I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Table 1 provides a summary of the recommendations and indicates a threshold for which routine pre-procedure testing may not be needed:
“For endoscopy centers where the prevalence of asymptomatic SARS-CoV-2 infection is low (<0.5%), the AGA suggests against implementing a pretesting strategy.”
Conditional recommendation, very low certainty evidence
Rationale: “In low-prevalence settings, a pretesting strategy may not be informative for triage due to the high number of false positives, thus PPE availability may drive decision-making.”
My take: Particularly after the rollout of vaccination to health care providers, routine testing for SARS-CoV-2 is not likely to be needed once the prevalence drops to low levels.
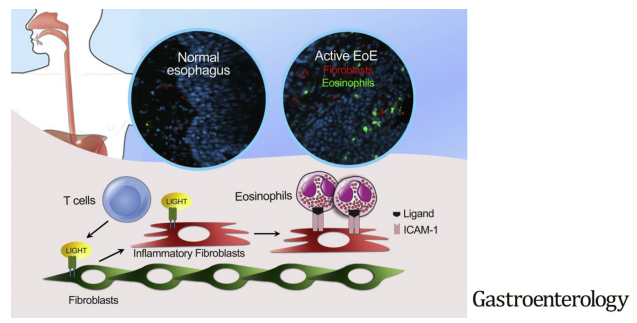
The authors investigated the effects of tumor necrosis factor superfamily member 14 (TNFSF14, also called LIGHT) on fibroblasts in EoE.
Key findings:
LIGHT was up-regulated in the esophageal tissues from patients with EoE, compared with control individuals
Stimulation of esophageal fibroblasts with LIGHT induced inflammatory gene transcription
My take: The authors show that patients with EoE had proinflammatory fibroblasts in the epithelium. Further, they show that eosinophil-fibroblast interaction was dependent on intact LIGHT signaling.
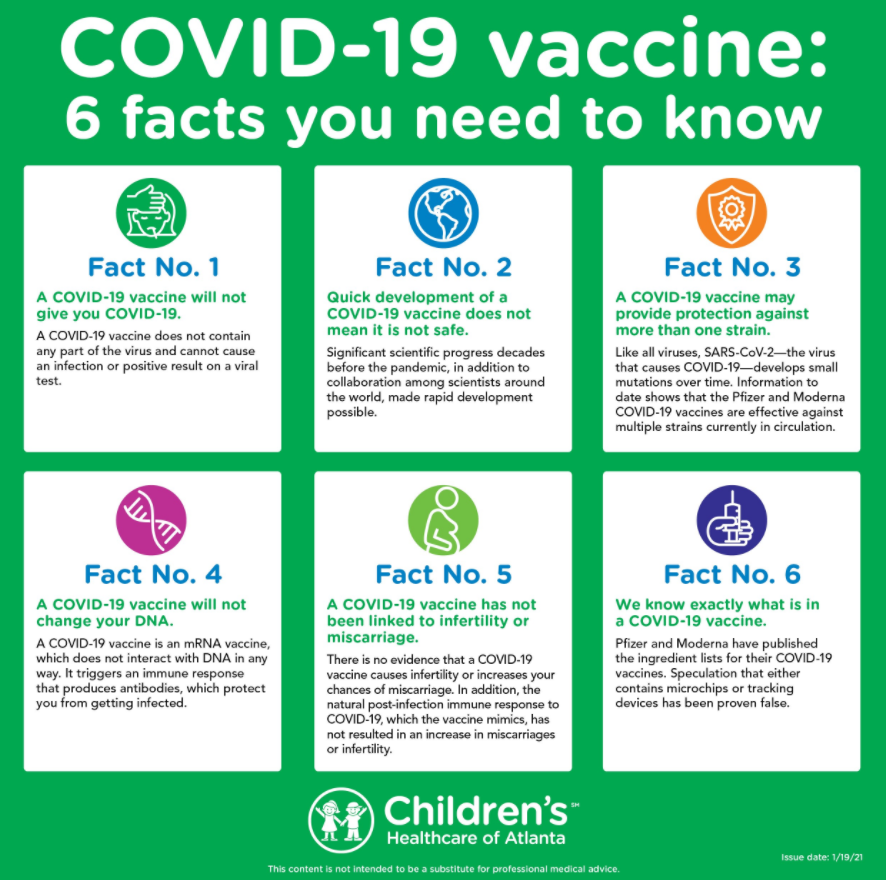
Yesterday, Evan Anderson (infectious disease) shared some updates on COVID-19 vaccines.
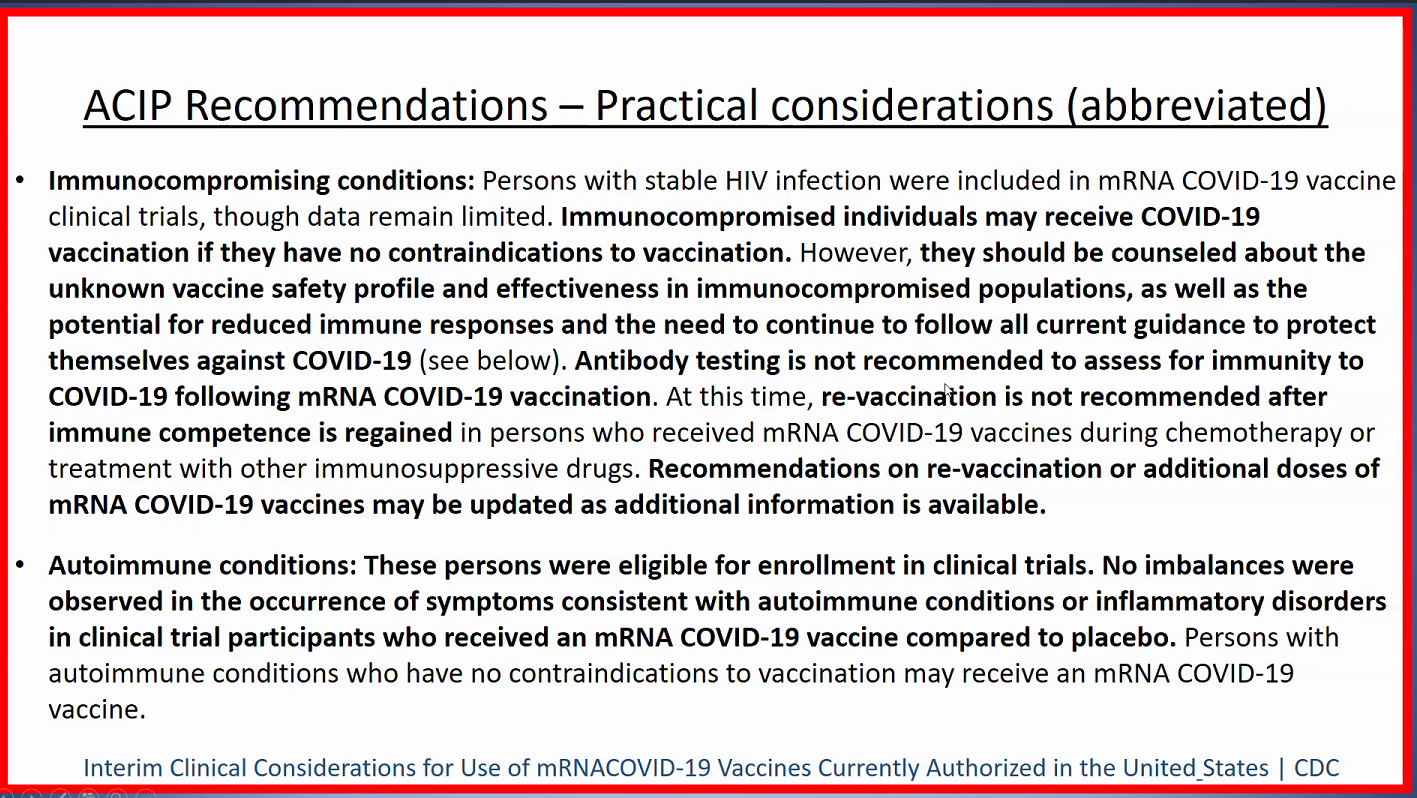
Dr. Anderson noted that more research is needed in children, pregnant women and immunocompromised populations. Immunocompromised patients may have a lower response rate to vaccination.
The South African 501Y.V2 COVID-19 variant may be less responsive to neutralization from donor plasma and the vaccines may be less effective in this variant.
He reviewed ACIP recommendations -available from CDC website as well
Dr. Anderson noted there is a good response to vaccination even in those with a lack of adverse effects with vaccination
Immunity after vaccination: data has been published showing good antibody levels at 3 months. Moderna has stated that they expect vaccine will provide immunity for at least a year
Immunity after infection with COVID-19: at least 3 months. Those with milder infection are more likely to get reinfected.
Antibody testing after vaccination to assess for immunity is not recommended
In the article, they note “the exception is for any live-attenuated virus vaccines or replication-competent viral vector vaccines that come to market.” Currently, all of the vaccines are inactivated (not live-attenuated).
These recommendations apply to approved populations which currently do not include pediatric patients or patients who are pregnant.
As noted in previous posts, I tend to favor isotonic IV fluids due to risk of hyponatremia with hypotonic fluids. A new study (below) indicates that some isotonic fluids are associated with an increased risk of electrolyte disturbances. Thanks to Ben Gold for this reference.
In this unblinded, randomized clinical trial with 614 children, participants were randomized to receive commercially available plasmalike isotonic fluid therapy (140 mmol/L of sodium and 5 mmol/L potassium in 5% dextrose) or moderately hypotonic fluid therapy (80 mmol/L sodium and 20 mmol/L potassium in 5% dextrose).
Key findings:
Clinically significant electrolyte disorder was more common in children receiving plasmalike isotonic fluid therapy:
Hypokalemia developed in 57 patients (19%) and hypernatremia developed in 4 patients (1.3%) receiving isotonic fluids; in total, this group had 61 of 308 patients [20%]) with electrolyte disturbance, compared with 9 of 306 patients [2.9%] of those receiving hypotonic fluid therapy (P < .001)
“Severe” hypokalemia (<3.0 mmol/L) was significantly more common in patients receiving isotonic fluid therapy 8 of 308 patients (2.6%) compared with 1 of 306 patients ( 0.3%) patients receiving hypotonic fluid therapy
My take: In the U.S., this suggests that fluids like lactated ringer’s which also has a low amount of potassium should not be routinely used. When choosing an isotonic fluid in children, D5 Normal Saline (0.9%) with added potassium may be more suitable..
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
A recent commentary (JM Perrin et al. NEJM 2020; 383: 2595-2598. Medicaid and Child Health Equity) describes what is happening with Medicaid and the Children’s Health Insurance Program (CHIP).
Key points:
Over the past 20 years, the proportion of pediatric health care coverage provided by Medicaid and CHIP has been increasing. In 1997, these programs represented about 15% of health care coverage compared to ~35% in 2018. This corresponds to reductions in employer-provided coverage
Unlike private insurance, Medicaid is always available as it doesn’t have fixed enrollment periods
State funding of Medicaid creates challenges. “States have routinely used strategies for limiting enrollment”
“Medicaid’s low physician payment rates, which average about two-thirds of rates paid by Medicare for the same services, depress physician participation…Lack of access to specialists poses additional problems in many communities”
The authors recommend the following:
Medicaid should be expanded to cover all children from birth through 21 years of age
The federal government should assume full financial responsibility
Medicaid payments should parallel national Medicare standards
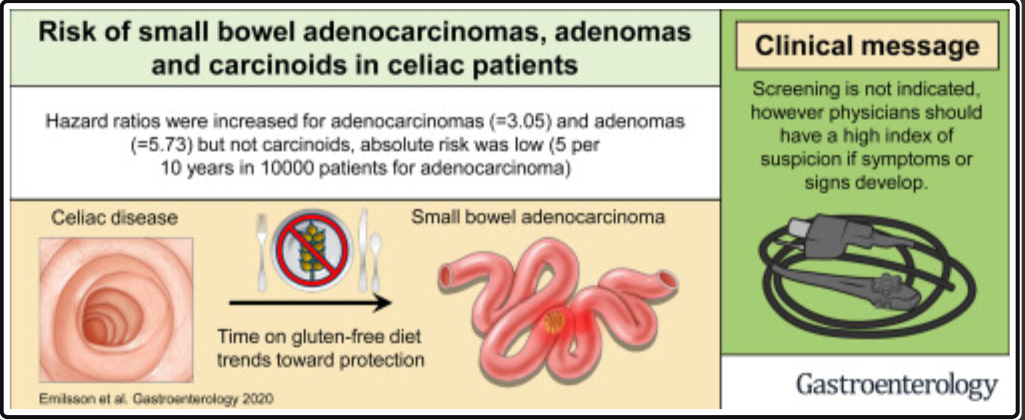
Beginning at 1 year after a diagnosis of CD, 29 patients (0.06%) received a diagnosis of small bowel adenocarcinoma vs 45 reference individuals (0.02%).
HRs were small bowel adenocarcinoma 3.05, carcinoids 0.59, and adenomas 5.73.).
Overall, there was 1 extra case of small bowel adenocarcinoma in every 2944 patients with CD followed for 10 years.
There was an inverse association between mucosal healing risk of future small bowel adenocarcinoma (HR, 0.18; 95% CI, 0.02–1.61), although the HR failed to attain statistical significance.
It is important to note that lymphoma is much more common malignancy than adenocarcinoma in celiacdisease. The authors, in their discussion, state: “compared with lymphomas, small bowel adenocarcinomas were approximately 10 times less common in patients with CD.” At the same time, with the discovery of milder cases of Celiac disease, lymphoma risk is not nearly as high as previously suggested. A large cohort study (Clinical Gastroenterology and Hepatology 2012; 10: 30-36) of ~45,000 did not see an increased risk of GI cancers beyond the first year after diagnosis. In addition, another study (Gastroenterology 2010; 139: 763), found that mortality NOT worsened in undiagnosed celiac disease (identified by review of serology) in Olmstead County, though bone density decreased. n=129 of 16,847. (?milder cases undiagnosed). Related post: Good News For Celiac Disease
My take (mostly borrowed from authors): There is a tiny increase in risk of “small bowel adenomas and adenocarcinomas in patients with diagnosed CD, but only a very marginal increase in terms of absolute risk. Our results do not imply a need for surveillance but celiac individuals with signs or symptoms of malignancy should merit further investigation for small bowel adenocarcinoma. Mucosal healing was strongly associated with lower risk of small bowel adenocarcinoma, although the association failed to reach statistical significance.’ Lymphoma is a more common malignancy associated with CD but the absolute risk remains low.
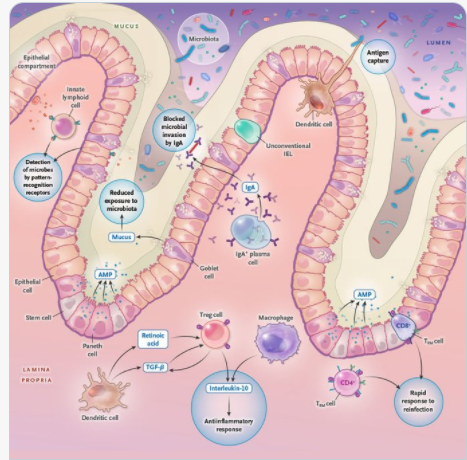
A recent review (JT Chang. NEJM 2020; 383: 2652-2664. Pathophysiology of Inflammatory Bowel Diseases) provides an in-depth description of the pathophysiology of inflammatory bowel disease (IBD). Digesting the article is akin to putting together a 1000 piece puzzle due to the complex interactions.
Some of the Key Points:
Based on genomewide association studies, there are “more than 240 risk variants that affect intracellular pathways recognizing microbial products (eg. NOD2); the autophagy pathway, which facilitates recycling intracellular organelles and removal of intracellular microorganisms (eg. ATG16L1); genes regulating epithelial barrier function (eg. ECM1); and pathways regulating innate and adaptive immunity (eg. IL23R and IL10).”
In this article, Figure 1 and 2 describe the intestinal mucosal immune system in health and disease. At baseline, this system promotes an antiinflammatory state “by virtue of active down-regulation of immune responses. For example, unlike macrophages in other parts of the body, intestinal macrophages do not produce inflammatory cytokines” after exposure to bacteria.
Other points:
Dysbiosis is present with IBD; however, studies have been “unable to infer causal relationships.”
Germ-free mice, when given fecal material from patients with IBD have increased susceptibility to colitis as compared to those who received fecal material from a healthy person.
Thus, this leads to potential for mitigating intestinal inflammation by modulation of the microbiome.
However, the authors note that humans are colonized by trillions of viral, fungal, bacterial, and eukaryotic microbes.
Other components of IBD pathophysiology: reduced mucus layer, increased microbial adherence, dysregulation of tight junctions/increased permeability, dysfunctional Paneth cells, TNF, IL23, IL12, IL6, IL 17A, IL17F, IL22, Interferon-gamma, integrins, JAK inhibitors, T-cells
My take: This article is a useful reference detailing the complexity of IBD pathophysiology and tries to summarize a whole textbook of information into 12 pages.
Key point: At 6 months after acute infection, COVID-19 survivors (n=1733 enrolled in study) were mainly troubled with fatigue or muscle weakness, sleep difficulties, and anxiety or depression. Patients who were more severely ill during their hospital stay had more severe impaired pulmonary diffusion capacities and abnormal chest imaging manifestations
NY Times (1/15/21): C.D.C. Warns the New Virus Variant Could Fuel Huge Spikes in Covid Cases “The new variant, called B.1.1.7, was first identified in Britain, where it rapidly became the primary source of infections, accounting for more than 80 percent of new cases diagnosed in London and at least a quarter of cases elsewhere in the country.”
Excluding those who died within the first 3 months, the 10‐year patient survival and graft survival rates were 92.6% and 77.1%, respectively, in the PSC with IBD (PSC‐IBD) group and 97.1% and 83.2% in the isolated PSC group, respectively.
The rate of recurrent PSC was 21% in the PSC‐IBD group and 11% in the isolated PSC group
Thus, it appears that having pre-existing IBD did not significantly influence survival after transplantation.