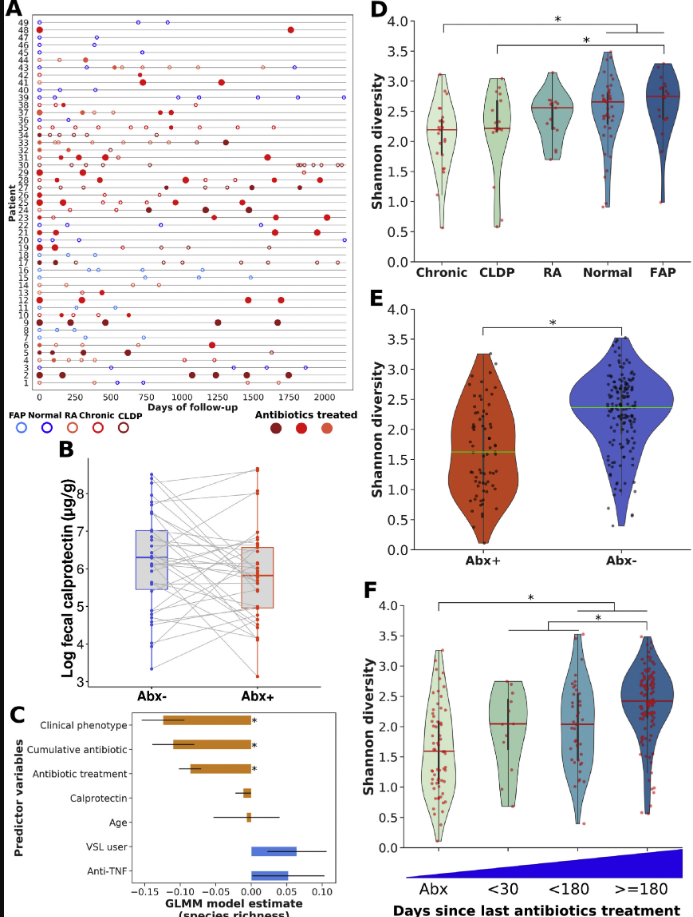
A prospective study (V Dubinsky et al. Gastroenterol 2020; 158: 610-24) followed 49 patients who had undergone pouch surgery for ulcerative colitis or for familial adenomatous polyposis (FAP).
The authors followed multiple parameters including calprotectin, metagenomes/bacterial diversity, antibiotic resistance testing, and virulence factors/toxins. 33 patients received antibiotics for a median of 425 days. Most patients were treated with a combination of ciprofloxacin and metronidazole.
Full text link: Predominantly Antibiotic-resistant Intestinal Microbiome Persists in Patients With Pouchitis Who Respond to Antibiotic Therapy
Key findings:
- Pouch phenotype: normal from UC (n=10), recurrent acute pouchitis (n=6), chronic pouchitis and Crohn’s-like disease of the pouch (n=27), and normal from FAP (n=6)
- 79% of antibiotic-treated patients had a clinical response to each course of antibiotics
- 89% of those who completed a 4-week course relapsed within 3 months
- Median calprotectin values decreased by 40% in response to antibiotics
- Antibiotic treatment reduced disease-associated bacteria including Clostridium perfringens, Ruminococcus gnavus, and Klebsiella pnneumoniae. However, F prausnitzii, a putative anti-inflammatory species, also decreased during antibiotic treatment
- While antibiotic resistance was noted, these strains had a tendency toward lower potential for virulence and “did not induce secretion of inflammatory cytokines by epithelial cells”
Why do patients become antibiotic-dependent?
“We observed a drastic shift in microbiome composition on antibiotics cessation, characterized by blooms of nonintestinal bacteria, especially those originating from the oral cavity, as well as of opportunistic pathogens. Intestinal colonization by oral bacteria has been associated with UC and Crohn’s disease, and shown to trigger severe intestinal inflammation in germ-free mice…[this] drug-resistant microbiome may be fragile and unable to prevent colonization by exogenous bacteria that are ecologically fitter once antibiotics are discontinued.”
My take: This study provides insight into how antibiotics improve pouchitis; namely, they reduce disease-associated bacteria and promote an antibiotic-resistant microbiome with lower inflammatory potential.
Related blog posts:
- IBD Briefs August 2019
- Pouchitis -Not So Rare in Patients with FAP
- IPAA (Pouch) for Crohn’s Disease and Indeterminate Colitis
Figure 1:
Link: 34 AAP Publications regarding COVID-19 and children