This was an open-label, retrospective study with 64 patients with collagenous gastritis (CG) (50 adults, 14 children). Budesonide was administered in 2 formulations: open-capsule budesonide or compounded immediate-release budesonide capsule. Key finding: Of the patients treated with topically targeted budesonide (TTB), 89% had a clinical response (42% complete, 46% partial), and 88% had a histologic response (53% complete, 33% partial).
In medical school, I took additional courses in bioethics and one of the influential lecturers was Tristramm Engelhardt (Right to Health Care). “According to him, injuries, disabilities, and diseases arising from natural causes are considered unfortunate. On the other hand, those situations become unfair when brought about by the doing of others. Engelhardt also notes that the result of someone’s unfair action should not be attributed to the society as a whole.”
Two recent articles detail the link between socioeconomics and outcomes in liver transplantation. Are these problems unfair or just unfortunate?
Disparities remain in pediatric liver transplantation at all time points: from access to referral for transplantation, likelihood of living donor transplantation, use of exception narratives, waitlist mortality, and inequitable posttransplant outcomes
Black children are less likely to be petitioned for exception scores, have higher waitlist mortality, are less likely to be the recipient of a living donor transplant, and have worse posttransplant outcomes compared with White children.
Children living in the most socioeconomically deprived neighborhoods have worse posttransplant outcomes.
Children living farther from a transplant center have higher waitlist mortality
Based on retrospective analysis of 3454 patients (2011-2018), neighborhood poverty was independently associated with waitlisting (odds ratio 0.56, 95% confidence interval [CI] 0.38–0.82) and death during LT evaluation (hazard ratio 1.49, 95% CI 1.09–2.09)
Despite use of the objective prioritization with MELD scores in the allocation of organs, disparities in access for LT continues for vulnerable populations
My take: It is unfortunate but not surprising that poverty and socioeconomic factors adversely affect liver transplantation; the outcomes show stark differences. These issues, however, affect every aspect of health care (& beyond). Though they are not easily addressed, efforts to try to level the playing field are important especially with regard to transplantation to assure optimal use of this life-saving resource.
The authors have devised a SQUIRT score for short bowel syndrome. The higher score indicates better enteral tolerance with a highest score of 13 and a lowest score is 3. It is a composite score based on composition, frequency and volume/blowouts. The authors define a blow-out to be a stool loose enough and large enough for the child to require a change of clothes.
How to Score:
Consistency (choose best stool of the day) Playdough, Formed 5 Peanut Butter, Pasty 4 Pudding, Seedy 3 Pea Soup, Loose 2 Water 1
Occurrences (over 24 hours) 1 to 3 4 4 to 6 3 7 to 9 2 Greater Than 10 1 Ostomy Present 0
Volume With Ostomy Without Ostomy (mL/kg) (# of blowouts)
< 10 mL/kg 8 0 =4
10 -14 mL/kg 7 15-19 mL/kg 6 1 =3
20-24 mL/kg 5 2 =2 25-29 mL/kg 4
30-34 mL/kg 3
35 mL/kg 2
>35 mL/kg 1 >3 =1
The authors state that this scoring system has been used in their institution. “This tool can provide objective information to guide clinical decision making. Even patients with ostomies, for whom we can measure stool volume, benefit from SQUIRT scores because including the variable of stool consistency provides a more nuanced assessment than relying on volume.”
My take:This type of scoring system would be useful, primarily in patients in which the volume of stool is difficult to measure. It would benefit from trials to validate its utility.
During the pandemic, several of the pharmaceutical companies have helped improve the reputation of the industry by expeditiously developing life-saving therapies and vaccines. At the same time, many have continued with outrageous price increases of generic medications. An example of this is rectal indomethacin which is used for the prevention of pancreatitis after ERCP. In this commentary, the key points:
The current price in the U.S. for this previously inexpensive medication is now $429 (in 2021) (previously $17). For patients, this charge is often multiplied by hospital billing departments and is frequently NOT covered by insurance as the manufacturer has not filed a new drug application with the FDA (new indication).
The authors note that rectal diclofenac would be a suitable alternative with similar (?better) effectiveness but is currently not available in U.S.
The government could allow importation of either diclofenac or indomethacin (see Table below for costs of these medications in other countries). “If the government used the powers granted in the Medicare Modernization Act of 2003, the price gouging problem caused by rectal NSAIDs could be swiftly solved without the need for expanding the US manufacturing market.” This would drop the “price of this potentially lifesaving prophylaxis by 99.24%.”
My take: I am still grateful to Mark Cuban (Why I No Longer Need to Be A Billionaire | gutsandgrowth) who is much more likely to fix the generic drug pricing problem than our government which has been reluctant to take measures against big pharma.
One of the difficult aspects at this point in my career is saying goodbye as physicians retire. Larry Saripkin, who is an amazing person, is retiring (last day yesterday).
I first met Larry when I was working at Egleston Hospital. Larry, along with Jeff Lewis, provided coverage for me when I had become the single physician in my group. This allowed me to be off when our youngest son was born. Then, later, Larry helped convince me to join the merging GI groups at Scottish Rite (23 years ago). This has been one of my best decisions. Of course, I feel that our group delivers very good care for our patients. Yet, the main reason why it has been a good choice is working alongside some terrific individuals.
Larry has a keen intellect and a wonderful ability to connect with everyone, even families with very stressful medical conditions. He is very generous with his time. I remember one night when he was on-call, the parents of one of my patients called. They were upset because they could not get the feeding pump to work. They told me that Larry insisted on driving out to their house (around 11 pm). He and his wife showed the family how to work the pump.
For about 15 years, he has spent a week every summer at Camp Oasis as the medical director. At heart, Larry is still a kid. For years, he would take some of the younger staff (or kids of other physicians) with him when he went to Bonaroo.
He has served as a mentor to many of us in our group and to about a dozen scribes who have moved on to become physician assistants or to medical school/physicians.
Countless families have told me how important Larry has been to them. He has attended many of his patients’ celebrations (eg. weddings).
It will be bittersweet going forward when I walk by Larry’s office & missing out on some great story or some new music.
In this picture with Melissa and Cassie (from 2011), Larry is dressed up as a cheeseburger (with a fake mustache) at Camp Oasis.
This retrospective study of patients (n=74) diagnosed with autoimmune hepatitis (AH) prior to 16 years of age examined the safety of low dose steroids. Median age of patients with 12.8 yrs and median followup was 12.6 years. Typically, after induction, patients were tapered over ~2 months to 5 mg per day (& 2.5 mg per day if <12 years). Key findings:
Growth of patients with AILD on a daily maintenance dose of steroids remains stable and within normal range during long-term follow up. At all time-points, the mean z-scores for weight, height and BMI were within the normal range, indicating normal nutritional status.
Small, daily doses are effective in maintaining disease control and minimize the need for high-dose steroid pulses during relapses.
In this cohort, there were 14 patients in which prednisolone was utilized as monotherapy; the majority received cotherapy with azathioprine (n=44), mycophenolate (n=12); triple-therapy was utilized tacrolimus (n=4).
Prednisolone was stopped in 17 patients (23%) after a median time of 9.5 years (range 3 years-14 years)
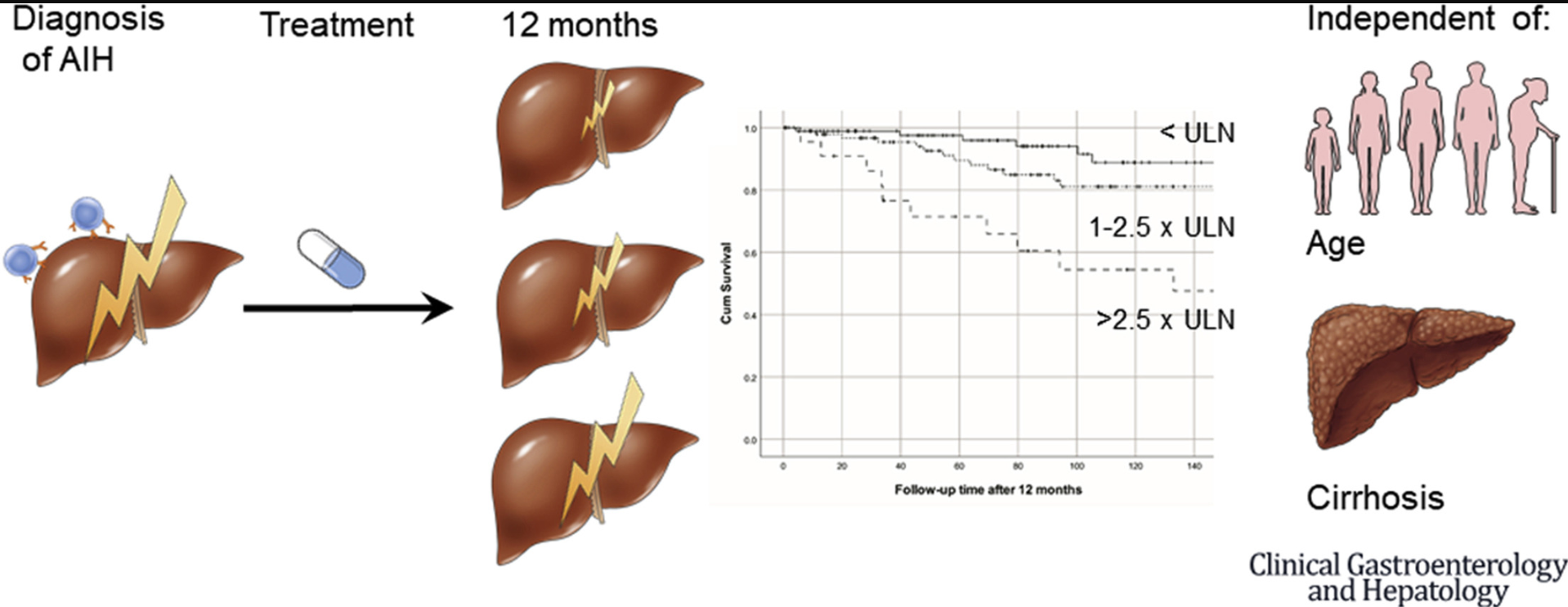
In this multicenter cohort study (n=301), it was shown that higher aminotransferases during treatment were independent of baseline risk factors associated with liver transplantation–free survival in patients with AIH type 1. Median followup was 99 months. Key finding:
During follow-up, 15 patients required liver transplantation and 33 patients died
In multivariate analysis AST at 12 months (HR, 2.13; P < .001) was predictive for survival independent of age, AST at diagnosis and cirrhosis, while IgG was not associated with survival (HR, 1.30; P = .53)
There was a trend toward a worse survival in patients with mildly elevated aminotransferases (1–1.5× upper limit of normal) compared with patients with normal aminotransferases (P = .097)
My take: Normalization of AST (aminotransferases), especially during the first year of treatment, is associated with better long-term outcomes. The study by Manwani et al suggest that long-term low dose steroids are associated with low risks.
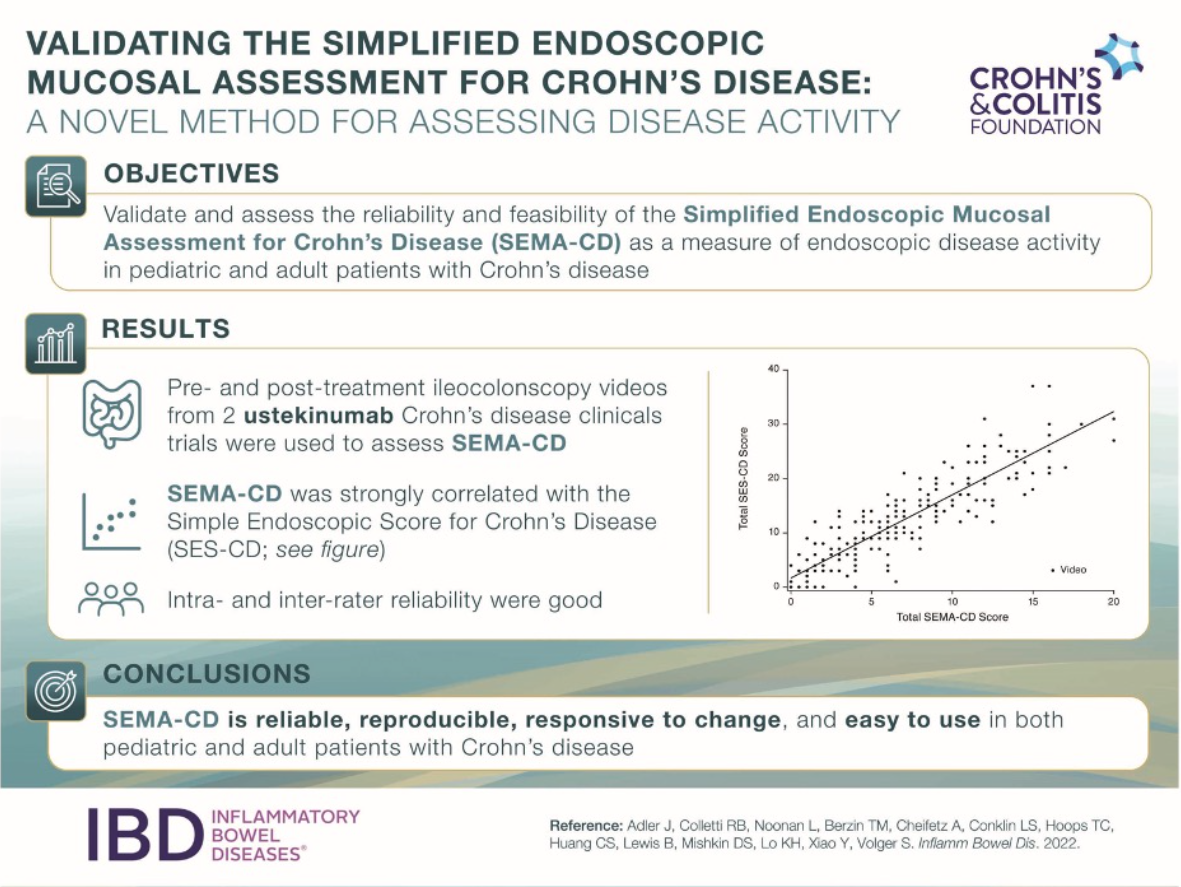
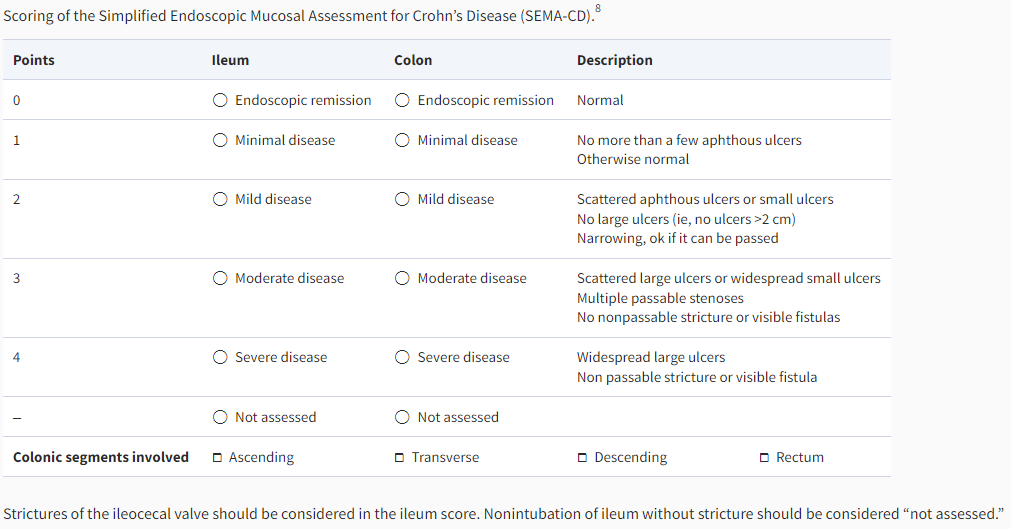
“The SEMA-CD is scored by assigning a numerical value ranging from 0 (endoscopic remission) to 4 (severe disease) for each bowel region (ileum and colon). The overall colon is scored as a whole based on the most severe colonic segment. The number of colonic segments with any degree of active disease is recorded, regardless of the severity of individual segments. The overall colon score is then multiplied by the number of involved colonic segments, and the result is added to the ileum score.”
In this retrospective study, “during a 20-month period until December 2021 using PPE and three different test approaches: no testing (n=4543), rapid antigen (RA) testing (n=682) and RT-PCR testing (n=10 465). In addition, 60 endoscopies were performed in patients with proven COVID-19. Not a single staff member became infected with SARS-CoV-2 during the 20 months analysed; vaccination rate of the team was 97%.”
The authors note that routine testing of clinical team was not performed; thus, they cannot exclude the possibility of asymptomatic infections.
My take (borrowed in part from authors): “PPE is highly effective for avoidance of SARS-CoV-2 transmission during upper or lower GI endoscopies.” Pre-op testing for COVID has many downsides: increased costs, delays in care, potential exacerbation of health disparities, and detrimental effects to endoscopy efficiency (especially with inconclusive results)
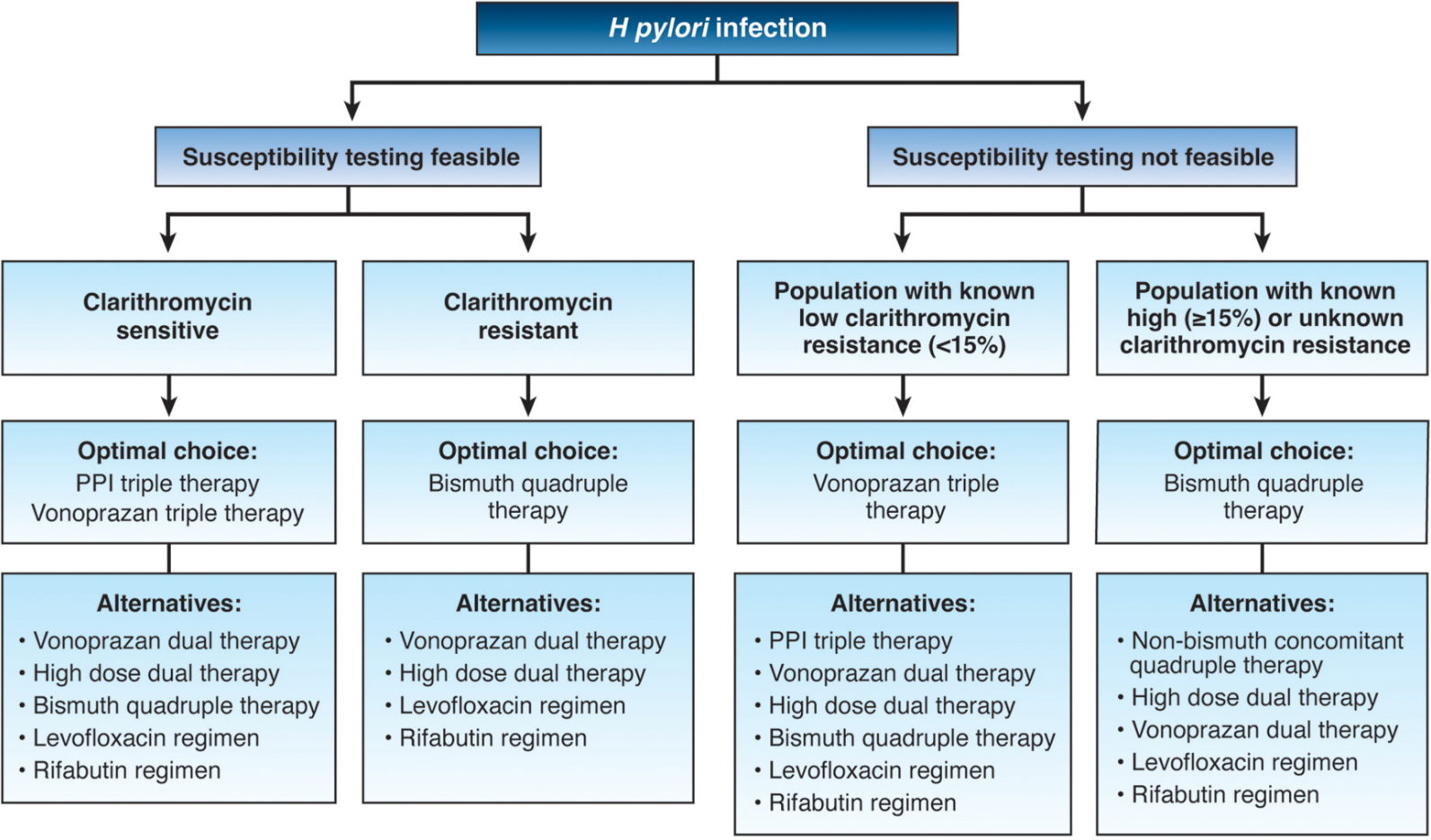
“The (FDA) has approved 2 vonoprazan-based medications for the treatment of Helicobacter pylori (H. pylori) infection.
Phathom Pharmaceuticals announced the approvals of both the Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin) based on positive safety and efficacy data from the phase 3 PHALCON-HP trial.”
Key findings from this randomized, controlled trial with treatment-naive 1046 adults:
In all patients, vonoprazan triple and dual therapy were superior to lansoprazole triple therapy (80.8% and 77.2%, respectively, vs 68.5% (both superior)
In patients with clarithromycin resistance, vonoprazan triple therapy was effective in 65.8%, dual therapy in 69.6%, vs lansoprazole triple therapy 31.9% (both superior)
Vonoprazan increases intragastric pH rapidly “and maintains it to a greater degree than PPI; this has been associated with higher H pylori eradication rates” (in prior studies as well)
Based on this new information, the author proposes the treatment algorithm below and notes that “the role of increased acid suppression by PPI substitution with vonoprazan should be examined in other H pylori regimens.” The author favors bismuth quadruple therapy in those with clarithromycin resistance as non-bismuth quadruple therapy utilizes an unnecessary antibiotic (clarithromycin).
Other points:
Metronidazole resistance is fairly common, but bismuth quadruple therapy can overcome much of the metronidazole resistance
Levofloxacin resistance is quite high in certain regions and should only be used with caution, given recent warnings from the US Food and Drug Administration of aortic rupture in susceptible individuals
Rifabutin can cause some bone marrow suppression
My take: With the more widespread availability of susceptiblity testing (beyond clarithromycin), I anticipate more targeted treatments. At the same time, vonoprazan-based treatments are likely to be important in increasing eradication rates.
Related blog posts:
How To Achieve Helicobacter Pylori Cure Rates of >95% This post lists some of the codes from several commercial companies that perform susceptibility testing. The Quest code has been updated. Our Quest representative indicated code: 36994 (H. pylori culture with reflex to susceptibility). Preferred Specimen: 3 mm Gastric/Antral or Duodenal biopsy collected in Brucella broth or Trypticase Soy Broth (TSB) with 10-20% glycerol
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In 2018, Belcher pharmaceuticals managed to get the FDA to designate Ethanol as an orphan drug with a subsequent increase in cost to ~$10,000 for a 10-vial pack (10-day supply) (Related post: FDA ‘Safety Initiative’ Now Means an Ounce of Ethanol Costs $30,000). As such, many (?most) children with intestinal failure (IF) no longer have access to this therapy which prevents life-threatening infections to their central lines.
A recent retrospective study (R Josyabhata et al. JPGN 2022; 75: 304-307. Sodium Bicarbonate Locks May Be a Safe and Effective Alternative in Pediatric Intestinal Failure: A Pilot Study) examined the use of sodium bicarbonate lock therapy (SBLT) as an alternative to ethanol in four children. This study was prompted by a clinical trial in hemodialysis patients which demonstrated a reduction in catheter-related bloodstream infections (CRBSI). None of the four patients had a CRBSI.
My take: A much larger multi-center study will be needed to determine if SBLT is worthwhile.
K Culbreath et al. JPGN 2022; 75: 345-350. Antibiotic Therapy for Culture-Proven Bacterial Overgrowth in Children With Intestinal Failure Results in Improved Symptoms and Growth This article describes outcomes of 104 children with intestinal failure who underwent endoscopy and had duodenal cultures sent to identify bacterial overgrowth/susceptibility/targeted antibiotics. This information was associated with fewer symptoms and better growth. The methods section provides detailed information on collection and handling of specimens (which could be helpful for those trying to implement this strategy). However, there is not a standardized protocol for duodenal cultures to detect bacterial overgrowth.