Food recipes -type ingredients you have at home, and ask it for a recipe
Explain complicated topics at age-appropriate levels
Travel itinerary (can specify if active vacation, with kids, specific goals)
Recommendation letters
Resumes
Lesson plans
Solve complex math problems in step-by-step fashion
Provide scientific/journal references
Write music in almost any genre
Write essays and develop ideas for novels
Provide personal advice
Create content in multiple languages
Medication appeal letters
Write or fix computer coding/software
Develop questions for speaker question and answers
Prep for interview
My take: Only George Santos can claim more accomplishments than ChatGPT (AI). It is important to verify the information that ChatGPT provides –it is sometimes wrong.
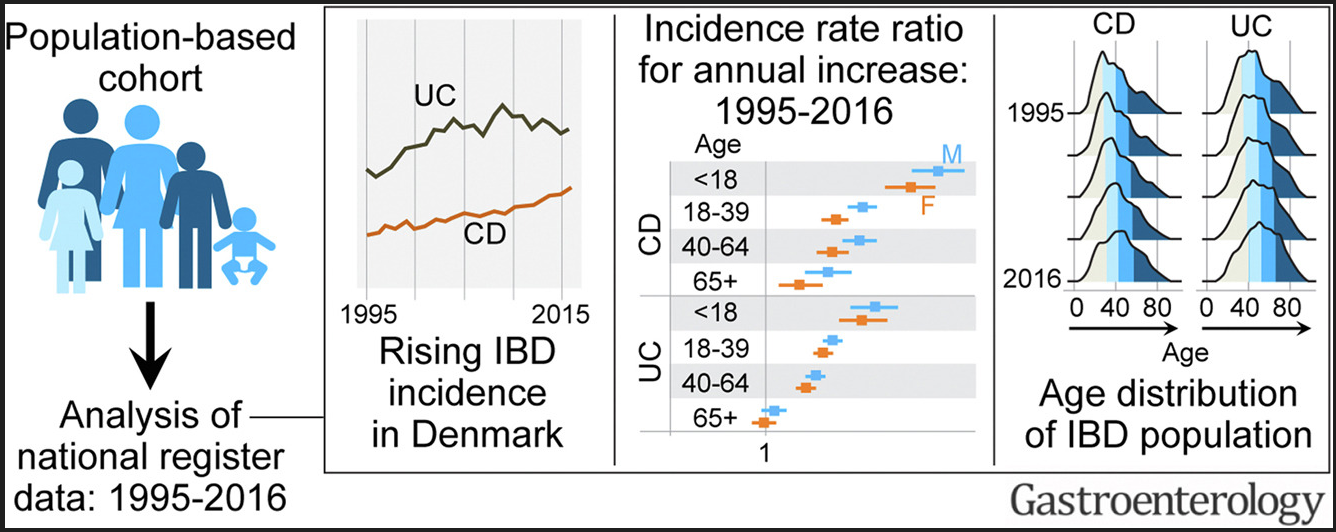
Between 1995 and 2016, the incidence rate (95% confidence interval) per 100,000 person-years rose from 9.1 (8.3–10.0) to 17.8 (16.8–19.0) for CD, and from 21.0 (19.8–22.3) to 28.4 (27.0–29.8) for UC.
The highest increase in CD and UC incidence rates occurred in children and young adults, respectively.
The prevalence of IBD doubled from 1995 to 2016; the greatest increase (2.5-fold) was in UC prevalence among individuals aged >40 years. During this period, the median age of the IBD population increased by 6 to 7 years.
In this retrospective study (n=130), therapeutic drug levels in the postoperative period were associated with improved outcomes for anti-TNF agents (infliximab (IFX) or adalimumab (ADA) but NOT for ustekinumab (UST):
In patients with IFX ≥3 µg/mL, higher rates of deep remission (39% vs 0%; P = .02) existed compared with those with IFX less than 3 µg/mL. This was true for clinical remission (44% vs 9%; P = .04) and objective (83% vs 62%; P = .1) remission.
In patients with ADA ≥7.5 µg/mL, rates of deep (42% vs 0%; P = .02), clinical (42% vs 0%; P = .02), and objective (88% vs 40%; P = .007) remission were higher than patients with lower concentrations.
For UST, rates of deep (28% vs 17%; P = 1.0), clinical (33% vs 33%; P = 1.0), and objective (70% vs 67%; P = 1.0) remission were similar between patients regardless of drug concentration.
In this retrospective study (n=147), a fecal calprotectin >800 mcg/g independently predicted the need for inpatient medical rescue therapy (odds ratio, 2.61; 95% CI, 1.12-6.12). An admission calprotectin >800 mcg/g independently predicted surgery within 3 months (odds ratio, 2.88; 95% CI, 1.01-8.17). My take: This is the least surprising study I’ve read this past month —those with more severe colitis, based on calprotectin values, were more likely to need more intensive treatments.
In this retrospective pediatric study (n=171), the authors found that a generic oral supplement (Fortsip) was as effective as a specialized formula (Modulen IBD) for enteral nutrition. “No difference was demonstrated in remission rate (Fortisip n = 67 of 106 [63%] vs Modulen IBD n = 41 of 64 [64%], P = .89), nonadherence rate (Fortisip n = 7 of 106 [7%] vs Modulen IBD 3 of 64 [5%], P = .57) or method of administration.” The main difference in outcome was a lower expense in the group receiving the generic formula. My take: This study is in agreement with previous studies.
Amjevita (adalimumab-atto) will be available in prefilled autoinjector pens (40 mg) and prefilled syringes (20 mg, 40 mg). Amjevita products will come in low-concentration forms, but they will be citrate-free. It’s expected to launch on January 31, 2023.
2. Cyltezo
Cyltezo (adalimumab-adbm) became the first biosimilar to be designated as interchangeable with Humira. Interchangeable biosimilars go through additional studies to determine whether you can switch back and forth between the biosimilar and the original product without issues. Biosimilars without this designation haven’t gone through these same studies.
Cyltezo will only be available in a prefilled syringe and will come in two doses: 20 mg and 40 mg. Both are low-concentration forms and citrate-free. Cyltezo is expected to launch in the U.S. as early as July 1, 2023.
3. Hyrimoz
Hyrimoz (adalimumab-adaz): a 40 mg dose will be available in both a pen and a syringe. A 10 mg syringe will also be available. Both are low-concentration forms. These products contain citric acid, which is closely related to citrate. Citric acid can also make injections more painful. A citrate-free high-concentration form of Hyrimoz is currently under FDA review. Hyrimoz is expected to launch in the U.S. on September 30, 2023.
4. Hadlima
Hadlima (adalimumab-bwwd) will be available in both an autoinjector and a syringe in a 40 mg dose. And it will come in both low- and high-concentration forms. The high-concentration form will be citrate-free. Hadlima is expected to launch in the U.S. on or after July 1, 2023.
5. Abrilada
Abrilada (adalimumab-afzb) will be available in a prefilled pen (40 mg) and in a syringe (10 mg, 20 mg, 40 mg). All Abrilada products will be low-concentration forms and citrate-free. Abrilada’s manufacturer has applied for interchangeable status with Humira. Abrilada is expected to launch in the U.S. as early as July 1, 2023.
6. Hulio
Hulio (adalimumab-fkjp) will be available in a prefilled pen (40 mg) and in a syringe (20 mg and 40 mg). All forms are low-concentration and citrate-free. Hulio is expected to launch in the U.S. on or after July 1, 2023.
7. Yusimry
Yusimry (adalimumab-aqvh) will only be available in a 40 mg prefilled syringe. It will be in a low-concentration form and citrate-free. Yusimry is expected to launch in the U.S. on or after July 1, 2023.
8. Idacio
Idacio (adalimumab-aacf) will be available in a 40 mg dose in both a pen and a syringe. Both forms will be low-concentration and citrate-free. Idacio is expected to launch in the U.S. as early as July 1, 2023.
My take: In high school, one of math teachers used to call me Hochman sub-1 and my twin brother Hochman sub-2. Perhaps, we can start designating biosimilars in a similar fashion?
“Gaming” U.S. Patent System by Big PharmaHumira, a rheumatoid arthritis drug from the Chicago-based biotech firm AbbVie, generated $17.3 billion in annual sales in 2021. There are 311 patent applications for the drug, 94% of which were sought after FDA approval. AbbVie’s original patent on the drug expired in 2016, but it won’t face competition until 2023
Two other important studies I wanted to cite -both studies have Benjamin Gold, one of my better-known partners, as one of the authors:
KA Chien, C Thomas, V Cooley, T Weinstein, KF Murray, L Muir, C Hayes, BD Gold, LM Gerber, CG Sauer, G Tomer. JPGN 2023; 76: 25-32. Physician Burnout in Pediatric Gastroenterology In this survey with 408 responses (23% response rate), the authors found 29% reported high risk for emotional exhaustion, 18% reported high risk for depersonalization, and 33% reported overall burnout.
VC Cohran, BD Gold, DJ Spencer, CR Cole. JPGN 2022; 75: 689-691. Health Care Disparities in Gastroenterology: The Pediatric Gastroenterology Perspective This commentary reviewed survey results highlighting healthcare disparities which have been identified in IBD, NALFD, and liver transplantation. The authors outline some of the steps that NASPGHAN has taken as well as some of the work that is needed.
In total, 6723 patients completed new patient gastroenterology visits for a primary diagnosis of constipation between 2013 and 2019. Of these, 993 (14.8%) patients had abdominal radiographs taken within 24 hours of their initial visit. Over the 7 years of this project, a mean frequency of abdominal radiograph use decreased from 24% to less than 11%.
No increases in subsequent emergency department visits or hospitalization for constipation within 30 days of patients’ initial visits were seen.
One of the keys to improvement was providing data to individual providers
The authors note that routine radiographs are NOT recommended by expert guidelines in patients presenting with functional constipation.
My take: The trend of using radiographs less frequently shows that a QI project can help avoid low value testing though more than 10% is still too high.
In this retrospective study from Israel with nearly 600,000 children, key findings:
The incidence rate of acid-suppressant medication use increased by 2.8-fold from 18.2 per 1000 in 2005 to 51.0 per 1000 in 2020
Primary care providers accounted for 74.8% of prescribing physicians in 2005 vs 96.1% in 2020, whereas the prevalence of prescribing gastroenterologists decreased from 18.8% to 2.8%
Other factors associated with increased use: first born child, male sex, multiple births and greater socioeconomic status; this latter group is more likely driven by health-seeking tendency rather than financial disparity due to national health insurance
Comments: This high use of acid suppression medications in infancy has been reported in multiple other studies despite the lack of efficacy in prior studies. Pediatricians, more than pediatric gastroenterologists, may be less familiar with the GERD guidelines and potential adverse effects of acid suppression (including association with an increase food allergies).
My take: This Israeli study shows that pediatric gastroenterologists are using acid blockers less in infants while pediatricians are using them more often. It is interesting that after the first child, parents are less likely to seek medical attention & are more tolerant of reflux symptoms.
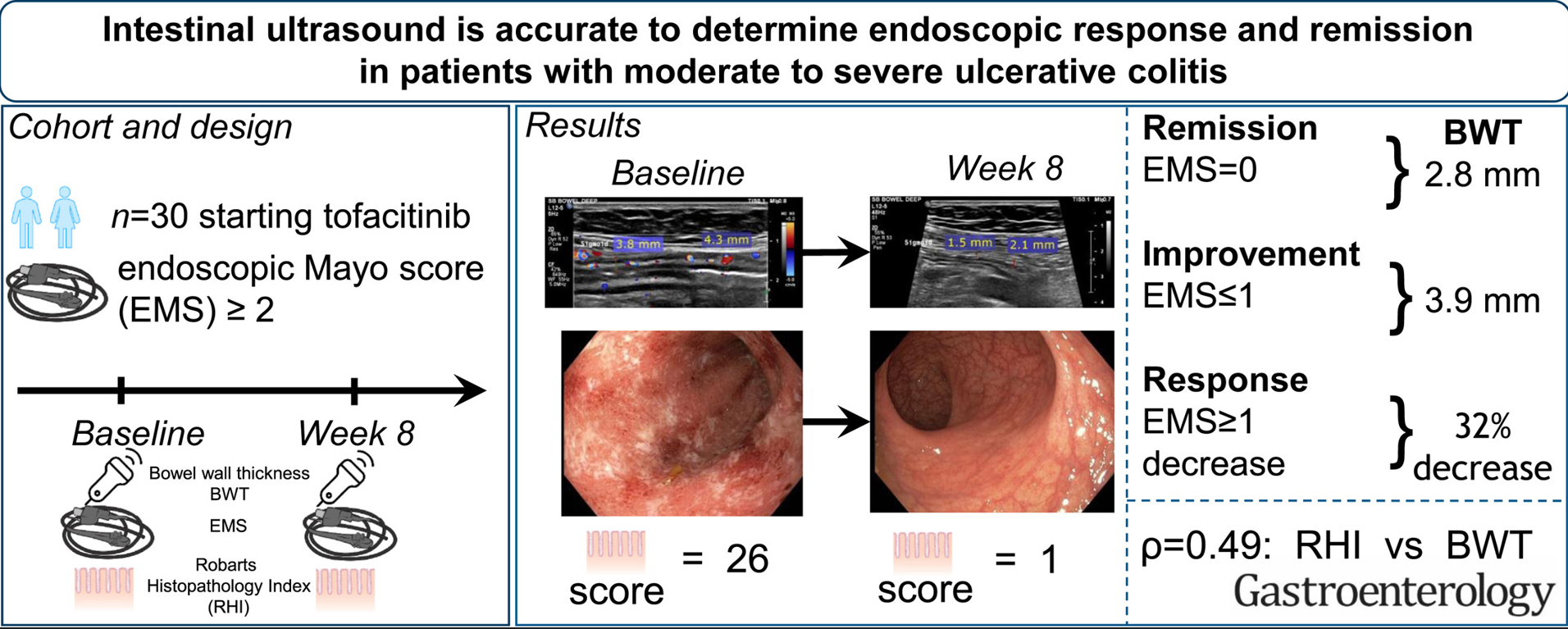
27 patients with moderate to severe ulcerative colitis (UC) completed followup in this single-center, prospective, longitudinal cohort study. Key findings:
Bowel wall thickness (BWT) correlated with endoscopic Mayo score. “The most accurate cutoff for BWT was 2.8 mm for endoscopic remission, 3.9 mm for improvement, and a decrease of 32% for response.”
The associated editorial (C Palmela, C Maaster.Gastroenterol 2022; 163: 1485-1487. Open Access! The Use of Intestinal Ultrasound in Ulcerative Colitis-More Than a Mucosal Disease?) details other studies showing the utility of intestinal ultrasound, including the TRUST%UC study which enrolled 253 patients with UC. “. At baseline, 88.5% of patients had increased bowel wall thickness (BWT). Response to therapy could be detected as early as 2 weeks after initiation of therapy, as shown by reduction of abnormal BWT.” In anothre study with severe UC, “BWT reduction of >20% being an excellent predictor of response to intravenous steroids at 48 hours, as shown recently by Ivemark et al.10“
The editorial notes that intestinal ultrasound “is often thought as being operator dependent. Nonetheless, several studies have shown an excellent inter-observer agreement in IUS, especially for the assessment of BWT,7,12 as was also found in this [De Voogd] study.” An additional finding in the De Voogd study was that the “the submucosa was the most thickened layer, and after 8 weeks of therapy it was also the most responsive layer;” thus, UC is not simply a mucosal disease.
My take: This study shows that with more widespread adoption, many UC patients could be followed non-invasively with intestinal ultrasound (and calprotectin).
Methods: VEDOKIDS was a paediatric, multicentre, prospective cohort study done in 17 centres in six countries. We report the 14-week outcomes as the first analyses of the planned 3-year follow-up of the VEDOKIDS cohort
Key findings:
32 (42%) of 77 children with ulcerative colitis and 21 (32%) of 65 children with Crohn’s disease were in steroid-free and exclusive enteral nutrition-free remission at 14 weeks.
In children who weighed less than 30 kg, the optimal drug concentration associated with steroid-free and exclusive enteral nutrition-free clinical remission was 7 μg/mL at week 14, corresponding to a dose of 200 mg/m2 body surface area or 10 mg/kg
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
The following information was provided by our coding advisor, Mary Suhr.
Key points:
Time codes (when used) for inpatient visits have changed (see below). In 2023, when you share a service with an APP, you may bill on patient medical decision making or time spent. You can add the time together and whoever spends more total time on that date of service (including face to face and non-face to-face) gets to be the service provider for that charge.
Extra time code: 99418 for every 15 minutes increments above average inpatient code.
Observation codes are obsolete.
Specific requirements for documentation of History and Physical exam are NOT needed for coding. Good documentation is still important part of medical practice and for liability; patient still needs to be examined.
ALL outpatient and inpatient E/M visits will be leveled using the same methodology.
Coding is based on medical decision making or time code (whichever has higher complexity). When selecting a level of service for Medical Decision Making, there is still the concept of having three components/tables and the requirement that two of the three components are met. Tables 1, 2, and 3 outline the requirements.
CPT 99251 (Straightforward Inpatient Consult) and CPT 99241 (Straightforward Outpatient Consult) are going away because the history and exam requirements for consults no longer apply and history/exam was the only difference between level 1 and level 2 consultation codes.
For consultations, you still need a requesting provider, a reason for the consult and a report back to the provider. CMS was explicit this year that assuming care of the problem is not considered a consult.
Consultationscannot be shared between two providers (e.g. physicians and APPs). If a consultation is shared between an APP and a MD, our advisor recommends the use admission codes for those. This is true for inpatient consultations as well as office-based consultations.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“Rebyota is approved for the prevention of recurrence of Clostridioides difficile infection (CDI) in individuals 18 years of age and older. It is for use after an individual has completed antibiotic treatment for recurrent CDI.”
“Rebyota is administered rectally as a single dose [150 mL]. Rebyota is prepared from stool donated by qualified individuals….The effectiveness of Rebyota was evaluated in an analysis of data from a randomized, double-blind, placebo-controlled, multicenter study….the overall estimated rate of success in preventing recurrent CDI through 8 weeks was significantly higher in the Rebyota group (70.6%) than in the placebo group (57.5%).”
My take: As pharmaceutical companies gain approval for fecal transplant products, I would anticipate a significant increase in costs. This product seemed to have a fairly low success rate compared to placebo.
In this retrospective study of 41 adults with history of ileal pouch-anal anastomosis (IPAA) for ulcerative colitis (UC), the authors evaluated the clinical response (subjective judgement of provider) to chronic vancomycin therapy (125 mg twice a day).
Key findings:
At 4 weeks, 21 (51%) of patients had a clinical response. 16 of these patients maintained a clinical response at 3 and 6 months (remained on treatment).
6 additional patients demonstrated a later response. In total 22 (54%) were considered clinical responders at 3 and 6 months.
The mean number of antibiotics utilized prior to vancomycin was 4, including ciprofloxacin, metronidazole, levofloxacin, rifaximin, sulamethoxazole-trimetoprim, amoxicillin, and amoxicillin-clavulanic acid
My take: Since vancomycin has poor enteral absorption, it’s side effect profile is very favorable. More prospective and objective data is needed; however, vancomycin’s high cost will likely limit frequent use.