Full report, NEJM, J Grein et al. April 10, 2020, DOI: 10.1056/NEJMoa2007016: Compassionate Use of Remdesivir for Patients with Severe Covid-19
53 of 61 had adequate data for inclusion. Indications of severe COVID-19: at baseline, 57% required mechanical ventilation and 4 (8%) were receiving ECMO.
With a median follow-up of 18 days, Key findings:
- 36 patients (68%) had an improvement in oxygen-support class, including 17 of 30 patients (57%) receiving mechanical ventilation who were extubated.
- 25 patients (47%) were discharged
- 7 patients (13%) died; mortality was 18% (6 of 34) among patients receiving invasive ventilation and 5% (1 of 19) among those not receiving invasive ventilation.
- By 28 days of follow-up, the cumulative incidence of clinical improvement, as defined by either a decrease of 2 points or more on the six-point ordinal scale or live discharge, was 84%
My take: Given the severity of the disease, this therapy looks promising. However, the authors note that “measurement of efficacy will require ongoing randomized, placebo-controlled trials of remdesivir therapy.”
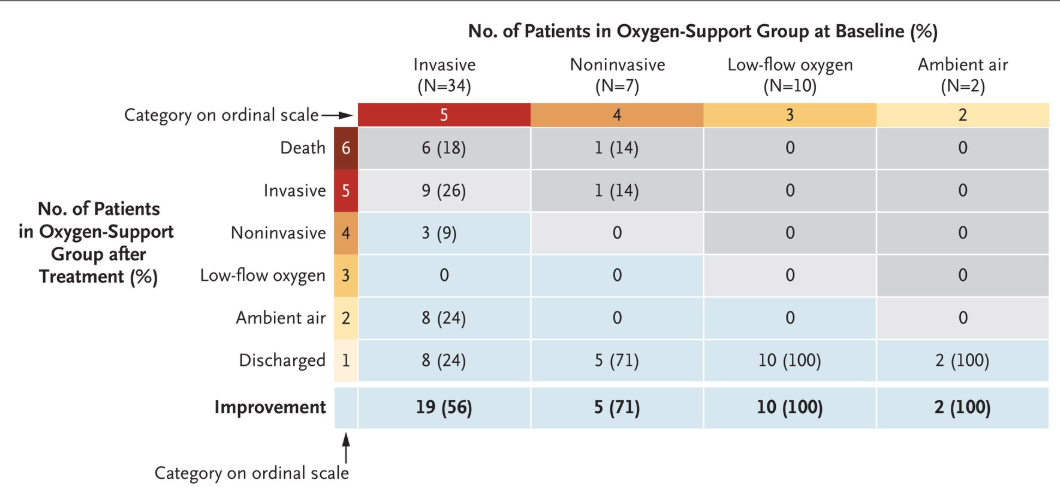
For each oxygen-support category, percentages were calculated with the number of patients at baseline as the denominator. Improvement (blue cells), no change (beige) and worsening (gray) in oxygen-support status are shown. Invasive ventilation includes invasive mechanical ventilation, extracorporeal membrane oxygenation (ECMO), or both. Noninvasive ventilation includes nasal high-flow oxygen therapy, noninvasive positive pressure ventilation (NIPPV), or both.