The images below show how much more prevalent problems with regurgitation, colic, functional diarrhea, dyschezia, and functional constipation in the first 3 months of life compared to later in the first year of life.



The images below show how much more prevalent problems with regurgitation, colic, functional diarrhea, dyschezia, and functional constipation in the first 3 months of life compared to later in the first year of life.
A recent study (S Salvatore et al. J Pediatr 2019; 212: 44-51) examines the role of neonatal antibiotics and prematurity on the development of functional gastrointestinal disorders in the first year of life.
What is most striking, though, in this study is how many of these infants have a GI disorder.
Background: Prospective cohort multicenter study with 934 infants who completed study; n=302 premature, n=320 antibiotic recipients
Key findings:
Limitation: This study relied on parental reports which could overestimate infant’s symptoms.
My take: More than 75% of infants had at least one FGID.
Related blog posts:

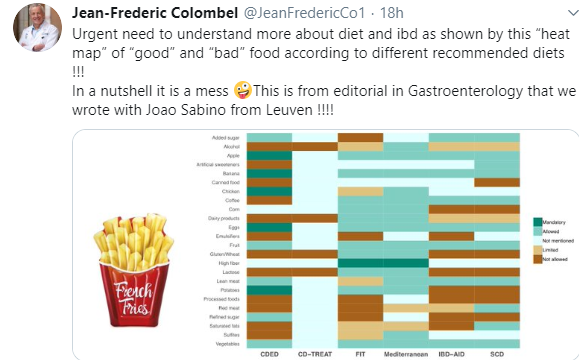
As noted in a previous blog (IBD Briefs August 2019), there have been numerous diets proposed to help with Crohn’s disease. The chart below illustrates the lack of any consensus.
Related blog posts:

A Carroccio et al. Clin Gastroenterol Hepatol 2019; 17: 682-90. This prospective study examined 78 patients with a diagnosis of non-celiac gluten sensitivity (NCGS) based on double-blind wheat challenge. The authors identified markers of inflammation including eosinophils in the duodenum and rectum of patients with NCGS: –the mean eosinophil infiltration was more than 2.5-fold the upper limit of normal in rectum and almost 2-fold in duodenum.
Rectal eosinophilia (>9 eos in the rectal lamina propria) had a sensitivity of 94%, specificity of 70%, positive predictive value of 81% and negative predictive value of 89% for NCGS.
My take: (from the editorial,pg 613-4) “In many cases, NCGS is likely a mislabeled functional GI disorder (IBS or FD) induced by wheat proteins or FODMAPs…tissue eosinophilia [is a] potential biomarker..although this observation needs further confirmation.”

Yummy! Though, probably the wrong place for those trying to be gluten-free
P Rosenthal et al. Hepatology 2019; 69: 2326-37. This study examined the efficacy and safety of combined entecavir and Peginterferon for immune-tolerant chronic hepatitis B-infected children (n=60). 48 weeks after completing treatment (week 96), 2 children (3%) achieved the primary outcome of undetectable HBeAg with HBV DNA levels <1000 IU/mL. These two children were also HBsAg negative/anti-HBs positive. In the other children (55 completed study), the ALT and HBV DNA levels were similar to baseline. 37 children experienced adverse events. My take: Entecavir/peginterferon is not very effective in immune-tolerant children infected with chronic HBV.
DL Thomas. NEJM 2019; 380: 2041-50. This article reviews the pathway to the global elimination of chronic hepatitis. Currently, it is estimated that hepatitis C virus (HCV) and hepatitis B virus (HBV) kill more than 1 million persons each year. “In fact, by 2040, deaths from chronic hepatitis are projected to exceed the combined mortality associated with HIV infection, tuberculosis, and malaria.”
JR Dillman et al. J Pediatr 2019; 212: 60-5. This study with 41 patients and 13 patients with biliary atresia prospectively assessed ultrasound shear wave elastography (SWE). The authors found that SWE with a cut-off value of >1.84 m/s had 92% sensitivity and 79% specificity. Also, in their cohort, GGT >320 had a sensitivity of 100% and specificity of 78%.
Z Younossi et al. Hepatology 2019; 69: 2672-82. This review provides a global perspective of NAFLD. 25% of the world’s population is currently thought to have NAFLD with highest prevalence in South America at 30.45% and lowest in Africa at 13.5%. This article usggest North America to have 24.1% prevalence rate.

Alpha-fetoprotein (AFP) levels are increased in >95% of patients with hepatoblastoma. These levels have to be interpreted carefully in infants as these levels typically are elevated in the first 6-12 months of life.
For patients with Beckwith-Wiedeman Spectrum (BWS), the relative risk of hepatoblastoma has been estimated to be 2280 times greater than the general population. In addition, in patients with BWS, AFP levels are known to be elevated compared to the general population in the absence of hepatoblastoma as well.
A recent study (KA Duffy et al. J Pediatr 2019; 212: 195-200) obtained 1372 AFP levels from 147 patients to establish normative values.
Table 2 -will be a useful reference. The authors found that AFP values were significantly higher in premature infants with BWS compared to full term and gradually approached normal levels around 12 months of life.
Some example AFP (95% CI) values from the entire cohort:
My take: This article will be very useful when monitoring for the risk of hepatoblastoma in patients with BWS
A recent cross-sectional study (LM Little et al. J Pediatr 2019; 210: 141-5) which examined sensory processing and constipaiton included 66 children and 66 control children.
Key finding:
The authors utilized the Child Sensory Profile-2 and the Toileting Habit Profile Questionnaire.
The finding that sensory problems contribute to chronic constipation. In those with over-responsiveness, which was more frequent in this study, this can lead to avoidance behaviors. In under-responsiveness, children may not realized that they need to defecate which can lead to problems as well.
My take: This study suggests that recognition of how sensory problems contribute to chronic constipation could improve counseling/treatment approaches.
Related blog posts:

Salt Creek Falls, OR
A recent study (JL Yasuda et al. JPGN 2019; 69: 163-70) shows that esophagitis is common with and without proton pump inhibitor (PPI) therapy in children with esophageal atresia (EA).
Background: This study encompassed 310 patients (34% long gap EA) and 576 endoscopies (median age 3.7 years)
Key findings:
While this is a large study, the findings have several limitations. This is a single center retrospective study and this center attracts highly complex cases of EA.
My take: In addition to fairly high rates of erosive esophagitis and eosinophilic esophagitis, this study shows a high incidence of microscopic esophagitis, the significance of this is unclear. This study supports the current recommendations of 3 endoscopies in childhood and perhaps more frequent surveillance in those with more complex EA.
Related blog posts:

Sign in Hood River, OR
A recent commentary (E Sepper. NEJM 2019; 381: 896-8) explains how the current administration’s “Protecting Statutory Conscience Rights in Health Care” policy will create additional problems for patients.
Background:
What is changing?
My take: In an effort to pander to religious communities, the administration is giving the green light to medical providers/staff to discriminate and deny services; this denial extends to even providing adequate information. The results of this policy could result in increased morbidity and even death in those denied services.

Pittock Mansion Hike, Portland, OR
WE Bennett, MD Pfefferkorn.
Full Link: Editorial: “Mental Health Screening as the Standard of Care in Pediatric Inflammatory Bowel Disease” Thanks to Ben Gold for this reference.
An excerpt:
Butwicka and colleagues1 have published a fascinating, landmark cohort study in this issue of JAMA Pediatricsassessing the prevalence of psychiatric diagnoses and symptoms among children with inflammatory bowel disease (IBD) in Sweden. The authors used a rigorous design that compared a cohort of more than 6000 pediatric patients with IBD with hundreds of thousands of healthy controls, as well as a separate cohort comprising the patients’ own siblings who did not have IBD. Butwicka et al1 computed hazard ratios for any psychiatric disorder, as well as for multiple specific disorders, and found a hazard ratio of 1.6 for any psychiatric diagnosis when comparing children with IBD with healthy controls. The statistical analysis is stellar and represents the best data we currently have on the intersection of pediatric IBD and mental health. Their study highlights a substantial risk in a vulnerable population and should trigger revision of guidelines and allocation of resources to support widespread screening and treatment for these dangerous conditions.
Related Article:
A Butwicka et al.
Full Text Link: Association of Childhood-Onset Inflammatory Bowel Disease With Risk of Psychiatric Disorders and Suicide Attempt
Related blog posts:

Crater Lake, OR
