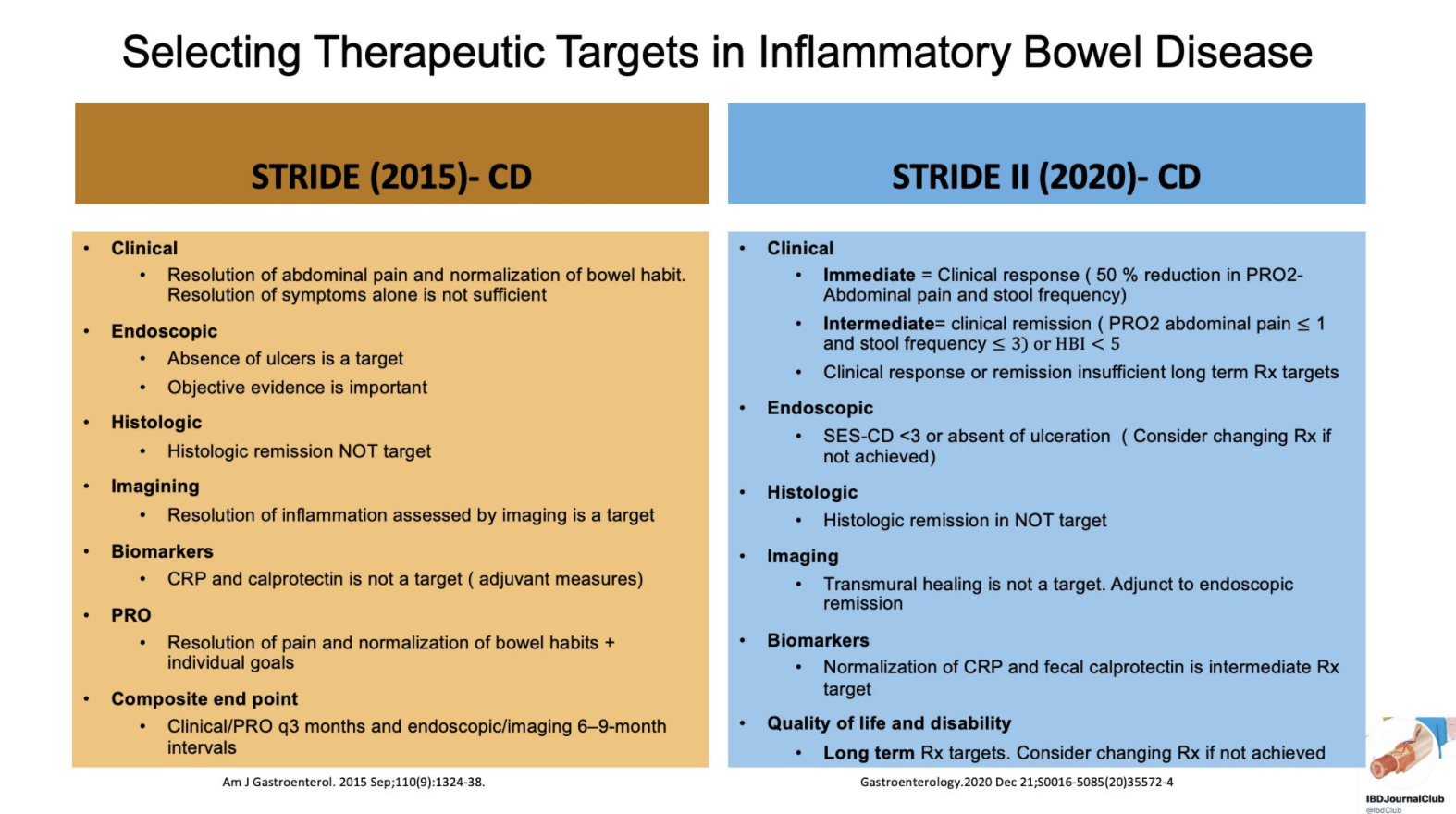
From Tauseef Ali’s Twitter Feed — a summary slide of Crohn’s disease targets for both pediatric and adult patients and a slide showing typical response/remission/healing times to medications.
Recommendations were based on a systematic review of the literature and iterative surveys of 89 IOIBD members, recommendations were drafted and modified in two surveys and two voting rounds.
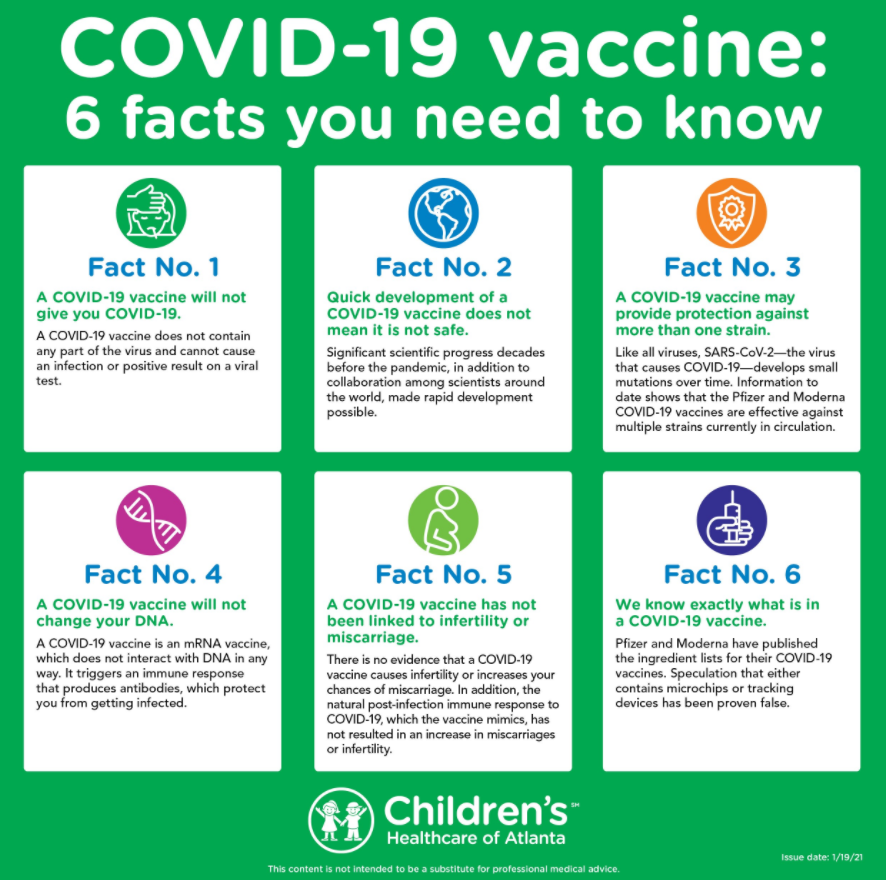
In the article, they note “the exception is for any live-attenuated virus vaccines or replication-competent viral vector vaccines that come to market.” Currently, all of the vaccines are inactivated (not live-attenuated).
These recommendations apply to approved populations which currently do not include pediatric patients or patients who are pregnant.
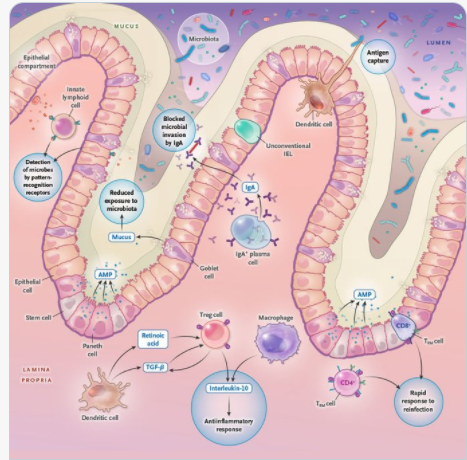
A recent review (JT Chang. NEJM 2020; 383: 2652-2664. Pathophysiology of Inflammatory Bowel Diseases) provides an in-depth description of the pathophysiology of inflammatory bowel disease (IBD). Digesting the article is akin to putting together a 1000 piece puzzle due to the complex interactions.
Some of the Key Points:
Based on genomewide association studies, there are “more than 240 risk variants that affect intracellular pathways recognizing microbial products (eg. NOD2); the autophagy pathway, which facilitates recycling intracellular organelles and removal of intracellular microorganisms (eg. ATG16L1); genes regulating epithelial barrier function (eg. ECM1); and pathways regulating innate and adaptive immunity (eg. IL23R and IL10).”
In this article, Figure 1 and 2 describe the intestinal mucosal immune system in health and disease. At baseline, this system promotes an antiinflammatory state “by virtue of active down-regulation of immune responses. For example, unlike macrophages in other parts of the body, intestinal macrophages do not produce inflammatory cytokines” after exposure to bacteria.
Other points:
Dysbiosis is present with IBD; however, studies have been “unable to infer causal relationships.”
Germ-free mice, when given fecal material from patients with IBD have increased susceptibility to colitis as compared to those who received fecal material from a healthy person.
Thus, this leads to potential for mitigating intestinal inflammation by modulation of the microbiome.
However, the authors note that humans are colonized by trillions of viral, fungal, bacterial, and eukaryotic microbes.
Other components of IBD pathophysiology: reduced mucus layer, increased microbial adherence, dysregulation of tight junctions/increased permeability, dysfunctional Paneth cells, TNF, IL23, IL12, IL6, IL 17A, IL17F, IL22, Interferon-gamma, integrins, JAK inhibitors, T-cells
My take: This article is a useful reference detailing the complexity of IBD pathophysiology and tries to summarize a whole textbook of information into 12 pages.
This study looked at 105 patients receiving combination therapy; the a median duration of combination therapy was 2.1 years, with infliximab and either methotrexate (53) or azathioprine (52). 89 patients had Crohn’s disease.
Key findings:
11 (10.5%) patients experienced a clinical relapse over a median duration of follow-up of 12.0 months after stopping the immunomodulator.
In the patients who did not relapse, the median IFX trough level at IM discontinuation was 6.2; the IFX trough level was 3.8 μg/mL in those who relapsed.
In their discussion, the authors urge caution in discontinuation of immunomodulators in those with clinically-severe Crohn’s disease and those with low infliximab levels.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
“Randomized controlled trials published more than a decade ago demonstrated that exclusive enteral nutrition, wherein all table foods are eliminated from a diet and the patient relies on an elemental diet alone for nutrition, was effective in not just inducing clinical remission but also improving inflammatory biomarkers.”
“More recent rigorous studies have demonstrated that the effects of exclusive enteral nutrition can be mimicked either by a selected, less-restrictive diet (such as CD-TREAT4), which is more sustainable, or by combining partial enteral nutrition with an elimination diet that is quite diverse (such as CDED5).”
“Exclusive enteral nutrition (EEN) has been studied the most rigorously of all diets in IBD and has demonstrated the greatest benefit, compared with other diet studies in IBD. EEN requires the intake of elemental, semi-elemental, or polymeric formulas to meet all nutritional requirements without additional intake of food for 6-8 weeks. Studies have been performed mostly in pediatric populations and have shown effectiveness in induction of remission with reduction in inflammatory markers, including C-reactive protein, erythrocyte sedimentation rate, and fecal calprotectin, and even mucosal healing. EEN has not worked out as well for adult populations, because of the poor tolerability of exclusive intake of enteral formulas.”
“Beyond EEN, there are many diets that have been considered … only the SCD and Crohn’s disease exclusion diets have shown improvement in clinical remission and reduction in inflammatory markers.”
“Most dietary studies are underpowered, lack a control arm, and do not include endoscopic endpoints. The current body of evidence remains insufficient to support the use of diet alone for the treatment of IBD.”
My take: Except for exclusive enteral nutrition (EEN) which is quite challenging, dietary therapies have not been proven as effective long-term stand-alone treatments. In patients who choose dietary therapy, careful monitoring is particularly important.
In this systematic review, a total of 995 adult patients were included from 18 observational studies (4 prospective and 14 retrospective), 1 nonrandomized controlled trial, and 1 subgroup analysis of a randomized controlled trial.
Key findings:
Biologic dose de-escalation was associated with relapse rates as high as 50% at 1 year. Overall, clinical relapse occurred in 0%–54% of patients who dose de-escalated biologic therapy (17 studies).
Lower rates of relapse (10%–25%) were reported in studies involving patients with endoscopic and/or histologic remission
These results are in agreement with a previous meta-analysis, which found a 1-year risk of relapse after discontinuation of anti-TNF therapy of 36% in CD and 28% in UC ( Gisbert JP, et al.. Am J Gastroenterol 2016;111:632–47).
My take: This study shows that dose de-escalation of biologic therapy in IBD seems to be associated with high rates of clinical relapse
In this national multicenter retrospective cohort study in 207 adult patients with either active or inactive perianal Crohn’s disease (pCD) who received ustekinumab (2017-2018). The majority had received multiple biologics (~85% had at least 2 anti-TNF agents, 28% had received vedolizumab) and prior anal surgeries (mean 2.8).
Methods: Success of ustekinumab was defined by (i) clinical success at 6 months of treatment assessed by the physicians’ judgment, with (ii) no need for dedicated medical treatment for perianal lesions (antibiotics and/or topics) nor (iii) unscheduled surgical treatment. For perianal disease evaluation, clinical success was defined in the study protocol, by the absence of draining pus for fistulas, and no anal ulcers
Key findings:
In patients with active pCD, success was reached in 57/148 (38.5%) patients.
Among patients with setons at initiation, 29/88 (33%) had a successful removal.
In patients with inactive pCD at initiation, the probability of recurrence-free survival was 86.2% and 75.1% at weeks 26 and 52, respectively.
The absence of ustekinumab optimization was associated with upper odds of success (OR 2.74). “We can suppose in our present study that optimization of treatment was needed in severe refractory patients with no or insufficient response to ustekinumab. Thus, in these nonresponders, success was not achieved despite optimization.”
My take (partly borrowed from authors): “This large multicenter dedicated study adds substantial evidence to the growing literature on ustekinumab effectiveness in refractory CD.” For pCD, optimization of ustekinumab has a low likelihood of improving response.
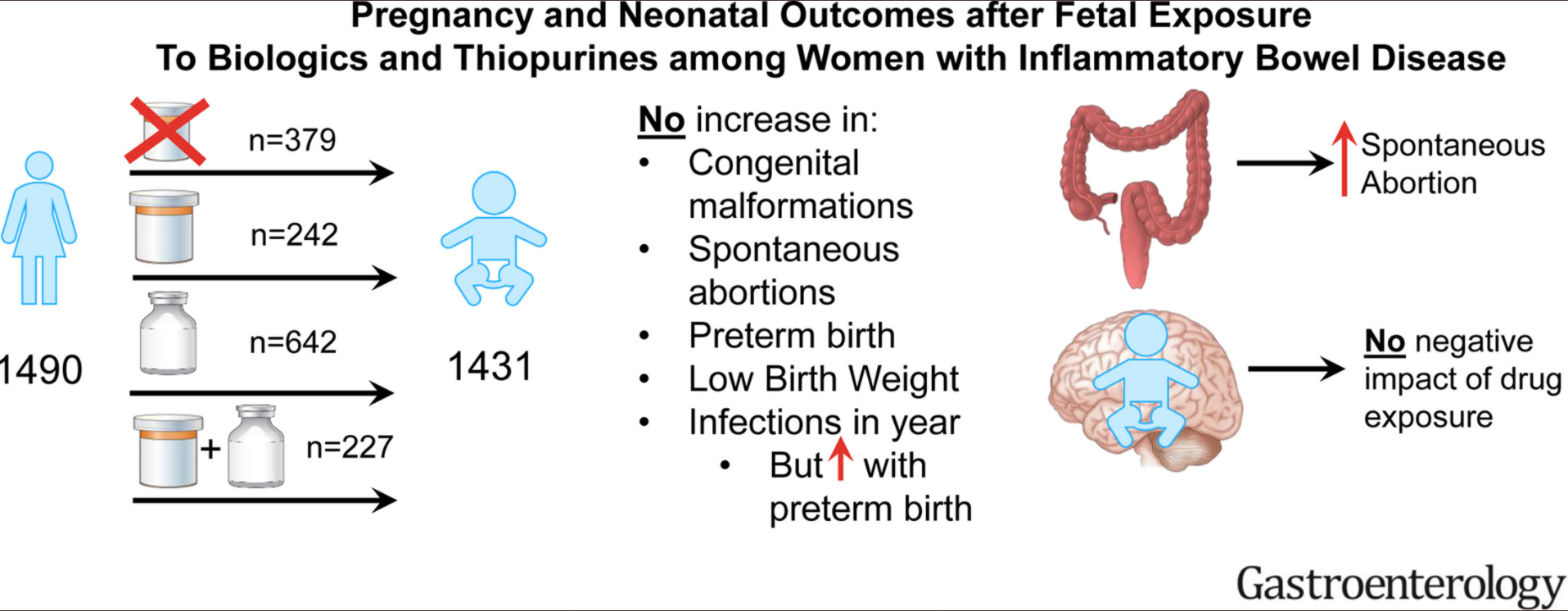
Methods: Between 2007 and 2019, pregnant women with IBD were enrolled in a prospective, observational, multicenter study across the United States (PIANO registry).
Key findings:
Exposure was to thiopurines (242), biologics (642) or both (227) versus unexposed (379)
Medication exposure did not increase the rate of congenital malformations, spontaneous abortions, preterm birth, LBW, and infections over the first year of life
Higher disease activity was associated with risk of spontaneous abortion (HR 3.41, 95% CI 1.51-7.69) and preterm birth with increased infant infection (OR 1.73, 95% CI 1.19-2.51)
My take: This study provides some reassurance that treatments for IBD are unlikely to affect neonatal outcomes; however, increased IBD activity does affect outcomes
This randomized study with 28 children with acute severe ulcerative colitis (ASUC) (PUCAI > /= 65) tried to determine if antibiotics with IV corticosteroids resulted in improved outcomes compared to IV corticosteroids alone. Most in the antibiotic group received the following for 3 weeks:
Vancomycin 250 mg 4/day (if less than 8 years, then 125 mg 4/day)
Amoxicillin 50 mg/kg/day divided into 3/day dosing (max 500 mg/dose)
Doxycycline 2 mg/kg/dose 2/day (children less than 7 years rec’d ciprofloxacin 10 mg/kg 2/day -max 250 mg/dose)
Key findings:
The mean day-5 PUCAI was 25 ± 16.7 in the abx/steroid combination group vs 40.4 ± 20.4 in the steroid monotherapy group (P = 0.037)
Median calprotectin values were lower in the abx combination group at day 5 (1202 vs. 2170, P=0.24) and at discharge (1210 vs 1840, P=0.695)
The need for 2nd line rescue therapy was low in both groups: 19% in abx group and 17% in the steroid group
Within 1 year, 3/16 (19%) in the abx combination group had had a colectomy compared with 2/12 (17%) in the steroid monotherapy.
The authors found no correlation between microbial features/microbiome at admissioin and clinical response 5 days later
In their discussion, the authors note that if antibiotics had a treatment benefit as high as 30% in avoiding second-line treatment (ie, 14% in intervention arm), “randomization of 1228 children would be required to show such a difference with a power of 80%.”
My take: I agree with the authors who state that “antibiotics cannot be routinely recommended until larger studies demonstrate a reduced need for second-line treatment or colectomy.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
Methods: Participants (n=78, ages 6-17 years) in this study were part of the PAILOT trial; they were naïve to biologic therapy with moderate to severe Crohn’s disease. This was a randomized controlled trial aimed to evaluate proactive vs reactive therapeutic drug monitoring in children with Crohn’s disease (CD) treated with adalimumab.
Key findings:
There was no significant difference in the rates of sustained corticosteroid-free clinical remission (25/34, 73%, vs 28/44, 63%; P = 0.35) or sustained composite outcome of clinical remission, C-reactive protein ≤0.5 mg/dL, and calprotectin ≤150 µg/g (10/34, 29%, vs 14/44, 32%; P = 0.77) between the combination group and the monotherapy group, respectively.
Adalimumab trough concentrations and immunogenicity were not significantly different between groups. The rate of serious adverse events was not significantly different between groups but was numerically higher in the monotherapy group. The monotherapy group had three patients undergo ileo-cecal resection.
The discussion reviews a number of studies that have compared combination and monotherapy. One key point is that this study enrolled children who were naïve to biologic therapy; thus, combination therapy may be more useful in those who have failed a previous biologic, particularly if the loss of response was immune-mediated.
My take: This study indicates that combination therapy is likely not routinely needed in children who start adalimumab and who are naïve to biologic therapy. Another finding of interest is the relatively low sustained composite outcome of clinical remission, approximately 30; this outcome combined clinical remission with biological markers. ~30%
“We found histologic evidence of UC activity (Geboes score ≥ 2B.1) in biopsies from 182 patients (65%) and endoscopic evidence of UC activity in 149 patients (53%) (substantial agreement, κ = 0.60).”
“Histologic features of UC activity were associated with increased rates of systemic corticosteroid use, colectomy, and hospitalization in the entire cohort (P < .05 for all) and associated with increased rates of systemic corticosteroid use in an analysis limited to patients in endoscopic remission (P < .001).”
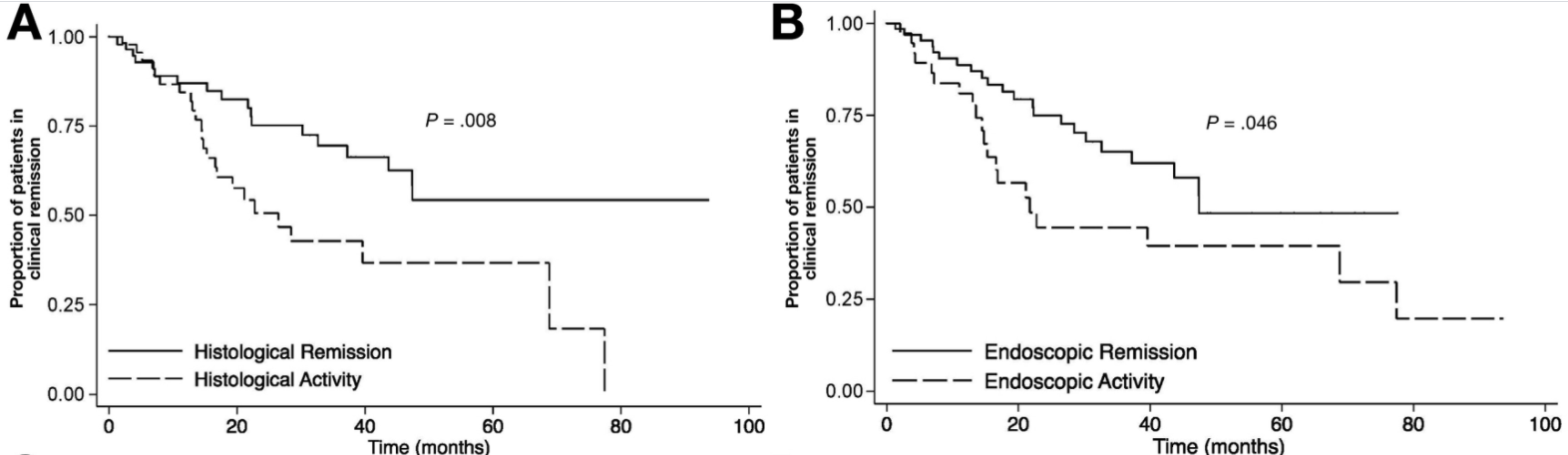
At ileo-colonoscopy, 63% of patients had endoscopic healing and 55% had histologic evidence of healing. The level of agreement between endoscopic and histologic activity was fair (62%, K = 0.2250, P = .0064)
On multivariate analysis, only histologic healing was associated with decreased risk of clinical relapse (hazard ratio [HR], 2.05; 95% CI, 1.07–3.94; P = .031), medication escalation (HR, 2.17; 95% CI, 1.2–3.96; P = .011), and corticosteroid use (HR, 2.44; 95% CI, 1.17–5.09; P = .018).
Kaplan-Meier analysis of effect of endoscopic and histologic activity on (A) clinical relapse-free survival versus histologic healing, (B) clinical relapse-free survival versus endoscopic healing
D Kevans et al. Inflamm Bowel Dis 2020; 26: 1722-1729. Histological Markers of Clinical Relapse in Endoscopically Quiescent Ulcerative Colitis Key finding: In endoscopically quiescent UC (n=76), active histological inflammation …[is] adjunctive histological marker associated with increased likelihood of disease relapse. The associated editorial (1730-32 by Asher Kornbluth) quotes Voltaire: “A wise Italian says that the best is the enemy of the good.” He notes that there is “a very real risk of abandoning an effective drug while chasing the goal of some yet to be universally defined histologic remission.” Currently organizational guidelines (ACG, AGA, ECCO, IOIBD) do NOT suggest the use of histologic normalization as an endpoint at this point.
My take: These studies show that histologic healing in ileal Crohn’s disease and in ulcerative colitis are associated with better outcomes that endoscopic appearance. However, there are a lot questions because many patients, possibly a majority, will not achieve histologic healing despite aggressive treatment. Related technical issues include how many biopsies are needed to assess histology and having a validated histologic assessment.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.