ASPEN website: 2021 Parenteral Nutrition Multivitamin Product Shortage Considerations

Related Blog Posts:

ASPEN website: 2021 Parenteral Nutrition Multivitamin Product Shortage Considerations
Related Blog Posts:
A terrific review of sickle cell disease (SCD) associated liver problems: F Lacaille et al. JPGN 2021; 72: 5-10. The Liver in Sickle Cell Disease
While the most frequent liver-related problem in individuals is cholelithiasis (>25% after age 5 yrs), a host of other problems can develop –this article is a good reference.
Key points:
Related blog posts:

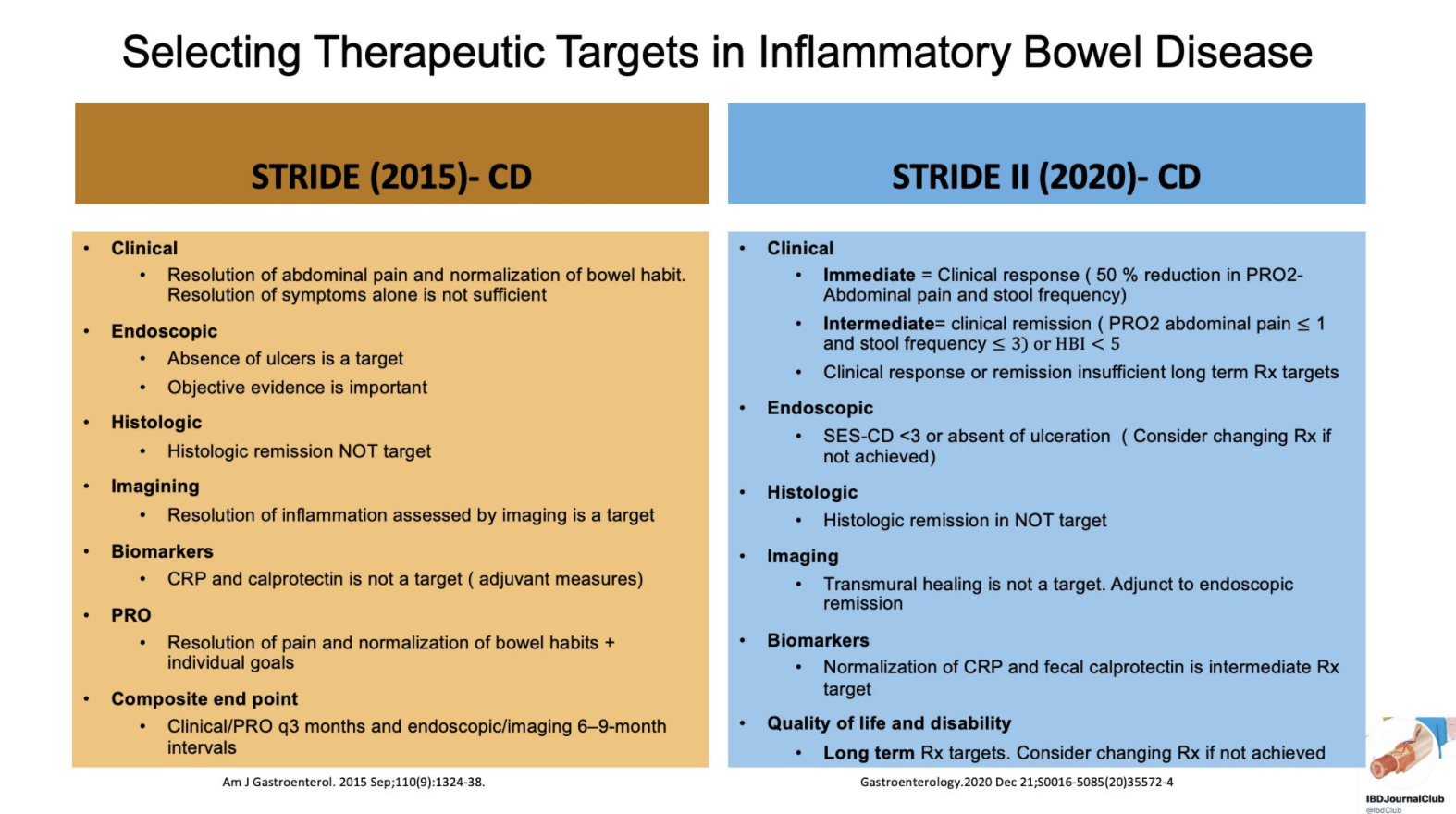
From Tauseef Ali’s Twitter Feed — a summary slide of Crohn’s disease targets for both pediatric and adult patients and a slide showing typical response/remission/healing times to medications.
From the following article: D Turner et al. Gastroenterology (12/31/20, Online Ahead of Print): DOI: 10.1053/j.gastro.2020.12.031 STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD
Recommendations were based on a systematic review of the literature and iterative surveys of 89 IOIBD members, recommendations were drafted and modified in two surveys and two voting rounds.

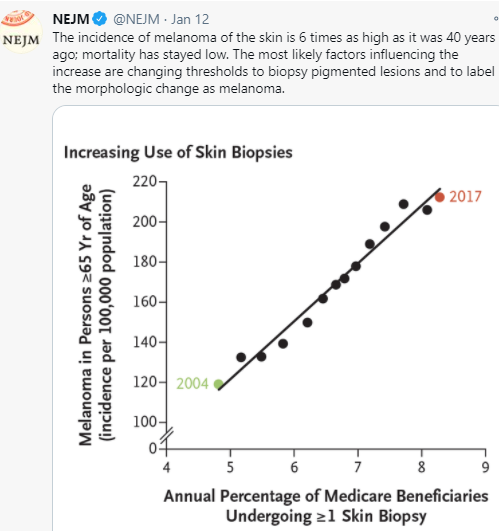
It would seem intuitive that screening for melanoma in at-risk pediatric patients would be worthwhile. And, this has been recommended in pediatric patients with inflammatory bowel disease who have received medications which increase the risk. However, a recent article (HG Welch et al. NEJM 2021; 384: 72-79. The Rapid Rise in Cutaneous Melanoma Diagnoses) provides a lot of reason to question this practice;. This article did not focus on pediatrics but its message about overdiagnosis of melanoma is applicable to this population as well.
Key points:
My take: Routine visits to dermatology are difficult to justify in the absence of worrisome skin findings. “Although the conventional response has been to recommend regular skin checks, it is far more likely that more skin checks are the cause of the epidemic — not its solution.”
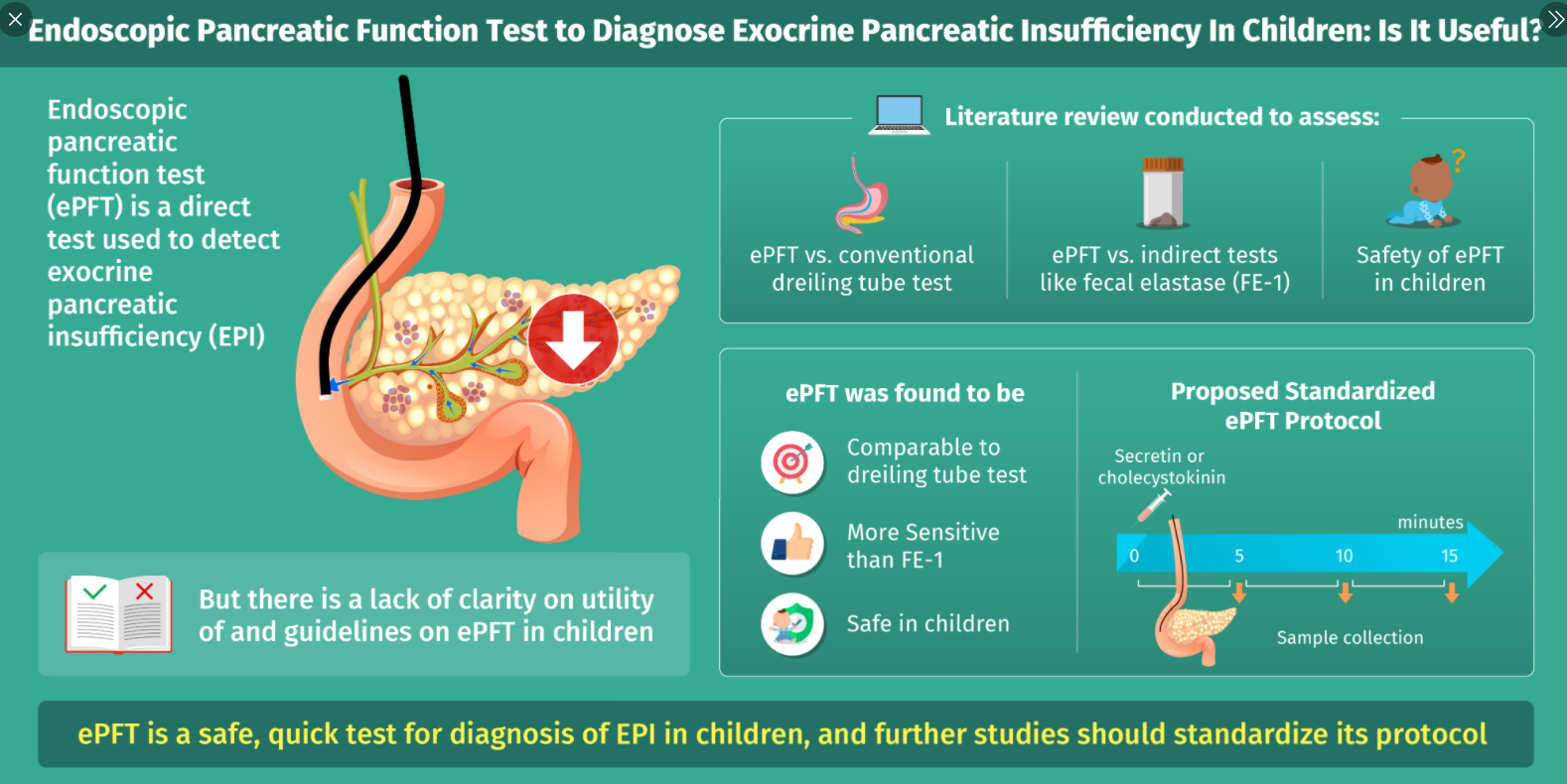
N Patel et al. JPGN 2021; 72: 144-150. full text Endoscopic Pancreatic Function Testing (ePFT) in Children: A Position Paper From the NASPGHAN Pancreas Committee
This articles serves as a good review of exocrine pancreatic insufficiency (EPI).
Etiologies:
Advantages/Disadvantages of Endoscopic Testing for EPI:
Endoscopic Testing Caveats:
My take: With careful clinical judgement, endoscopic EPI testing is rarely needed. First of all, fecal elastase measurements can detect most patients with EPI. In addition, a lot of patients with poor growth and suspected malabsorption are too young for reliable endoscopic EPI testing.
Related blog posts:


From BBC (1/25/21): Moderna vaccine appears to work against variants
An excerpt:
“For the Moderna study, researchers looked at blood samples taken from eight people who had received the recommended two doses of the Moderna vaccine. The findings are yet to be peer reviewed, but suggest immunity from the vaccine recognises the new variants. Neutralising antibodies, made by the body’s immune system, stop the virus from entering cells.
Blood samples exposed to the new variants appeared to have sufficient antibodies to achieve this neutralising effect, although it was not as strong for the South Africa variant as for the UK one. Moderna says this could mean that protection against the South Africa variant might disappear more quickly.”
AT Trout et al. JPGN 2021; 72: doi: 10.1097/MPG.0000000000002964 Free full text: North American Society for Pediatric Gastroenterology, Hepatology and Nutrition and the Society for Pediatric Radiology Joint Position Paper on Noninvasive Imaging of Pediatric Pancreatitis: Literature Summary and Recommendations. Also, I want to give a shout out to Jay Freeman who is one of the authors and a very appreciated colleague.
Some of the recommendations:
My take: This report provides a great deal of detail regarding the imaging modalities, terminology and diagnostic considerations for pediatric pancreatitis.
Related blog posts:

Briefly noted: S Sultan, SM Siddique et al. Gastroenterol 2020; 159: 1935-1948. Full text: AGA Institute Rapid Review and Recommendations on the Role of Pre-Procedure SARS-CoV-2 Testing and Endoscopy
Table 1 provides a summary of the recommendations and indicates a threshold for which routine pre-procedure testing may not be needed:
My take: Particularly after the rollout of vaccination to health care providers, routine testing for SARS-CoV-2 is not likely to be needed once the prevalence drops to low levels.
Related blog posts:

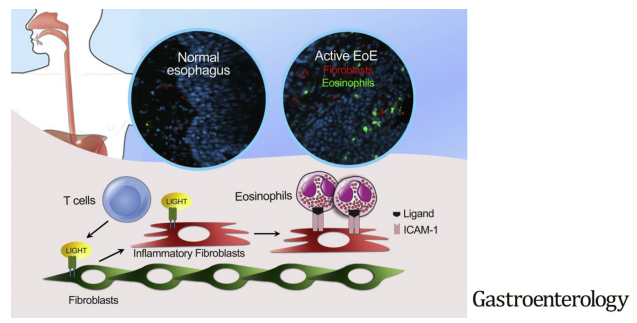
Briefly noted: MC Manresa et al. Gastroenterol 2020; 159: 1778-1792. Full text: Increased Production of LIGHT by T Cells in Eosinophilic Esophagitis Promotes Differentiation of Esophageal Fibroblasts Toward an Inflammatory Phenotype
The authors investigated the effects of tumor necrosis factor superfamily member 14 (TNFSF14, also called LIGHT) on fibroblasts in EoE.
Key findings:
My take: The authors show that patients with EoE had proinflammatory fibroblasts in the epithelium. Further, they show that eosinophil-fibroblast interaction was dependent on intact LIGHT signaling.
Related blog posts: