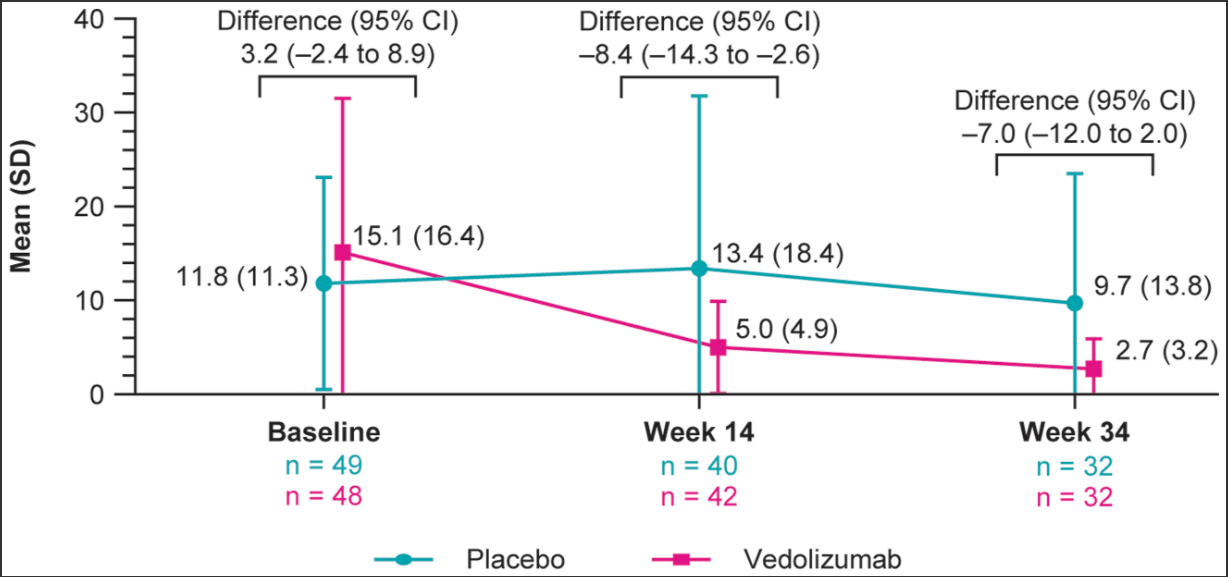
Methods: EARNEST, a randomized, double-blind, placebo-controlled study, evaluated vedolizumab efficacy and safety in adults with chronic pouchitis.
Key findings:
More patients treated with vedolizumab vs placebo achieved mucosal healing, reduction in ulcers and ulcerated pouch area and SES-CD remission.
Reduction in the Number of Ulcers was much better for Vedolizumab than PlaceboProportion of patients with (A) change in ulcerated surface area and (B) with no ulcers (ulcers >5 mm, erosions ≤5 mm)
My take: Fortunately, chronic pouchitis is uncommon in the pediatric population. This study shows that many patients with chronic pouchitis improve with vedolizumab.
Methods: Children (n=936) aged 5–16 years with suspected non-perforated appendicitis (based on clinical diagnosis with or without radiological diagnosis) were randomly assigned (1:1) to the antibiotic or the appendectomy group. Treatment failure: Within 1 year of random assignment, n the antibiotic group, failure was defined as removal of the appendix, and in the appendectomy group, failure was defined as a normal appendix based on pathology.
Key findings:
Treatment failure occurred in 153 (34%) of 452 patients in the antibiotic group, compared with 28 (7%) of 394 in the appendectomy group
There were no deaths or serious adverse events in either group
The relative risk of having a mild-to-moderate adverse event in the antibiotic group compared with the appendectomy group was 4·3
My take: Appendectomy was superior to antibiotic management of acute non-perforated appendicitis.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: This study aimed to identify biomarkers by conducting a Danish nationwide genome-wide association study (GWAS) on severe vs less severe ulcerative colitis.
Methods: Severe ulcerative colitis: Patients with severe ulcerative colitis were defined as having at least 1 major ulcerative colitis–related operation, at least 2 ulcerative colitis–related hospitalizations exceeding 2 days, and/or use of at least 5000 mg of systemic corticosteroids within 3 years of diagnosis
The authors utilized two source populations
The Center for Molecular Prediction of Inflammatory Bowel Disease (PREDICT) neonatal blood spot cohort (NBS) includes individuals born in Denmark and diagnosed with ulcerative colitis from 1981 to 2022
The North Denmark Biobank study is a population-based cohort of patients from Northern Denmark with inflammatory bowel disease from 1978 to 2020 (NorDIBD)
The combined cohort included 4491 patients (4153 from NBS and 338 from NorDIBD) with a mean (SD) age at diagnosis of 23.3 (8.4) years; 53% of patients were female and 27% had severe disease.
Key findings:
The association with HLA-DRB1*01:03 (Figure 1) had an OR of 6.38 for major operation, OR of 5.24 for at least 2 hospitalizations, and OR of 2.30 for use of at least 5000 mg of systemic corticosteroids in carriers vs noncarriers
Carriage of HLA-DRB1*01:03 allele was 2.8% in these cohorts
Limiation: Danish cohort -may not be applicable to other populations
My take: HLA-DRB1*01:03 is a low-frequency allele, carriers have a significantly higher risk of severe ulcerative colitis.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
E Park. NEJM 2025; DOI: 10.1056/NEJMp2501855. Medicaid on the Chopping Block
An excerpt:
A top priority for Congress and President Donald Trump is extending and expanding tax cuts expiring at the end of 2025…Republican leaders in the House intend to make at least $880 billion in Medicaid cuts over 10 years to offset some of the tax cuts’ $4.5 trillion cost…
Medicaid, however, is more essential than it has ever been. It provides affordable, comprehensive health coverage to more than 72 million low-income Americans1…Medicaid covers about 40% of all children and births in the United States. It covers more than one third of people with disabilities and 44% of children with special health care needs…
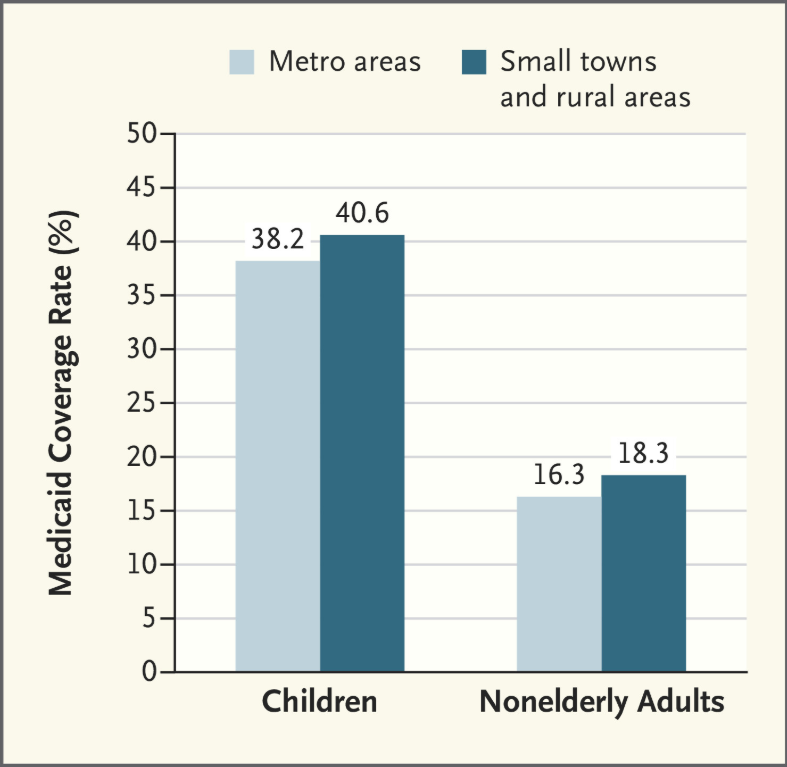
Medicaid is especially vital for rural communities. Residents of small towns and rural areas disproportionately rely on Medicaid…
Under many of these proposals, states would face drastic reductions in federal Medicaid funding….states would have to choose among three painful options. They could dramatically raise income and sales taxes. They could deeply cut other parts of their budgets, such as budgets for K–12 education and higher education, which account for about 43% of states’ own spending. Or — the option most states would have to choose — they could slash their Medicaid programs by substantially narrowing Medicaid eligibility, restricting benefits, making it harder for eligible people to enroll in and renew coverage, and making sharp cuts to already low reimbursement rates for hospitals, physicians, and nursing homes.
As a result, many low-income children, parents, people with disabilities, older adults, and others would be at risk for becoming uninsured and forgoing needed care…As opposition becomes increasingly public, widespread, and vocal, congressional Republican leaders could ultimately view severe Medicaid cuts as too politically difficult and decide they need to drop them from budget reconciliation.
My take: This article elaborates on all the ways that Congress could curtail Medicaid spending. Ultimately, all of them will leave the states with additional costs if they are to maintain current coverage levels. Even with the proposed cuts to Medicaid, the tax cut plan is projected to add two trillion dollars each year during this administration.
Related article: 3/2/25 Patricia Murphy, AJC: Medicaid cuts from Washington would gut this Georgia pediatrician’s practice (behind paywall) “A South Atlanta pediatrician [Dr. Dorsey Norwood] says 85% of her patients are covered by government health care program…For at least one Georgia pediatrician, cutting Medicaid benefits for her young patients would leave a wound in her practice that even she couldn’t heal.”
MT Fioretti et al. J Pediatr Gastroenterol Nutr. 2025;80:300–307. A decade of real-world clinical experience with 8-week azithromycin–metronidazole combined therapy in pediatric Crohn’s disease
Methods: This retrospective study over 10 years examined the efficacy of azithromycin-metronidazole for induction treatment in 44 children. All patients were given metronidazole (15–20 mg/kg/day two times daily, maximum of 1000 mg/day) administered daily for 8 weeks and azithromycin (7.5 mg/kg to a maximum of 500 mg/once a day) administered 5 days per week for the first 4 weeks, followed by 3 days per week for the final 4 weeks as per the initial publications.17, 18
Key findings:
After 8 weeks, the overall remission rate was 64%.
Of the 38 patients who completed the CD AZCRO course, 28 patients (74%) entered remission (Group 1) and 10 (26%) did not (Group 2)
After 8 weeks, Group 1 showed improved CRP levels and higher albumin and hemoglobin levels than Group 2. Median FC declined significantly from 650 mcg/g at baseline to 190 mcg/g at Week 8 in Group 1 (p < 0.001).
The authors conclude that “a combination treatment of azithromycin and metronidazole represents an alternative induction therapy for mild to moderate pediatric CD, offering benefits in terms of cost and practicalities compared to EEN and in side effects compared to steroids.”
My take: There are a small number of children with mild Crohn’s disease who could benefit from this induction regimen. An alternative would be the use of a more modest dietary approach (eg. Mediterranean diet)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: Hypermobility spectrum disorders (HSD) and hypermobility Ehlers–Danlos syndrome (hEDS) are frequently associated with gastrointestinal symptoms, although the underlying mechanisms remain unclear. Since recruitment occurred before the 2017 criteria for hEDS were established, it was not possible to distinguish between HSD and hEDS.
Methods: Retrospective review of all patients (>18 yrs) referred t for gastrointestinal motility evaluation and undergoing ADM were consecutively included from 2009 to 2023. This included 239 patients (50 HSD/hEDS and 189 non-HSD/hEDS). The HSD/hEDS group showed a lower BMI and higher use of enteral feeding than the control group (p < 0.001 and p = 0.026, respectively). This group was also younger, with a mean age of 30.4 ± 11.1 years versus 45.3 ± 15.4 years (p < 0.001).
Key findings:
The prevalence of antroduodenal dysmotility was not different between both groups, but enteric dysmotility was less common in the HSD/hEDS group (13% vs. 34%, p = 0.006).
There were similar percentages of delayed gastric emptying than non-HSD/hEDS patients; delayed gastric emptying was highly prevalent in both groups, 85% in patients with HSD/hEDS and 94% in non-HSD/hEDS patients
There were no differences in predominant symptoms between patients with and without HSD/hEDS.
In the discussion, the authors note that the lower rate of dysmotility combined with higher rates of enteral nutrition indicate that “factors like visceral hypersensitivity and autonomic function could be relevant in this context.”
My take: Most patients at this referral center had delayed gastric emptying. However, Ehlers-Danlos patients, in fact, had lower rates of enteric dysmotility.
“Health insurers process more than five billion payment claims annually, federal figures show. About 850 million are denied, according to calculations by appeals company Claimable, based on data from health-policy nonprofit KFF and the Centers for Medicare and Medicaid Services. Less than 1% of patients appeal.
Few people realize how worthwhile those labors can be: Up to three-quarters of claim appeals are granted, studies show…”
The author then details how one man overcame a denial to receive a life-saving liver transplantation and how a family helped their child receive immunoglobulin therapy for her neurologic condition. However, this only occurred after numerous appeals and after letters to the Georgia governor and Georgia attorney general.
Excerpts from the second article:
“Here are five things you can do to appeal a denied health-insurance claim.
1. Read up
Know what your plan covers. A good place to start is the summary of benefits and coverage. More detailed information should be available from your employer or insurer, which can provide a more in-depth document sometimes called the “evidence of coverage.” Check to make sure a denial met your insurer’s own rules. These policies are generally available online.
2. Take note
Log dates of calls to your insurer and whom you spoke to. Save paperwork including billing codes for denied services. And act quickly: Insurers have deadlines to file appeals.
3. Fight back
Call your insurer at the number on the back of your insurance card and ask why treatment wasn’t covered. You can ask how to file an appeal. If you have a denial or explanation of benefits letter, look for the section explaining appeals.
4. Get help
State assistance programs and nonprofits including the Patient Advocate Foundation and the Medicare Rights Center can help craft appeals. A startup called Claimable is trying to use technology to smooth the process. You can hire an advocate, looking through a directory or a third-party company, Solace Health. The nonprofit Dollar For helps with hospital bills. You can also ask your doctor’s office or hospital to appeal for you, and try to ensure they keep you in the loop on their communications.
5. Escalate
After you determine why your insurer denied a claim, you can write a letter explaining why the rejection wasn’t warranted. Your doctor can write a letter explaining why care is medically necessary. Pertinent medical studies can strengthen your case. Request the “designated record set” relevant to your case.
If your appeal is rejected, you can often appeal to a higher authority within the insurer. If that fails, you can generally appeal to a third party, often an independent review organization or a government-administered program. Your rejection letter or state insurance department should explain those steps. Practices vary state by state. You can also escalate your appeal to an administrative law judge.”
FDA IBD Workshop -Take-Home PointsOff-label does not equate to experimentalFDA Statement: The FD&C Act does not, however, limit the manner in which a physician may use an approved drug. Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling. Such “unapproved” or, more precisely, “unlabeled” uses may be appropriate and rational in certain circumstances, and may, in fact, reflect approaches to drug therapy that have been extensively reported in medical literature
Twenty-eight studies involving 153,027 patients with IBD were included.
Key findings:
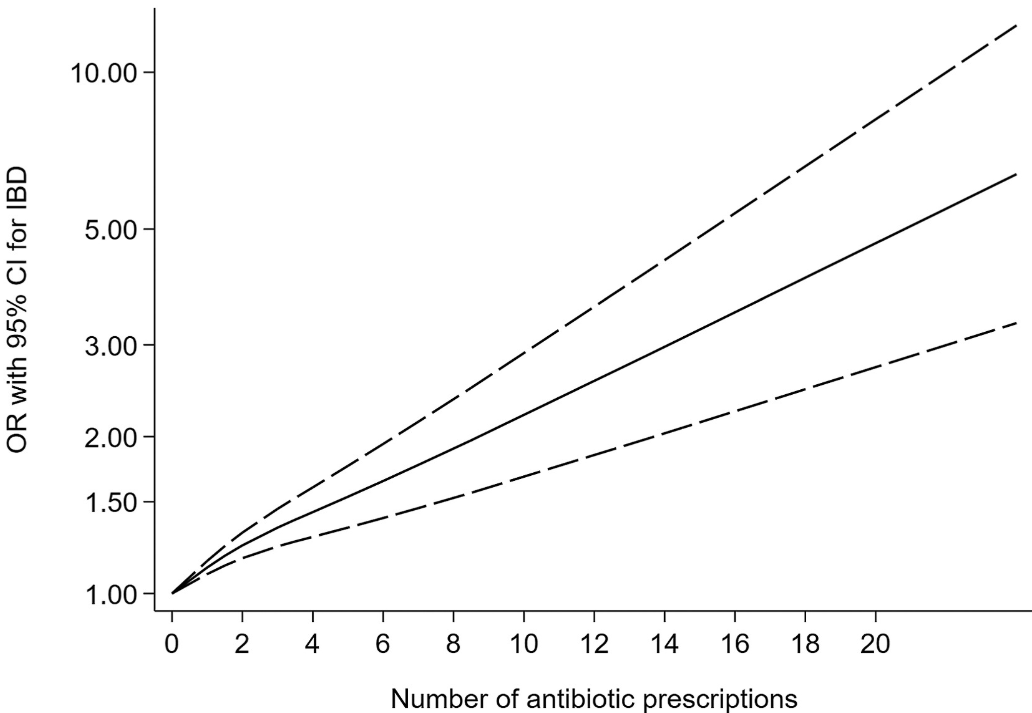
Antibiotic exposure was significantly associated with an increased risk of new-onset IBD for prescription-based studies (pooled OR, 1.41; 95% CI, 1.29–1.53) and for questionnaire-based studies (pooled OR, 1.35; 95% CI, 1.08–1.68). ‘
This association existed for both Crohn’s disease and ulcerative colitis, as well as in children and adults for prescription-based studies.
Some of the limitations:
There was statistical heterogeneity was high in the primary analysis, possibly because of inconsistencies in study design
Most studies included a clear lag time, yet an inadequate lag time still creates the possibility of reverse causality.
The authors could not disentangle the risk of antibiotics from the risk of infection in leading to the development of IBD.
Nonlinear dose-response relationship between antibiotic exposure and risk of new-onset IBD (solid black line and short dash black line represent estimated ORs and corresponding 95% CIs of nonlinear relationship)
My take: This is another study showing an association between antibiotic use and new-onset IBD. While this study does not prove causation, it is another reason for good antibiotic stewardship.
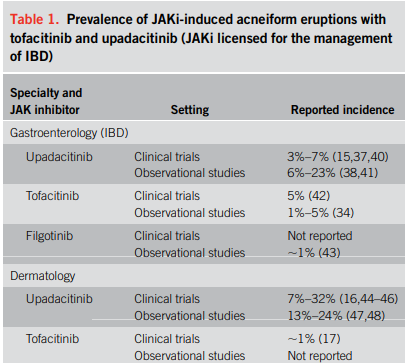
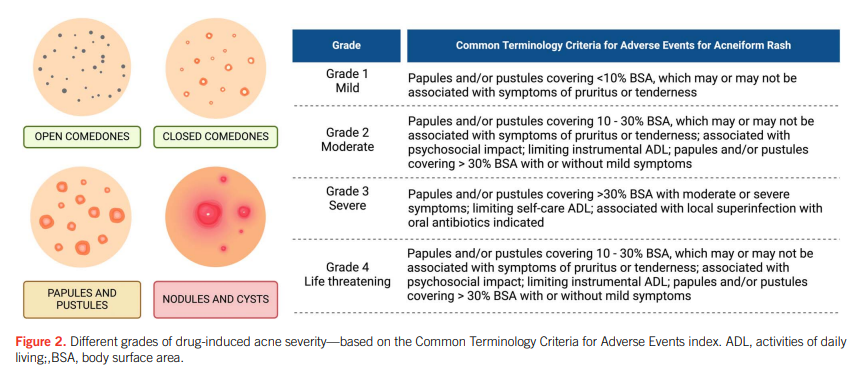
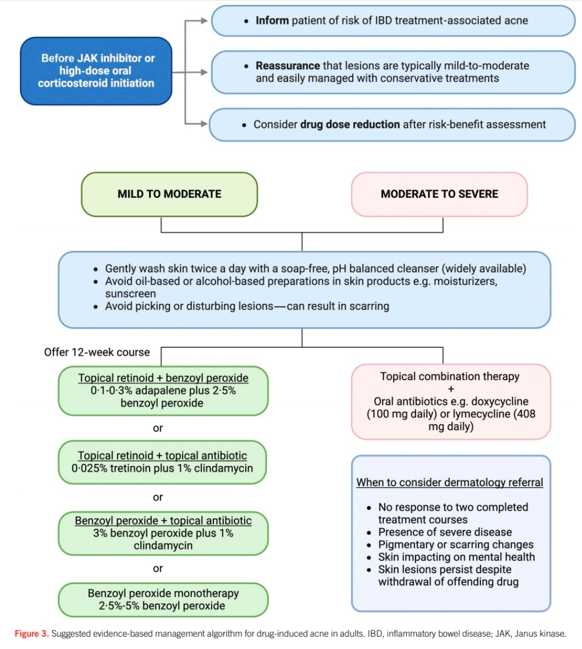
“Corticosteroids and Janus kinase inhibitors (JAKi) are commonly used for the treatment of inflammatory bowel disease (IBD) and are known to aggravate a prior tendency to acne or trigger the development of new acneiform eruptions. Both randomized controlled trials and real-world studies have identified acne as one of the most common treatment-emergent adverse events in JAKi… This review examines the characteristics of drug-induced acne in IBD treatments, provides a practical guide for gastroenterologists to manage mild-to-moderate occurrences, and highlights when to seek specialist dermatology advice.”
My take: This is a helpful review of acne management in the setting of IBD.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.