Healthcare workers with COVID-19 who are asymptomatic can return to work after 7 days with a negative test, and that isolation time can be cut further if there are staffing shortages.
Healthcare workers who have received all recommended COVID-19 vaccine doses, including a booster, do not need to quarantine at home following high-risk exposures.
This retrospective case-control study identified 93 patients out of 1032 with chronic HCV infection who had a relapse of detectable infection following treatment. Key findings:
12 patients (13%) spontaneously cleared HCV within 6 months after the documented relapse without additional therapy
The spontaneous clearers had low levels of HCV RNA (<4 log IU/mL in 11 of 12) and normal levels of alanine aminotransferase at the time of relapse. Low level RNA was identified in only 1 persistent relapser
There was no significant difference between the spontaneous clearance group and the SVR12 group in magnitude and breadth of HCV-specific T cell responses
The authors note that one limitation of the study was a false positive PCR assay –though this does not negate their message that retesting is important before retreatment
The relatively high relapse rate (9%) in this cohort is likely related to the use of first-generation DAA therapy
The timing of retesting in the 12 with spontaneous clearance was variable. 7 who had repeat testing at 3 months were all negative.
My take: In those with a low level virological relapse after DAA therapy for HCV, it is a good idea to repeat testing before consideration of further treatment.
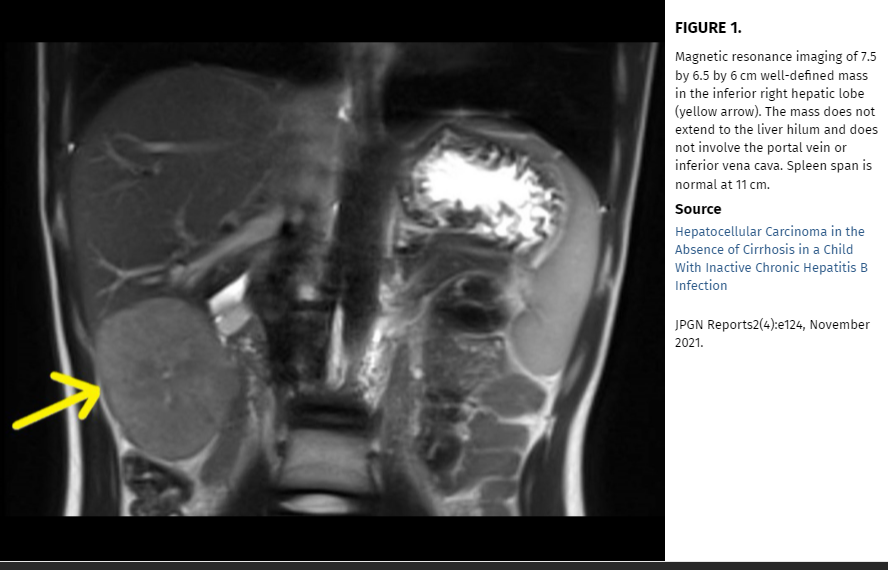
In this case study, the authors “describe an unusual case of a child with chronic hepatitis B infection who developed HCC in the absence of active hepatitis or cirrhosis.” Based on their case report, they advocate for “regular HCC surveillance for all children with chronic hepatitis B, regardless of presence or absence of hepatitis or cirrhosis.”
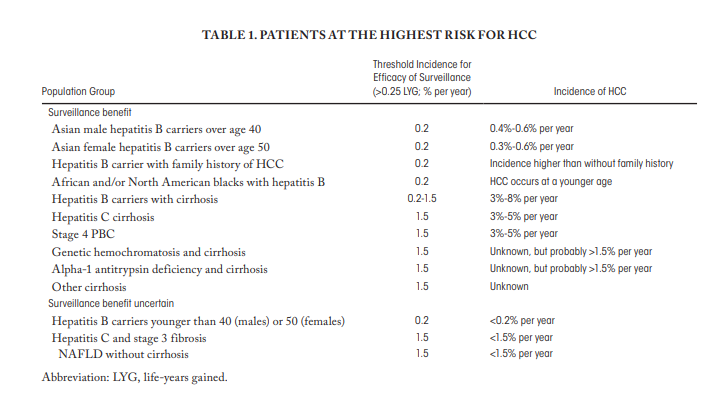
However, the authors suggestions to expand surveillance to all children with hepatitis B is NOT aligned with current expert opinion (by most experts). This potential recommendation deserves (deserved) more commentary in their discussion. The AASLD recommends offering surveillance when the risk of HCC is at least 1.5% per year and the incidence is greater than 0.2% per year, which includes patients with cirrhosis and some non-cirrhotic hepatitis B carriers [7]. In a study from Taiwan (blog post: HBV Vaccination Prevents Cancer), the authors showed the beneficial effects of vaccination: HCC incidence per 105 person-years was 0.92 in the unvaccinated cohort and 0.23 in the vaccinated birth cohorts. This study also showed how rare HCC cases are in children; thus, showing benefit of vaccination was impressive.
My take: This case report is helpful in emphasizing the risk of HCC in patients with HBV, even in those without significant risk factors. However, at this time most experts do not recommend surveillance in those with a low risk of developing HCC.
HBV Vaccination Prevents Cancer In Taiwan: HCC incidence per 105 person-years was 0.92 in the unvaccinated cohort and 0.23 in the vaccinated birth cohorts.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
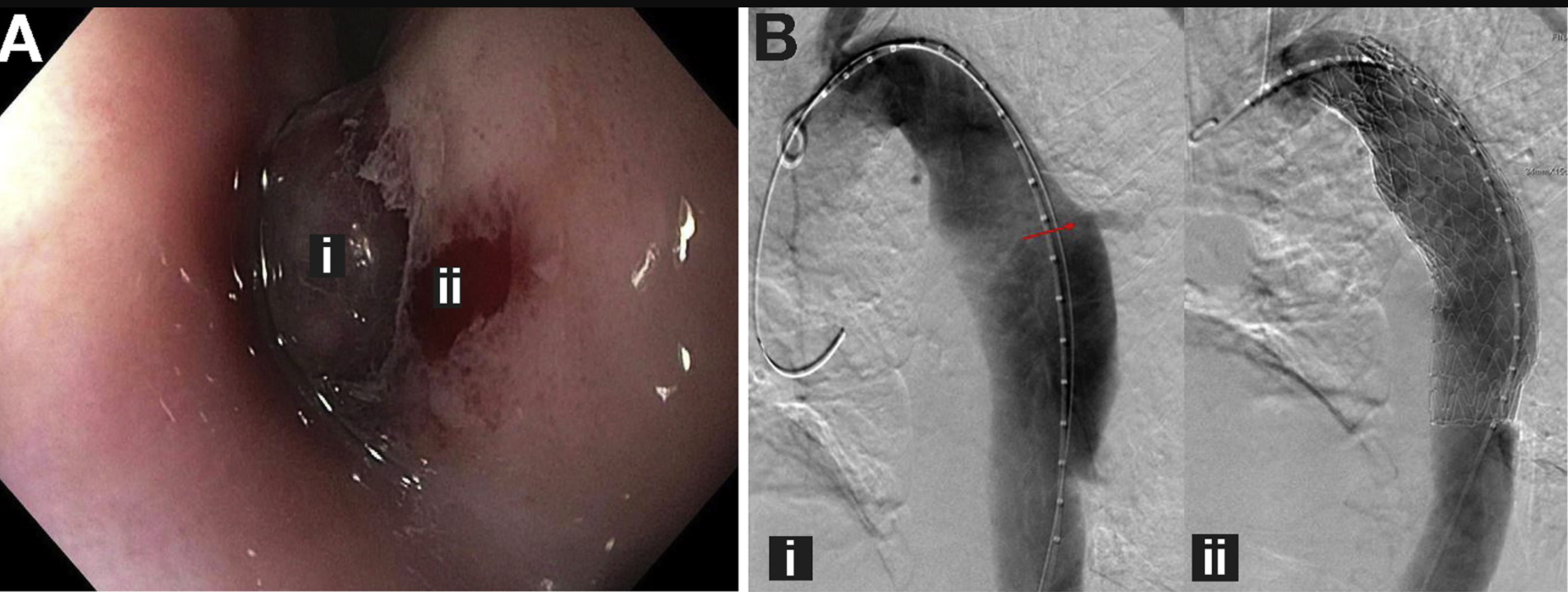
The authors recognized a “visible thoracic aorta eroding into the esophagus through a large transmural defect (FigureA) and a nonbleeding aortoesophageal fistula (FigureB) directly superior to the erosion in the middle third of the esophagus. This 76 year old patient had a known thoracic aortic aneurysm.
My take: This is an amazing case report because the patient survived. It is very easy to imagine the circumstance of massive exsanguination. In all patients with known cardiac repair and disease, it is important to consider the possibility of an major vessel fistula into the esophagus in those presenting with significant hematemesis and to consider how this could be managed.
In this prospective study of 50 patients with IBS (ROME III, all subtypes), with and without serologic reactivity to gluten (antigliadin IgG and IgA), and 25 healthy subjects (controls) were studied before and after 4 weeks of a GFD. Celiac disease (CD) was ruled out in patients and controls by negative tissue transglutaminase (tTG) IgA antibody and deamidated gliadin IgA or IgG antibodies and by the absence of mucosal atrophy in a duodenal biopsy specimen (Marsh 0 or 1). At least 4 and 2 biopsy specimens were obtained from the second and the first part of the duodenum, respectively.
Key findings:
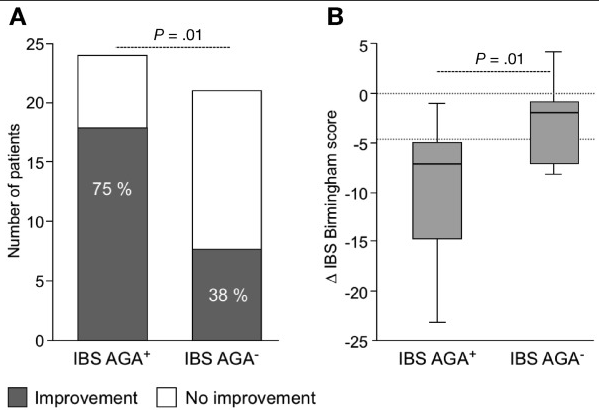
Compared with baseline, IBS symptoms improved in 18 of 24 patients (75%) with antigliadin IgG and IgA and in 8 of 21 patients (38%) without the antibodies
(A) Improvement in IBS symptoms (>4.5 points in the total Birmingham score) in antigliadin antibody (AGA)+ and AGA– patients after GFD. (B) Change in IBS symptoms after a gluten-free diet (GFD) compared with baseline in AGA+ and AGA– patients.
“A key trigger for symptom generation in IBS is diet, with more than 80% reporting food-related symptoms…It seems that wheat is a key component for symptom generation in IBS, as demonstrated by a study in 920 patients by Carroccio et al,8 which identified wheat sensitivity in 30% of patients”
The authors note that the Pinto-Sanchez population had a higher-than-expected rate of AGA positivity of 50% when previous studies have found rates of 7-18%.
My take: This prospective study indicates that a GFD is associated with clinical improvement in a significant number of individuals with IBS (with and without antigliadin antibodies) who did not report any gluten sensitivity or were not on a gluten-restricted diet before study entry. Based on a number of other studies, however, it seems that a low FODMAPs diet is likely to have a higher efficacy for patients with IBS.
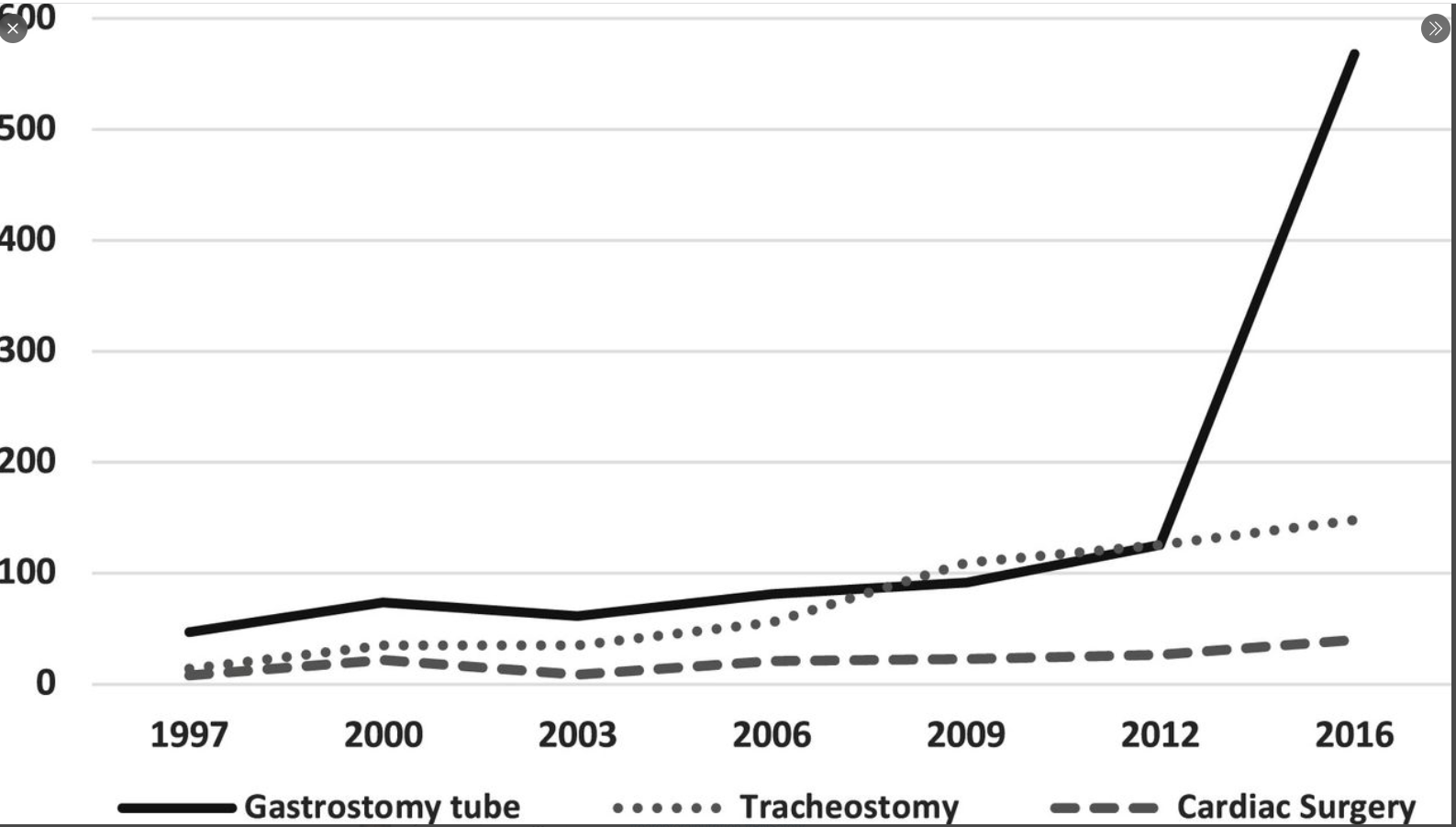
Methods: A retrospective analysis using the Kids’ Inpatient Database from 1997 to 2016 (10,151 admissions) was performed for trisomy 18.
Key Findings:
Gastrostomy tube placement increased 12-fold during the study period, tracheostomy increased 11-fold, and cardiac intervention increased 5-fold
The overall mortality rate (based on inpatient data) decreased in those with trisomy 18 from 32% in 1997 to 21% in 2016
Limitations: their data are limited to only hospitalized children and do not include all patients with trisomy 18 or capture population incidence
My take: This study documents a change in the approach to treating children with Trisomy 18. Compared to 20 years ago, these children are being offered more medical/surgical treatments rather than only palliative interventions.
Background: “Despite the progress made over the last 40 years the rate of indeterminate cases [of acute liver failure] remains ~30%”
Methods: The authors identified 41 children (<10 yrs) with DNA sample availability who were admitted to King’s College Hospital, London, with ALF of indeterminate etiology (2000-2018). In addition, trio exome sequencing was performed on 4 children admitted during 2019.
Key Findings:
Homozygous and compound heterozygous variants were identified in 8 out of 41 children (20%) and 4 out of 4 children (100%) in whom targeted and exome sequencing were carried out, respectively
The genes involved were NBAS (3 children); DLD (2 children); and CPT1A, FAH, LARS1, MPV17, NPC1, POLG, SUCLG1, and TWINK (1 each). Variants in NBAS and mitochondrial DNA maintenance genes were the most common findings.
My take: Genetic testing for underlying metabolic/metabolic disorders is important to further determine the reasons for ALF. Given the potential need for liver transplantation, obtaining these results quickly will be crucial. In addition, interpretation of the results in some cases will be difficult.
Two phase 3 placebo-controlled trials with the immune modulator risankizumab demonstrated control of Crohn’s disease whether or not patients had previously received a biologic agent.
Rates of clinical remission at 12 weeks with the interleukin (IL)-23 inhibitor risankizumab (Skyrizi, AbbVie), were about 48% in patients without prior exposure to biologic therapy and more than 40% in those with prior exposure…
The two trials, ADVANCE and MOTIVATE were presented together at the 2021 Digestive Disease Week (abstract 775a)…
Only 12% of patients in the placebo group achieved endoscopic remission versus 40.3% of those on the 600-mg dose of risankizumab (P<0.001). [Rates of endoscopic remission were higher in the biologic-naive (50.5%)]
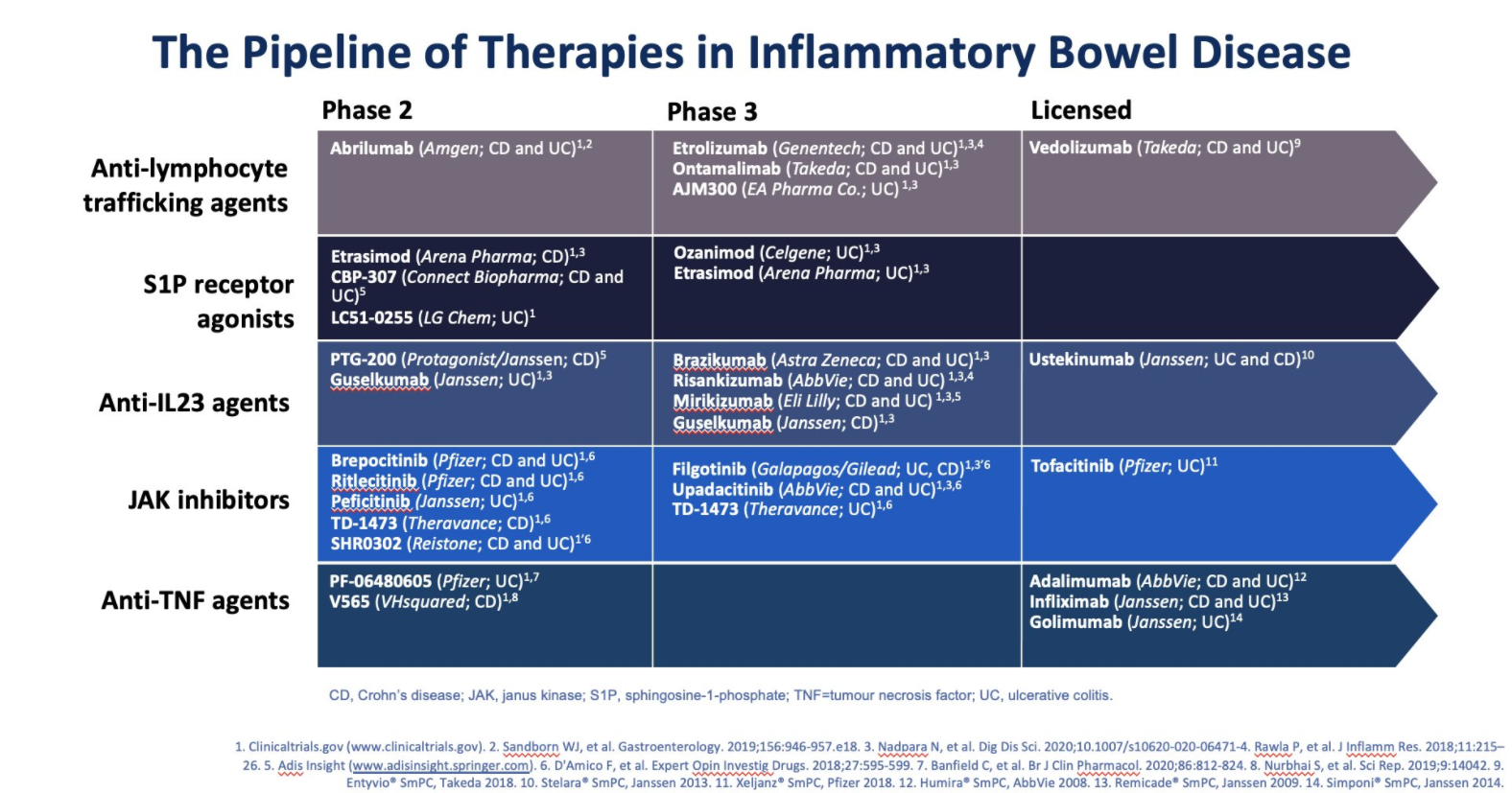
My take: In addition to ustekinumab (already approved), a number of other therapeutic agents that target IL-23 are likely to be available soon to help manage Crohn’s disease. This includes risankizumab but others with phase 3 studies include brazikumab, mirikizumab, and guselkumab..
Slide from David Rubin Twitter Feed (March 2021). Ozanimod now approved.
The first head-to-head trial comparing ustekinumab and adalimumab has found the two drugs are similarly safe and effective in patients with moderate to severe Crohn’s disease…
Dr. Scherl and her co-investigators in the SEAVUE trial randomly assigned 386 biologic-naive patients with Crohn’s disease to receive one year of treatment with either ustekinumab or adalimumab at standard on-label doses, with no dose escalation throughout the study period and no concomitant immunomodulators...
The findings, which were presented at the 2021 annual meeting of the European Crohn’s and Colitis Organisation (oral presentation OP02), showed that after one year of treatment, 65% of patients who received ustekinumab and 61% of those who received adalimumab achieved clinical remission, defined as a CDAI below 150...[And] similar additional outcomes, including clinical response at one year (72.3% for ustekinumab vs. 66.2% for adalimumab), corticosteroid-free remission at one year (60.7% vs. 57.4%, respectively), endoscopic remission at one year (28.5% vs. 30.7%)
My take: This study indicates that ustekinumab likely has similar safety and efficacy as adalimumab (though the study did not allow dose escalation or immunomodulators); thus, it could be positioned as a first-line treatment. It is administered less frequently as well.
For those who have not followed the FDA’s controversial decision of approving Aducanumab for the treatment of Alzheimer’s disease, the NEJM has two useful commentaries:
“Biogen…has announced a list price of $56,000 –10 times the evidence-based benchmark recommended by the independent Institute for Clinical and Economic Review…if even 10% of U.S. patients with Alzheimer’s disease were prescribed aducanumab, drug spending for Medicare Part B would increase from $37 billion to $69 billion per year”
The authors note that Medicare Part B payments rely on average sales price (ASP) from private insurers rather than a direct negotiated price; thus, the higher the price for private plans (even if poorly covered), the higher the Medicare rate
Hospitals and physicians are incentivized at higher prices due to receiving a 4-6% reimbursement price over the acquisition price
“The $56,000 price for aducanumab is a rational manufacturer response to an irrational insurance system.”
Key points -from 2nd article:
By one estimate, the potential cost will exceed the budgets of agencies such as EPA or NASA
“In granting accelerated approval to aducanumab, the FDA concluded that the drug’s ability to reduce amyloid plaques was reasonably likely to translate into clinical benefits. But this claim is hotly contested and was not presented to the FDA’s advisory committee, which voted against recommending approval of the drug because of the lack of a demonstrated clinical benefit”
If Medicare refuses to cover medication, this would leave a burden to state budgets. “As a legal matter,…state Medicaid programs are required to cover nearly all FDA-approved drugs.”
“Congress could adopt new legislation specifying that state Medicaid programs need not cover aducanumab…Protecting state budgets shouldn’t require Medicare to cover an expensive drug with unproven clinical benefits.”
My take: This type of huge fiscal burden may provide the rationale for Medicare and Medicaid to reexamine whether/how they cover expensive FDA-approved medications.