Since May 2021, “those living in counties that voted 60% or higher for Trump in November 2020 had 2.26 times the death rate of those that went by the same margin for Biden. Counties with a higher share of Trump votes had even higher mortality rates…. previous polling has shown that belief in misinformation is highly correlated with being unvaccinated. Kaiser examined several common pieces of misinformation such as the idea that the government is exaggerating the severity of the pandemic, or that the vaccines contain a microchip. Kaiser’s poll found that 94% of Republicans believed one or more false statements about the vaccines.”
I have not paid close attention to the movement to unionize health care workers in the U.S. As such, I learned a few things in this past weekend NY Times article: Doctors and Nurses Shouldn’t Have to Strike (online version titled “When Health Care Workers Are Protected, Patients Are, Too”)
Excerpts:
Since the pandemic began, the health care work force — the country’s largest industry by employment — has shrunk by nearly 2 percent… Now, with astronomical turnover and rising demand as patients seek care that they may have put off during the height of the pandemic, hospitals, clinics, nursing homes and home care agencies across the country lack sufficient staff members to adequately care for patients…
Most hospitals might be private companies in their formal legal identity, but the reality is that government has shaped the health care system every step of the way of its modern existence…
Unionized health care workers all over the country are fighting back against untenable conditions in the health care industry, and they are often met with harsh treatment by employers for doing so…
Peace agreements are popular with unions because they help prevent the type of devastating reprisals that drive many workers out of their jobs, but employers often refuse to accept them…
By giving weight to workers’ on-the-job needs, while eliminating strikes, labor peace policies in health care facilities benefit patients because they give workers more power to manage their work environments. They also make establishing unions easier for workers, and data suggests that unionization in health care improves patient care.
My take: In our hospital system, recent staffing shortages have forced the hospital to close a significant number of intensive care unit beds. This will inevitably lead to postponement or cancellation (often at last minute) of needed surgical procedures (that often require availability of an ICU bed). The fix for some of the ills in our hospital system is going to be difficult. Adequate staffing with highly-trained health care workers needs to be the top priority.
Another sign that helps keep folks on the designated walking areas –this one was at the Valley of Fires State Park, NM
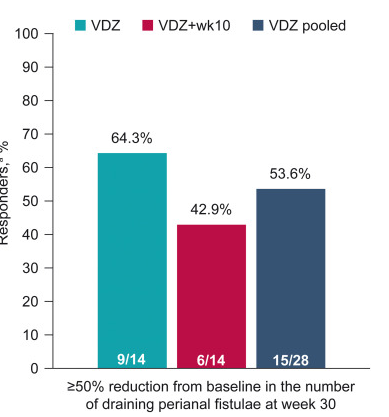
Methods: “Patients with moderately to severely active CD and 1–3 active perianal fistulae (identified on magnetic resonance imaging [MRI]) received vedolizumab 300 mg intravenously at weeks 0, 2, 6, 14, and 22 (VDZ) or the same regimen plus an additional vedolizumab dose at week 10 (VDZ + wk10)… Enrollment was stopped prematurely because of recruitment challenges”
Key findings:
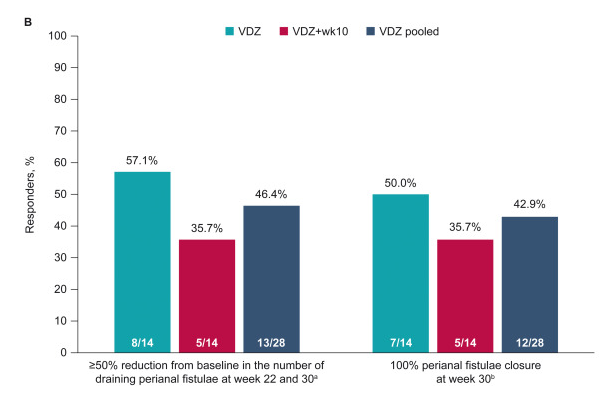
“Rapid and sustained fistula closure was observed; 53.6% (VDZ, 64.3%; VDZ + wk10, 42.9%) and 42.9% (VDZ, 50.0%; VDZ + wk10, 35.7%) of patients achieved ≥50% decrease in draining fistulae and 100% fistulae closure, respectively, at week 30”
“MRI healing, defined as the disappearance of T2 hyperintensity signal and absence of gadolinium contrast enhancement,3 was not reached in this study…gadolinium contrast enhancement showed improvement at week 30…MRI studies have shown that internal fistulae healing lags behind clinical remission by a median of 12 months”
Figure 1Figure 2 B
The study findings are limited by relatively small size and lack of control group (eg. placebo or seton/antibiotic group). However, the rate of response in this study is significantly higher than placebo studies which have shown “~1 in 6” who experienced fistula closure.
My take: Vedolizumab is another option for treating Crohn’s disease with perianal fistula. Both regimens in this study were associated with response, though the additional 10-week dose (in one group) did not improve outcomes.
Most patients that I see with celiac disease (CD) do very well after diagnosis/implementation of dietary therapy. A recent study indicates a subset of patients have significant work disability as adults.
In this large-scale nationwide study (part of the ESPRESSO study) from Sweden, the authors used prospectively recorded register data to estimate work loss in patients with CD in comparison to the general population, including the temporal relationship of work loss before and after diagnosis. This study included more than 16,000 patients with CD.
Key findings:
In 2015, patients with prevalent CD had a mean of 42.5 lost work days as compared with 28.6 in comparators
More than one-half of the work loss (60.1%) in patients with CD was derived from a small subgroup (7%), whereas 75.4% had no work loss
The annual mean difference between patients and comparators was 8.0 days of lost work 5 years before CD diagnosis, which grew to 13.7 days 5 years after diagnosis in the incident CD group (dx between 2008-2015)
In the discussion, the authors speculate about whether the work loss could be due to inadequate response to a gluten free diet; however, in this study, the authors found similar work loss between patients with CD with or without mucosal healing (only 25% underwent f/u biopsy).
My take: It would be interesting to see the pediatric corollary of work loss, namely school absenteeism and whether this is increased in a small subset as well. My suspicion is that the subset with increased work loss likely has a higher rate of functional disorders, in addition to CD, than the comparator group and probably accounts for a significant amount of the work disability.
A couple recent articles indicate a lot of reasons for concern.
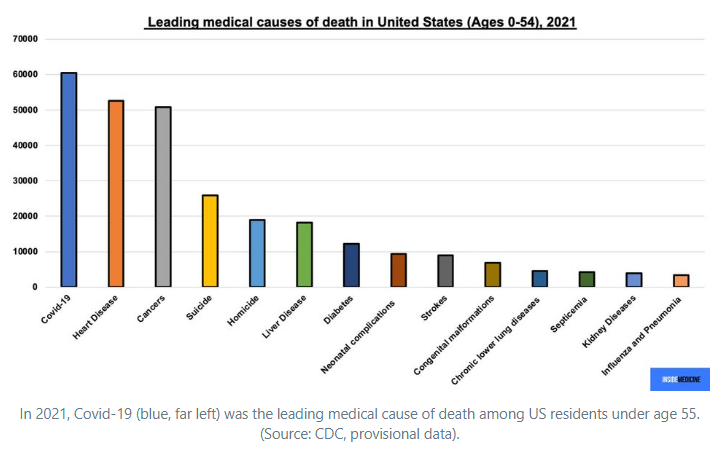
First of all, it is important to recognize that even among persons less than 55 years of age, COVID-19 was the leading cause of death in 2021. Inside Medicine: Open Access: The million US Covid dead are younger than you think.
There has been a culture shift to learn to live with the virus. This is evident almost everywhere from packed restaurants, crowded venues, etc. However, there is currently high transmission and variants that are evading vaccine protection as detailed by Eric Topol, Open Access: The Covid Capitulation
Key points:
The United States is now in the midst of a new wave related to Omicron variants BA.2 and BA.2.12.1 with over 90,000 confirmed new cases a day and a 20% increase in hospitalizations in the past 2 weeks…The real number of cases is likely at least 500,000 per day, far greater than any of the US prior waves except Omicron.
“Infections…beget more cases, …Long Covid, … sickness, hospitalizations and deaths. They are also the underpinning of new variants.”
CDC currently is vastly underestimating the number of cases leading many towards false confidence, “feeding the myth that the pandemic is over.”
“As of last week, 43% of new cases were attributable to BA.2.12.1 …. BA.2.12.1 is out-competing BA.2 with its 25% higher transmission rate, which foretells its further rise to dominance across the US in the days and weeks ahead.”
“This family of Omicron variants with functional impact indicates more rapid evolution of the virus than what we have seen previously.”
There has been a “reduction in vaccine effectiveness that we are now encountering…[Protection from severe disease] has declined to approximately 80%, particularly taking account the more rapid waning than previously seen.”
“It’s overly optimistic to think we’ll be done when Omicron variants run their course. Not only are they providing further seeding grounds for more variants of concern, but that path is further facilitated by tens of millions of immunocompromised people around the world, multiple and massive animal reservoirs, and increased frequency of recombinants.”
“Vaccinated individuals accounted for … 42 per cent [of the deaths] during the Omicron wave. This is attributable to waning of protection, lack of boosters, and the diminished protection against Omicron (BA.1).”
What needs to be done: More boosters/vaccines (“we rank 60th in the world’s countries for boosters”) along with more medicines, and nasal vaccines which could induce mucosal immunity
My take: Unfortunately, these articles indicate that we have a long way to go. High quality masks are going to be needed at health care settings for a while. For those trying to avoid COVID-19, it will remain important to avoid large indoor gatherings. For public policy/economic policy, we need to continue to fund COVID-19 resources.
Background: Whether proactive therapeutic drug monitoring (pTDM) is superior to reactive TDM (rTDM) is not entirely clear, though some studies have shown better outcomes with pTDM. Additionally, Colombel et al (Clin Gastroenterol Hepatol 2019; 17: 1525-32) showed that antidrug antibodies during combination therapy were detected only in those with the lowest quartile of infliximab trough levels; this suggests that optimized monotherapy should be similarly effective to combination therapy.
Methods: The authors retrospectively analyzed a commercial laboratory database (Prometheus) with 3970 patients and paired 6-thioguanine (6-TGN) levels with infliximab (IFX) and antibodies to infliximab (ATIs)
Key findings:
“Those with higher levels of IFX had negligible benefit from concomitant thiopurine treatment in preventing ATIs.”
ATIs were detected in 9.9% of all patients. IFX level of >5 mcg/mL were associated with a very low risk of ATI (OR 0.05). “Immunogenicity was negligible (<3%) in the presence of IFX concentrations greater than 5 mcg/mL.”
6-TGN levels (>125) were associated with lower risk of ATI, OR 0.42; though, this effect had a significant impact, only for those with with IFX <5 mcg/mL.
The authors note the prospective OPTIMIZE study (NCT04835506) should help determine the effectiveness of pTDM.
My take: In patients with IFX levels >5 mcg/mL, there does not appear to be much benefit for most patients from the addition of a thiopurine; this may not be true for those who are switching to a 2nd anti-TNF agent due to antidrug antibodies. This study supports pTDM to assure adequate IFX levels.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“Between 2004 and 2018, the number of reported illnesses from mosquito, tick, and flea bites more than doubled, with more than 760,000 cases reported in the United States. Nine new germs spread by mosquitoes and ticks were discovered or introduced into the United States during this period. The geographic ranges where ticks spread Lyme disease, anaplasmosis, ehrlichiosis, and spotted fever rickettsiosis have expanded, and experts predict that tickborne diseases will continue to increase.”
The general approach, outlined in Figure 1, is to empirically treat patients with typical GERD symptoms for 4-8 weeks with single-dose PPI. In those with response, the goal is to use the lowest effective dose and consider reflux testing (“offer endoscopy with prolonged wireless reflux monitoring”) if needing prolonged treatment (>1 yr). In those without a response, adjusting treatment (possibly change medication or change to twice a day) should be considered and reflux testing (off treatment) is recommended as well in those lacking response to treatment.
Some of the recommendations/best practice advice:
Clinicians should provide standardized educational material on GERD mechanisms, weight management, lifestyle and dietary behaviors, relaxation strategies, and awareness about the brain-gut axis relationship to patients with reflux symptoms.
Clinicians should emphasize safety of proton pump inhibitors (PPIs) for the treatment of GERD.
Clinicians should provide patients presenting with troublesome heartburn, regurgitation, and/or non-cardiac chest pain without alarm symptoms a 4- to 8-week trial of single-dose PPI therapy. With inadequate response, dosing can be increased to twice a day or switched to a more effective acid suppressive agent once a day. When there is adequate response, PPI should be tapered to the lowest effective dose.
If troublesome heartburn, regurgitation, and/or non-cardiac chest pain do not respond adequately to a PPI trial or when alarm symptoms exist, clinicians should investigate with endoscopy and, in the absence of erosive reflux disease (Los Angeles B or greater) or long-segment (≥3 cm) Barrett’s esophagus, perform prolonged wireless pH monitoring off medication (96-hour preferred if available) to confirm and phenotype GERD or to rule out GERD.
Clinicians should perform upfront objective reflux testing off medication (rather than an empiric PPI trial) in patients with isolated extra-esophageal symptoms and suspicion for reflux etiology.
Clinicians should provide pharmacologic neuromodulation, and/or referral to a behavioral therapist for hypnotherapy, cognitive behavioral therapy, diaphragmatic breathing, and relaxation strategies in patients with functional heartburn or reflux disease associated with esophageal hypervigilance reflux hypersensitivity and/or behavioral disorders.
In patients with proven GERD, laparoscopic fundoplication and magnetic sphincter augmentation are effective surgical options, and transoral incisionless fundoplication is an effective endoscopic option in carefully selected patients.