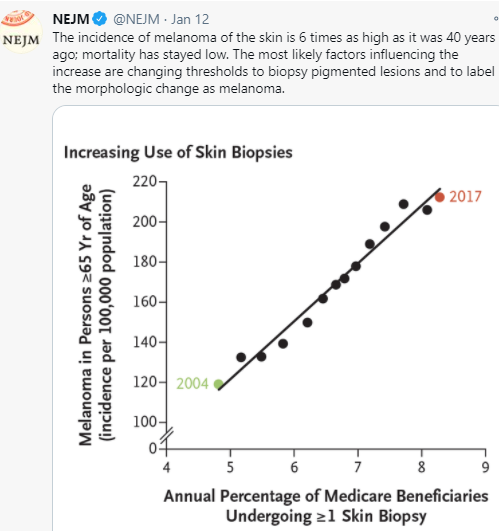
It would seem intuitive that screening for melanoma in at-risk pediatric patients would be worthwhile. And, this has been recommended in pediatric patients with inflammatory bowel disease who have received medications which increase the risk. However, a recent article (HG Welch et al. NEJM 2021; 384: 72-79. The Rapid Rise in Cutaneous Melanoma Diagnoses) provides a lot of reason to question this practice;. This article did not focus on pediatrics but its message about overdiagnosis of melanoma is applicable to this population as well.
Key points:
The increase in melanoma diagnosis (6-fold increase over 40 years) without a significant change in mortality (see Figure 4) indicates that the increase is primarily related to diagnostic scrutiny
This is driven by a fear of missing a diagnosis, medicolegal concerns and patient anxiety along with lower thresholds for referring to dermatology, lower thresholds for dermatologists to biopsy, and lower threshold by pathologists to diagnose melanoma
There are “no definitive diagnostic criteria for the pathological diagnosis of melanoma”
“The incidence of melanoma in situ is now 50 times as high as it was in 1975 (25 vs 0.5 per 100,000 population)…[yet there is a] lack of any appreciable effect in reducing the occurrence of invasive melanoma.”
Adverse consequences of unnecessary dermatology referrals: feeling vulnerable related to overdiagnosis of melanoma, increased costs, and difficulty obtaining life or health insurance
More “survivors” of melanoma overdiagnosis increase awareness of melanoma and can increase the cycle of overdiagnosis
My take: Routine visits to dermatology are difficult to justify in the absence of worrisome skin findings. “Although the conventional response has been to recommend regular skin checks, it is far more likely that more skin checks are the cause of the epidemic — not its solution.”
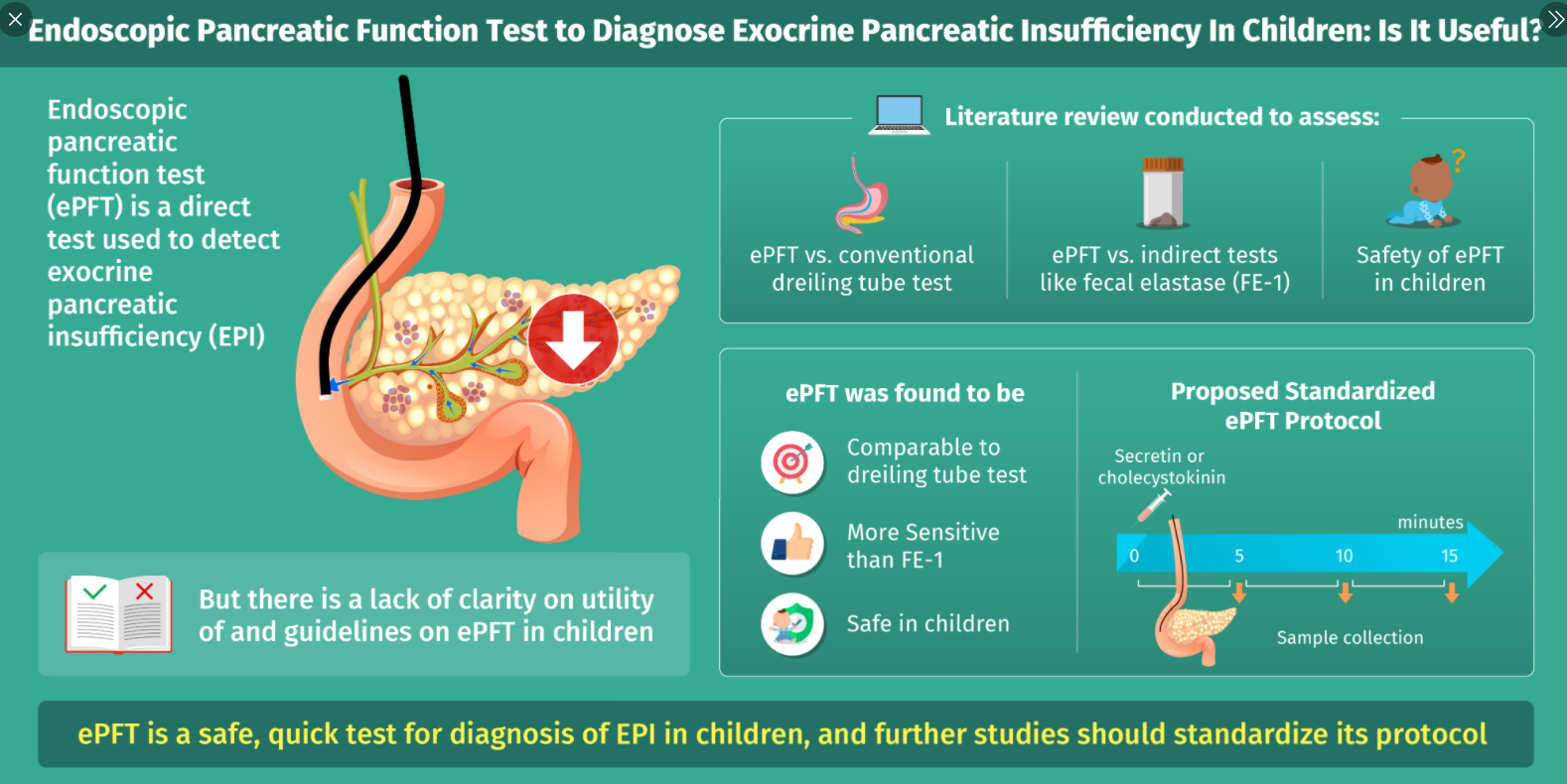
This articles serves as a good review of exocrine pancreatic insufficiency (EPI).
Etiologies:
“Cystic fibrosis is the most common cause of EPI in children .” Other congenital causes include aberrant embryonic development of the pancreas, “Shwachman-Diamond syndrome, Johanson-Blizzard syndrome, Pearson marrow pancreas syndrome, and Jeune syndrome”
“Acquired causes of EPI can be transient, such as in the aftermath of acute pancreatitis (which can persist weeks to months)”
Also, infants, compared to adults, have “physiological” EPI. Lipase output is 5–10% of adult values during the 1st 6 months of life.
Advantages/Disadvantages of Endoscopic Testing for EPI:
Advantages:
• Safe, technically easy, and quick procedure to perform in conjunction to routine investigative EGD
• Allows assessment of acinar and ductal function
• High sensitivity and specificity in detection of isolated and generalized enzyme deficiencies
• Can diagnose minor and more severe degrees of EPI and aid in early diagnosis of CP in patients with unremarkable radiological changes
Disadvantages:
• Can be done only in conjunction with EGD and the patient will likely require sedation• Prolongs routine EGD
• Assesses peak enzyme activity and bicarbonate concentrations rather than total secretory capacity
• No standardized pancreatic fluid collection frequency or duration in pediatrics
• Lack of age-specific standardized reference ranges in pediatrics
Endoscopic Testing Caveats:
Any sample with a pH less than 7 may be unreliable as it is below the pH optimum of the enzymes and may reflect contamination with gastric fluid; however, ” the inability to increase pH, or bicarbonate, upon secretin stimulation may be reflective of loss of cystic fibrosis transmembrane conductance regulator (CFTR) function”
My take: With careful clinical judgement, endoscopic EPI testing is rarely needed. First of all, fecal elastase measurements can detect most patients with EPI. In addition, a lot of patients with poor growth and suspected malabsorption are too young for reliable endoscopic EPI testing.
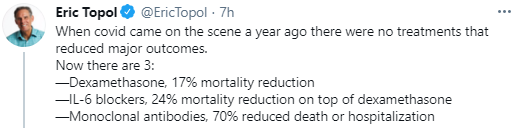
“For the Moderna study, researchers looked at blood samples taken from eight people who had received the recommended two doses of the Moderna vaccine. The findings are yet to be peer reviewed, but suggest immunity from the vaccine recognises the new variants. Neutralising antibodies, made by the body’s immune system, stop the virus from entering cells.
Blood samples exposed to the new variants appeared to have sufficient antibodies to achieve this neutralising effect, although it was not as strong for the South Africa variant as for the UK one. Moderna says this could mean that protection against the South Africa variant might disappear more quickly.”
Transabdominal ultrasound is recommended as a first-line noninvasive imaging modality for suspected AP
If ultrasound is negative for AP and an imaging diagnosis of AP is needed, either CT or MRI is recommended
“MRI, particularly MRCP, has also been shown to be more sensitive than CT for biliary etiologies of pancreatitis”
“In clinical practice, MRI is often used for assessment and monitoring of late complications of AP, such as fluid collections, to time and guide therapeutic interventions.”
Acute Recurrent Pancreatitis:
MRI is recommended to identify structural or obstructive causes for ARP
Chronic Pancreatitis:
MRI is the recommended modality for imaging of suspected CP
When imaging is needed to assess a suspected or known episode of AP in a child with CP, transabdominal ultrasound is the preferred first-line imaging modality
My take: This report provides a great deal of detail regarding the imaging modalities, terminology and diagnostic considerations for pediatric pancreatitis.