Listed below are the 10 ‘Best Practice Advice’ recommendations. I think the acknowledgement that “hemostatic powder should be preferentially used as a rescue therapy and not for primary hemostasis, except in cases of malignant bleeding or massive bleeding with inability to perform thermal therapy or hemoclip placement” (#7) is very useful.
“Best Practice Advice:”
Endoscopic therapy should achieve hemostasis in the majority of patients with NVUGIB.
This may include clips, thermal (heater probes, bipolar/multipolar catheters, hemostatic forceps), diluted epinephrine injection, and hemostatic spray
Initial management of the patient with NVUGIB should focus on resuscitation, triage, and preparation for upper endoscopy. After stabilization, patients with NVUGIB should undergo endoscopy with endoscopic treatment of sites with active bleeding or high-risk stigmata for rebleeding.
Endoscopists should be familiar with the indications, efficacy, and limitations of currently available tools and techniques for endoscopic hemostasis, and be comfortable applying conventional thermal therapy and placing hemoclips.
Monopolar hemostatic forceps with low-voltage coagulation can be an effective alternative to other mechanical and thermal treatments for NVUGIB, particularly for ulcers in difficult locations or those with a rigid and fibrotic base.
Hemostasis using an over-the-scope clip should be considered in select patients with NVUGIB, in whom conventional electrosurgical coagulation and hemostatic clips are unsuccessful or predicted to be ineffective.
Hemostatic powders are a noncontact endoscopic option that may be considered in cases of massive bleeding with poor visualization, for salvage therapy, and for diffuse bleeding from malignancy.
Hemostatic powder should be preferentially used as a rescue therapy and not for primary hemostasis, except in cases of malignant bleeding or massive bleeding with inability to perform thermal therapy or hemoclip placement.
Endoscopists should understand the risk of bleeding from therapeutic endoscopic interventions (eg, endoluminal resection and endoscopic sphincterotomy) and be familiar with the endoscopic tools and techniques to treat intraprocedural bleeding and minimize the risk of delayed bleeding.
In patients with endoscopically refractory NVUGIB, the etiology of bleeding (peptic ulcer disease, unknown source, post surgical); patient factors (hemodynamic instability, coagulopathy, multi-organ failure, surgical history); risk of rebleeding; and potential adverse events should be taken into consideration when deciding on a case-by-case basis between transcatheter arterial embolization and surgery.
Prophylactic transcatheter arterial embolization of high-risk ulcers after successful endoscopic therapy is not encouraged.
As an aside, I have always thought that the name, “Operation Warp Speed,” sounded like a line from the movie Spaceballs.
This article provides insight into the strategy for “Operation Warp Speed” (OWS). An excerpt:
OWS’s strategy relies on a few key principles. First, we sought to build a diverse project portfolio that includes two vaccine candidates based on each of the four platform technologies…In addition, advancing eight vaccines in parallel will increase the chances of delivering 300 million doses in the first half of 2021…
Of the eight vaccines in OWS’s portfolio, six have been announced and partnerships executed with the companies: Moderna and Pfizer/BioNTech (both mRNA), AstraZeneca and Janssen (both replication-defective live-vector), and Novavax and Sanofi/GSK (both recombinant-subunit-adjuvanted protein). These candidates cover three of the four platform technologies and are currently in clinical trials. The remaining two candidates will enter trials soon...
No scientific enterprise could guarantee success by January 2021, but the strategic decisions and choices we’ve made, the support the government has provided, and the accomplishments to date make us optimistic that we will succeed in this unprecedented endeavor.
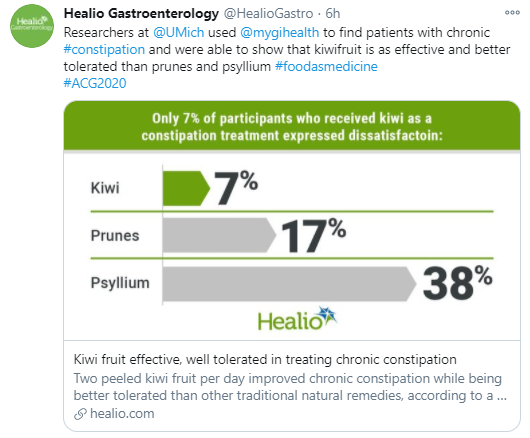
From a randomized (Virtual) ACG 2020 study from Samuel W. Chey and colleagues (University of Michigan), n=79 adults:
“All three treatments improved complete spontaneous bowel movement (P .003). Prunes demonstrated the largest magnitude of response at 67% vs. 64% for psyllium vs. 45% for Kiwi fruit”
“The highest proportion of participants – 68% – reported treatment satisfaction with kiwifruit while similar proportions of those receiving prunes and psyllium – 48% – reported satisfaction”
“The kiwi group had the lowest proportion of participants reporting treatment dissatisfaction at 7%….Participants receiving prunes and psyllium were more likely to report abdominal pain and bloating than those receiving kiwi”
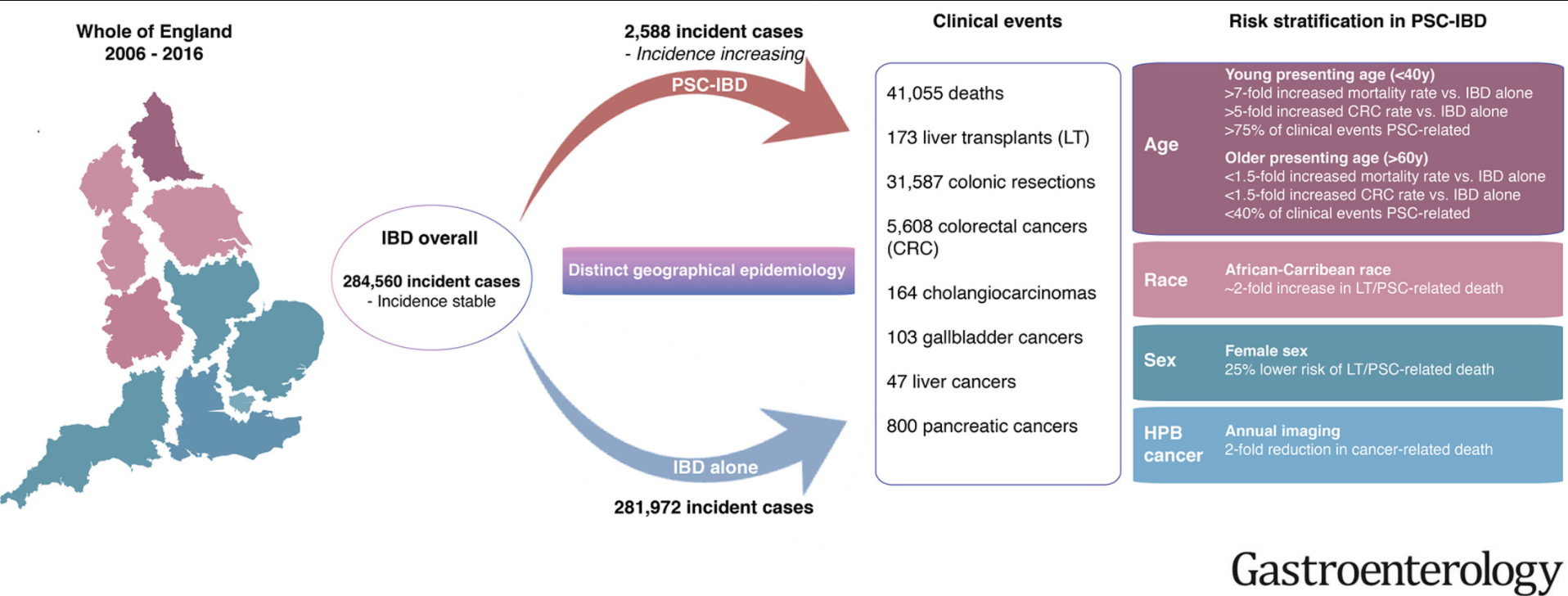
Methods: The authors linked prospectively collected data from national health care registries maintained for all adults in England on hospital attendances, imaging and endoscopic evaluations, surgical procedures, cancer, and deaths.
Key findings:
Over 10 years, we identified 284,560 incident cases of IBD nationwide; of these, 2588 patients developed PSC. This study excluded patients <18 years of age.
Development of PSC was associated with increased risk of death and CRC (hazard ratios [HRs], 3.20 and 2.43, respectively; P < .001) and a lower median age at CRC diagnosis (59 y vs 69 y without PSC; P < .001)
Compared to patients with IBD alone, patients with PSC-IBD had a 4-fold higher risk of CRC if they received a diagnosis of IBD at an age younger than 40 years
Development of PSC also increased risks of cholangiocarcinoma (HR, 28.46), hepatocellular carcinoma (HR, 21.00), pancreatic cancer (HR, 5.26), and gallbladder cancer (HR, 9.19) ( P < .001 for all)
The greatest difference in mortality between the PSC-IBD alone group vs the IBD alone group was for patients younger than 40 years
Patients with PSC-UC had >40% risk of colonic resection compared to patients with IBD alone (aHR 1.65)
My take: This study shows the impact the added diagnosis of PSC has for patients with IBD. One of the limitations in assessing outcomes is determining whether someone with IBD has PSC as there are a lot of patients with IBD who have asymptomatic changes in their biliary tree.
In an analysis (n= 279 adults, 70% female, average age 47 years) of patients with chronic constipation at a tertiary center who were referred for anorectal manometry, 19% had symptoms consistent with an eating disorder; this assessment was based on the Eating Attitudes Test (EAT-26).
“Gastrointestinal-specific anxiety fully mediated the relationship between the severity of ED pathology and constipation (standardized β, 0.11–0.16; P = .026–.024).”
The authors note that screening for eating disorders “is of particular importance before prescribing dietary interventions.”
My take: While this was a study with adults, it is likely that chronic constipation may be a presenting feature of an eating disorder in teenagers as well.
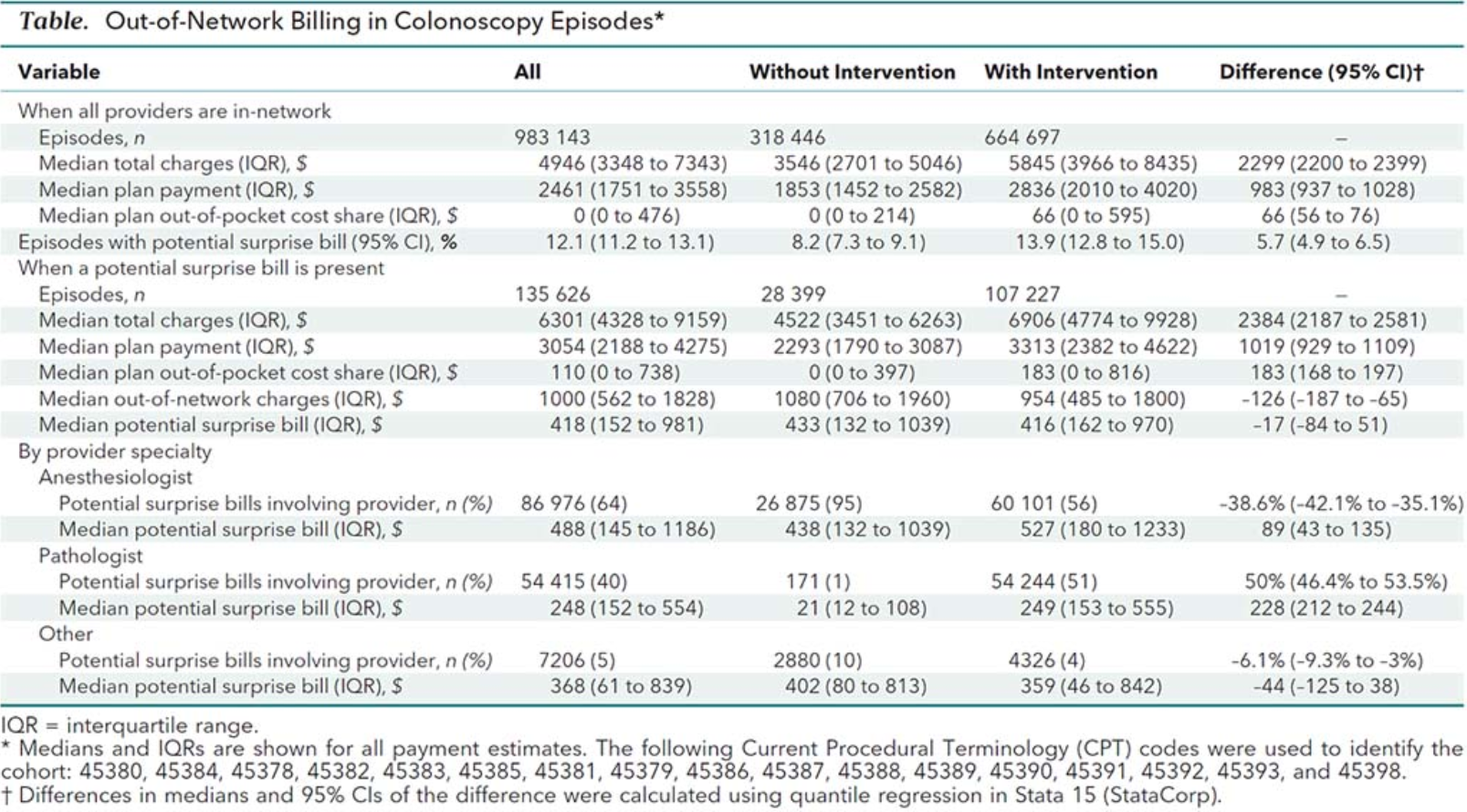
Background: “Federal law eliminates consumer cost sharing for multiple methods of colorectal cancer screening, including colonoscopy when done by an in-network provider. However, some patients having screening incur considerable out-of-pocket costs because out-of-network bills are not included in federal mandates. “Surprise billing” articles are widespread in the research literature and lay press . To date, the frequency of unexpected patient costs for screening colonoscopy have yet to be rigorously quantified.”
This study with ~983,000 procedures, which was conducted between 2012-2017, shows that it is common to get additional charges from a screening colonoscopy (which is supposed to be covered). Despite using an in-network physician, these charges can be due to “out-of-network” costs from anesthesia or pathology. This can also occur when anesthesia bills the colonoscopy as a diagnostic procedure rather than as a screening procedure.
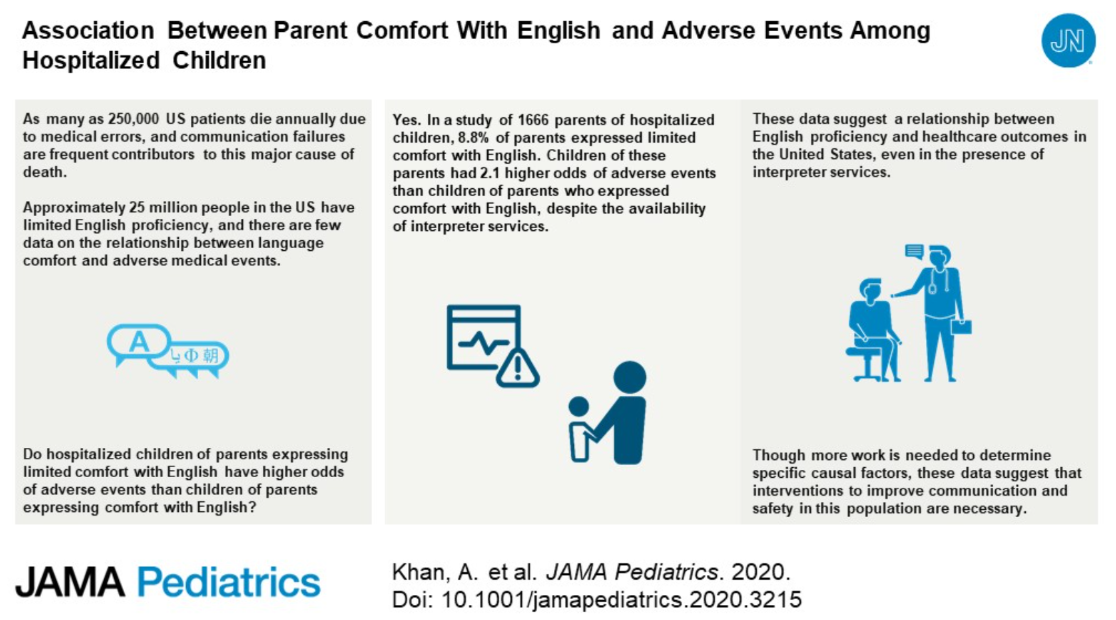
Key finding: Children of parents expressing LCE (limited comfort with English) had 2.1 higher odds of adverse events than children of parents who expressed comfort with English, after controlling for other factors.
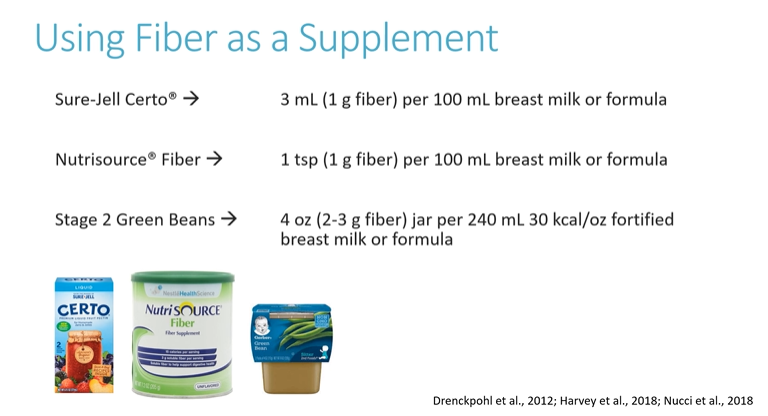
One useful resource for NASPGHAN members (NASPGHAN Nutrition Pearls) has been the short monthly nutrition pearl videos (about 10 of them so far). Here are some pointers from the most recent of these.
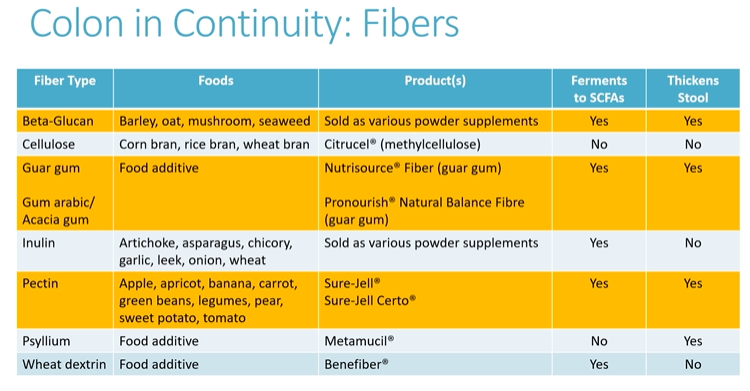
In October: Fiber for Short Bowel Syndrome –Beneficial for those with a colon in continuity:
Commercial products with limited data supporting use in short bowel syndromeAll of the fiber products are fermented in colon and may be beneficial. Highlighted products are more likely to help with stool consistency (thickening).
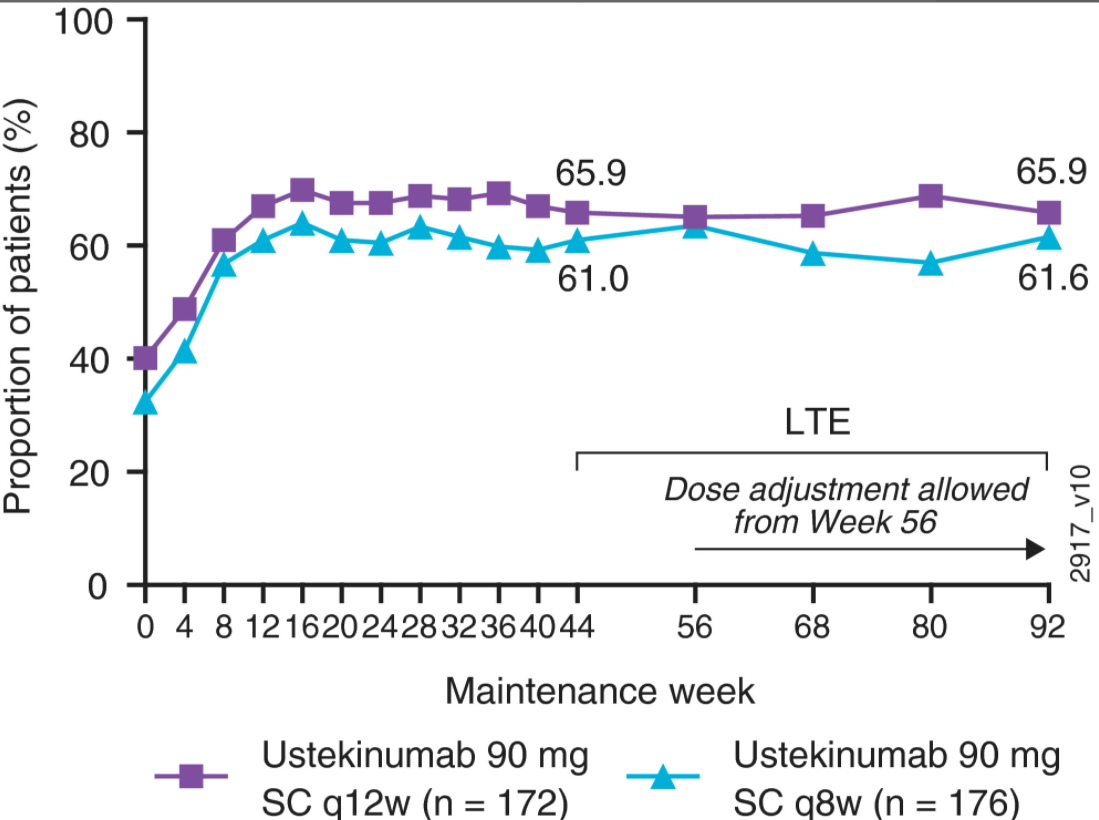
Methods: Overall, 399 (adult) “responders to intravenous ustekinumab induction and who were randomised to maintenance therapy were treated in the long‐term extension (115 received subcutaneous placebo, 141 received ustekinumab 90 mg every 12 weeks [q12w], and 143 received ustekinumab 90 mg q8w). Placebo treatment was discontinued at unblinding after week 44”
Key Findings:
Symptomatic remission rates (stool frequency = 0/1; rectal bleeding = 0) at week 92 were, 64.5% and 67.6% in the ustekinumab q12w and q8w groups, respectively ((Intent-to-treat population).
At week 44 of maintenance, measures of UC disease activity (eg Mayo scores) were generally comparable among patients randomised to ustekinumab q12w and q8w with 46.1% and 52.4% in clinical remission and 56.7% and 61.5% with endoscopic improvement respectively
Among randomised patients treated in the long‐term extension, 78.7% and 83.2% of patients receiving q12w and q8w, respectively, attained symptomatic remission at week 92; >95% of patients in symptomatic remission at week 92 were corticosteroid‐free
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition