Here are some selected slides and notes from this year’s NASPGHAN’s postrgraduate course. With my notes, there could be errors of omission and transcription on my part.
Link to the full NASPGHAN PG Syllabus 2019 (Borrowed with permission)
Liver/Pancreas Session
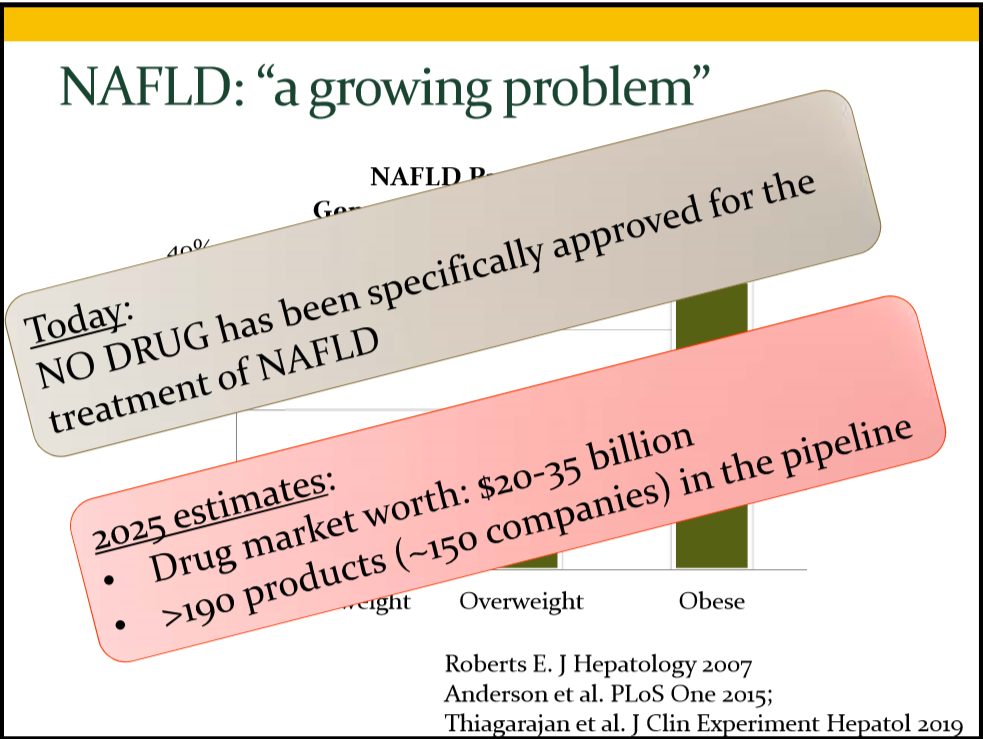
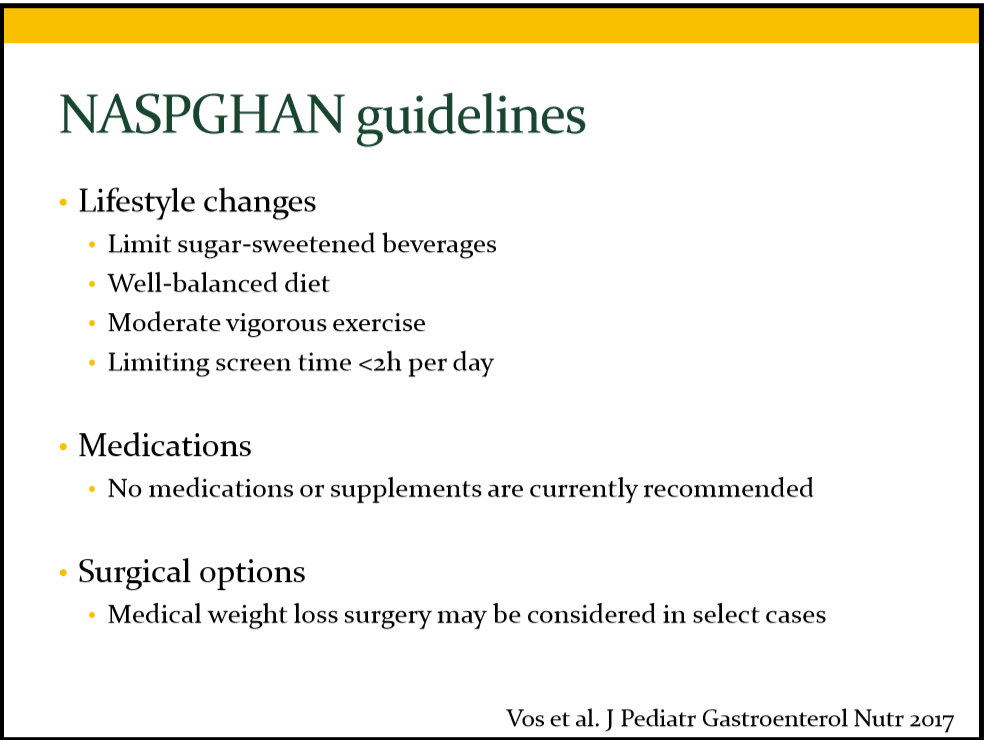
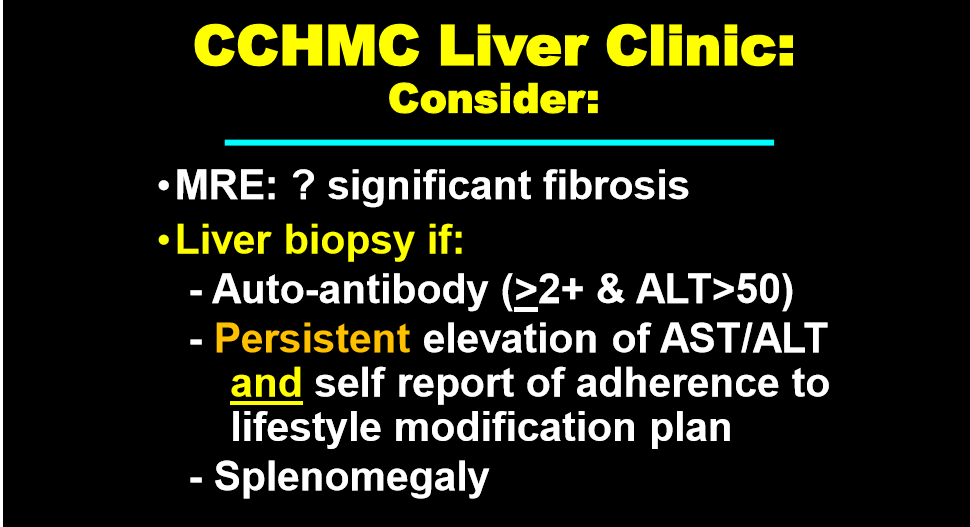
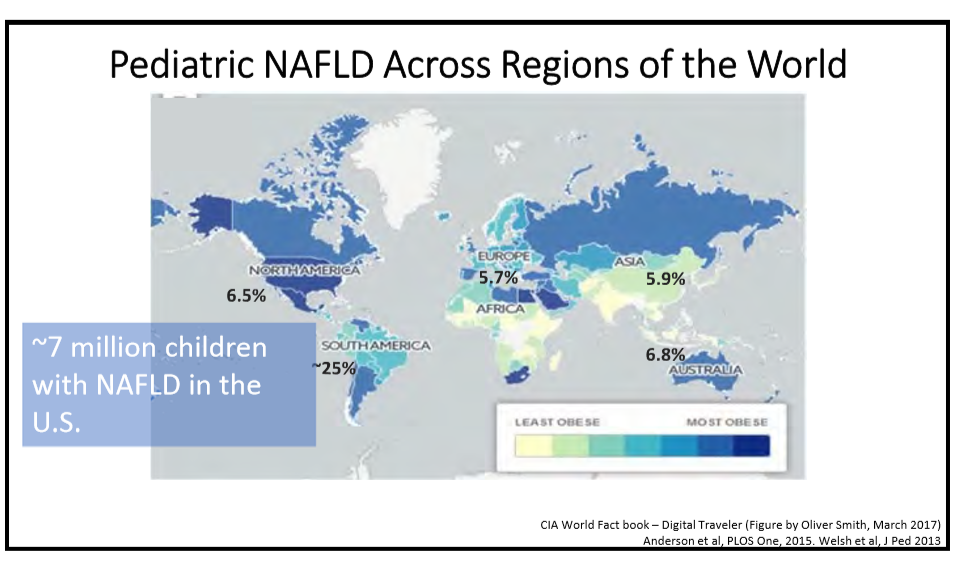
150 Miriam Vos, MD, MSPH, Emory University New news in NAFLD
Dr. Vos gave a terrific lecture. Key points:
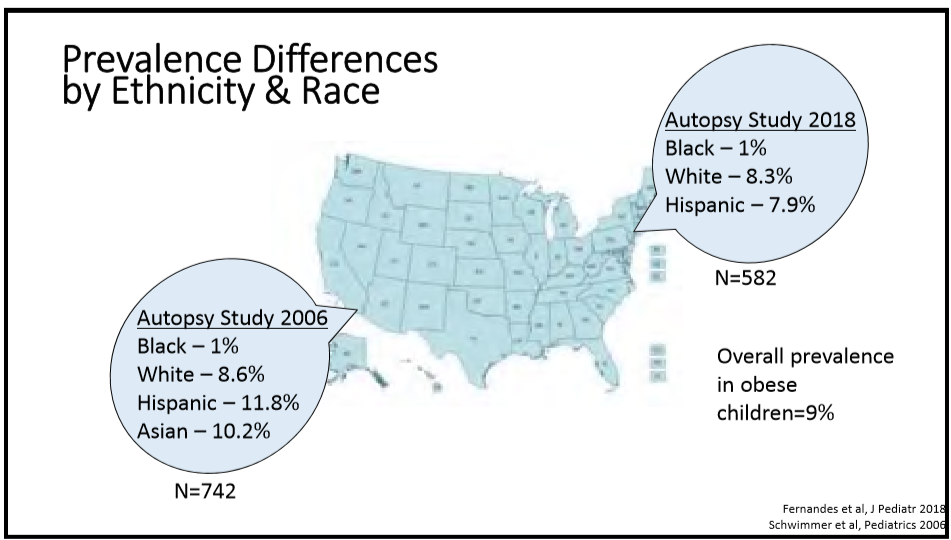
- NAFLD screening: recommended around age 10 years (in children with obesity) based on increasing prevalence with age
- PNPLA3 encodes adiponutrin –> important for clearing stored triglycerides. Common polymorphism PNPLA3 rs738409‐is associated with NAFLD
- Who to screen –all obese children >10 years. Overweight children with risk factors: Type II diabetes, Hispanic, Family history, Pituitary disorders (GH), Right sided abdominal pain
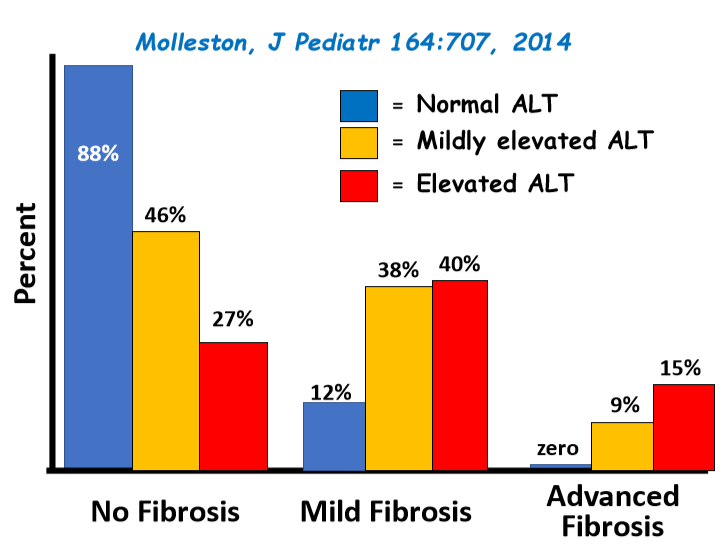
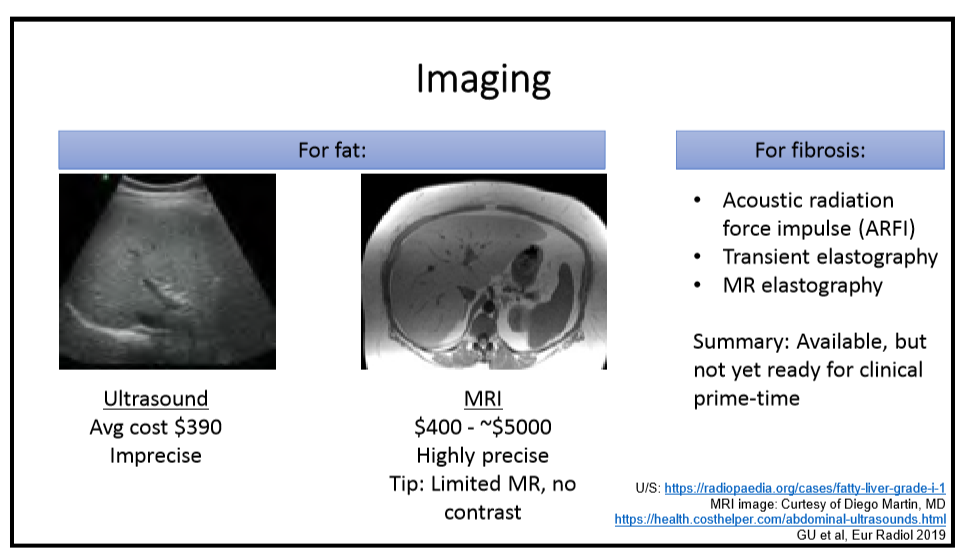
- ALT and ultrasound are imperfect screens
- Alcohol worsens NAFLD. Sugar/juice boxes are also culprits
- #1 Recommendation: Sugar reduction in diet
Related blog post: “The Paramount Health Challenger for Humans in the 21st Century”


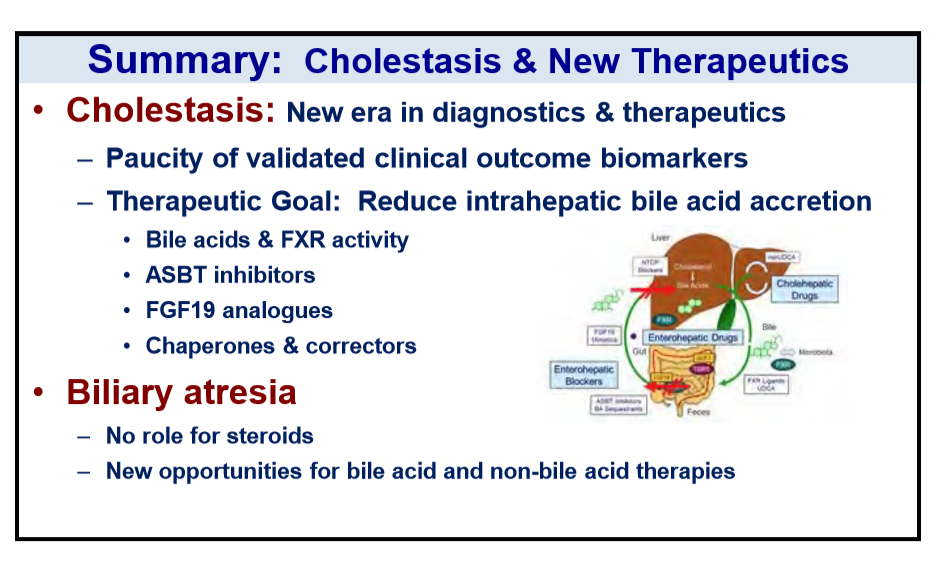
161 Saul J. Karpen, MD, PhD, Emory University School of Medicine/Children’s Healthcare of Atlanta New therapies for chronic cholestatic diseases
- Limited therapies currently available. A number of treatments appear promising: Obeticholic acid, Norursodeoxycholic acid
- For ABCB4, some drugs used for cystic fibrosis may help as well
- ASBT inhibitor appears promising for Alagille (see ITCH study)





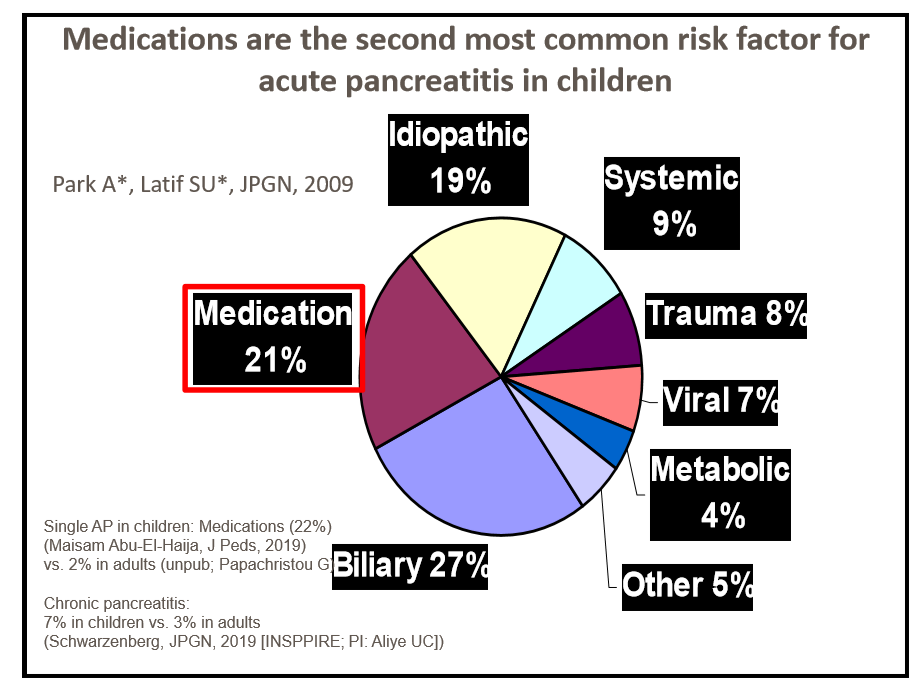
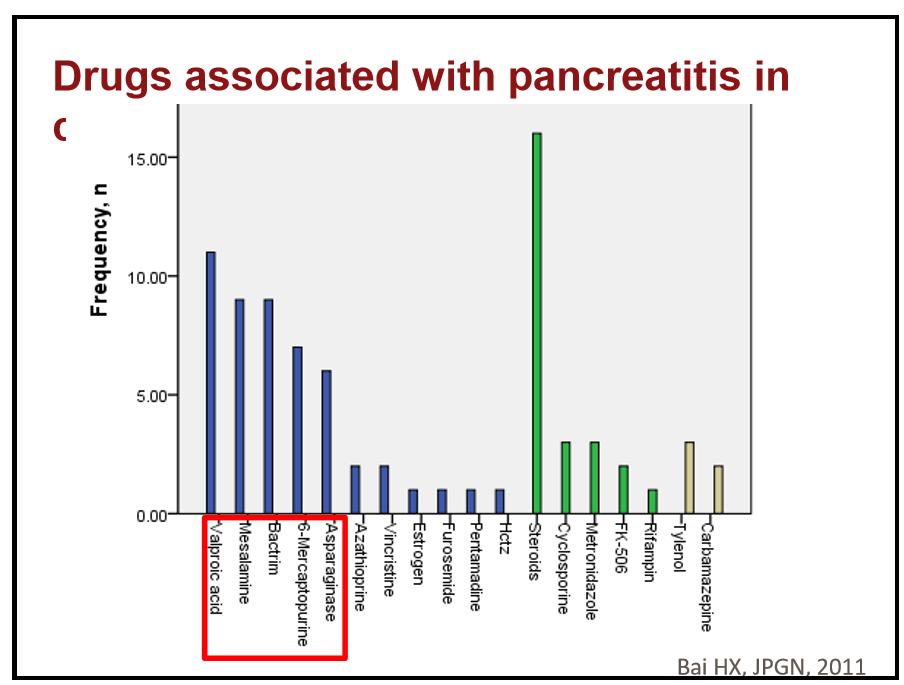
171 Sohail Husain, MD, Stanford Children’s Hospital Diagnosing drug-induced pancreatitis
- In patients with IBD, thiopurines and mesalamine/ sulfasalazine (mesalamine have greater risk than sulfasalazine) are associated with pancreatitis
- ~1/3rd of patients with drug-induced pancreatitis have other risk factors
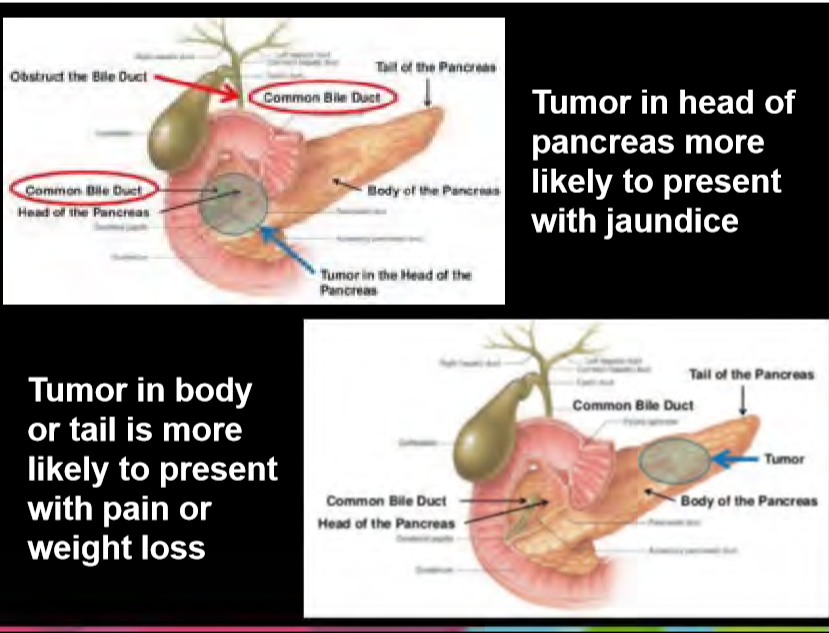
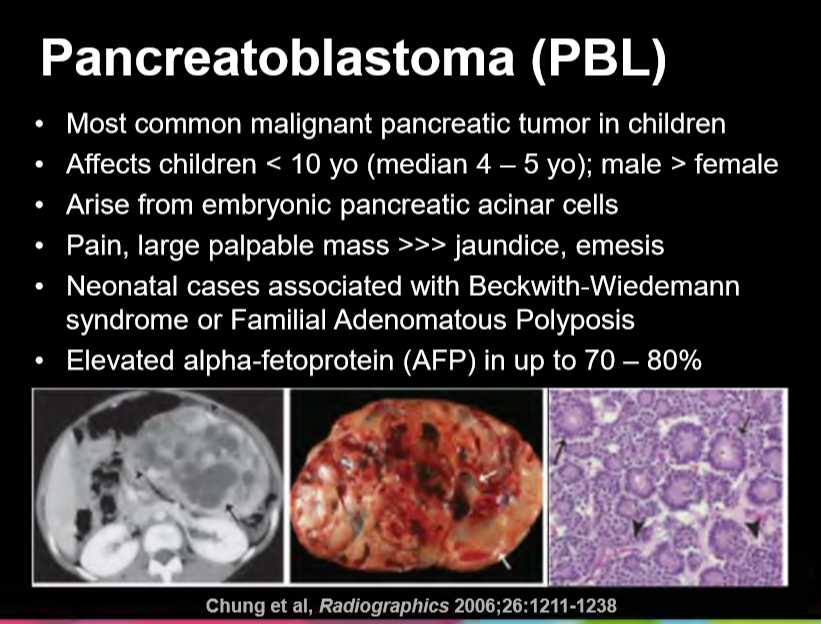
179 Jaimie D. Nathan, MD, FACS, Cincinnati Children’s Hospital Medical Center Pediatric pancreatic masses: Steroids, surgery or surveillance?



Disclaimer: NASPGHAN/gutsandgrowth assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. The discussion, views, and recommendations as to medical procedures, choice of drugs and drug dosages herein are the sole responsibility of the authors. Because of rapid advances in the medical sciences, the Society cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. Some of the slides reproduced in this syllabus contain animation in the power point version. This cannot be seen in the printed version.