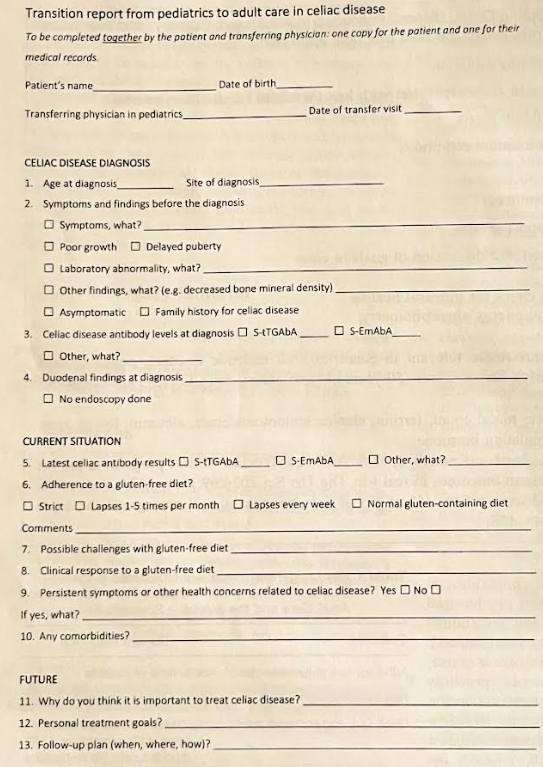
This clinical practice article offers some useful advice in transitioning patients with Celiac disease into adult provider care. Some of their recommendations for adult provider care:
Regular visits
Assessment of gluten-free diet adherence with low thresholf for dietician referral
H Kaplan et al. NEJM 2025; 392: 21: 2084-2086. Health Care in an Evolving Immigration Landscape — Providing Care while Upholding the Law
An excerpt:
In January 2025, the “sensitive locations policy,” which protected health care facilities and other designated areas from immigration enforcement activities, was rescinded. This change does not grant the officials unrestricted access to all areas of health care facilities or to patient information — the Fourth Amendment and the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule remain in place. Immigration officials may enter public spaces (e.g., lobbies) without consent, but they can access private spaces (e.g., exam rooms) only with a valid warrant or in exigent circumstances, such as threats to public safety…
Under the HIPAA Privacy Rule, health care professionals are not obligated to provide protected health information (PHI) to anyone without a judicial warrant or subpoena. The definition of PHI is expansive and includes a patient’s name, immigration status, and hospital discharge date. Administrative warrants from the Department of Homeland Security (such as Form I-200 or I-205) are not judicial warrants and do not compel health care professionals to disclose PHI. A judicial warrant must be signed by a judge and list a state court or U.S. district court on the document.
If an immigration official presents a judicial warrant or subpoena, health care professionals should verify its validity with their institution’s legal counsel before complying with it. They should escort the official away from private areas and document the official’s name and identification number, the nature of the request, and any actions taken, and obtain a copy of any documentation the official provides. They should not provide immigration officials with information beyond the scope of the warrant. When possible, they should avoid documenting a patient’s immigration status in the medical record, since that information could be used against the patient in legal proceedings….
If an official attempts to gain access to a private area by claiming there are exigent circumstances, legal counsel should be contacted. If an official forcibly enters a private area without legal authorization, staff should avoid physical confrontation, document the incident in detail (including names, badge numbers, and any statements made), and notify institutional leadership, their security team, and legal counsel as soon as possible…
In the past, immigration officials have pressured clinicians to transgress their clinical duties or to conduct evaluations or interventions that are not clinically indicated, such as certifying detainees’ fitness to travel for deportation…Without a court order, clinicians are not obligated to perform interventions that are not clinically indicated.
My take (borrowed in part from authors): “Health care professionals may face legal and ethical challenges as immigration policies evolve. By understanding their own legal rights and those of their patients, they can continue caring for patients while advocating for them and adhering to the law.”
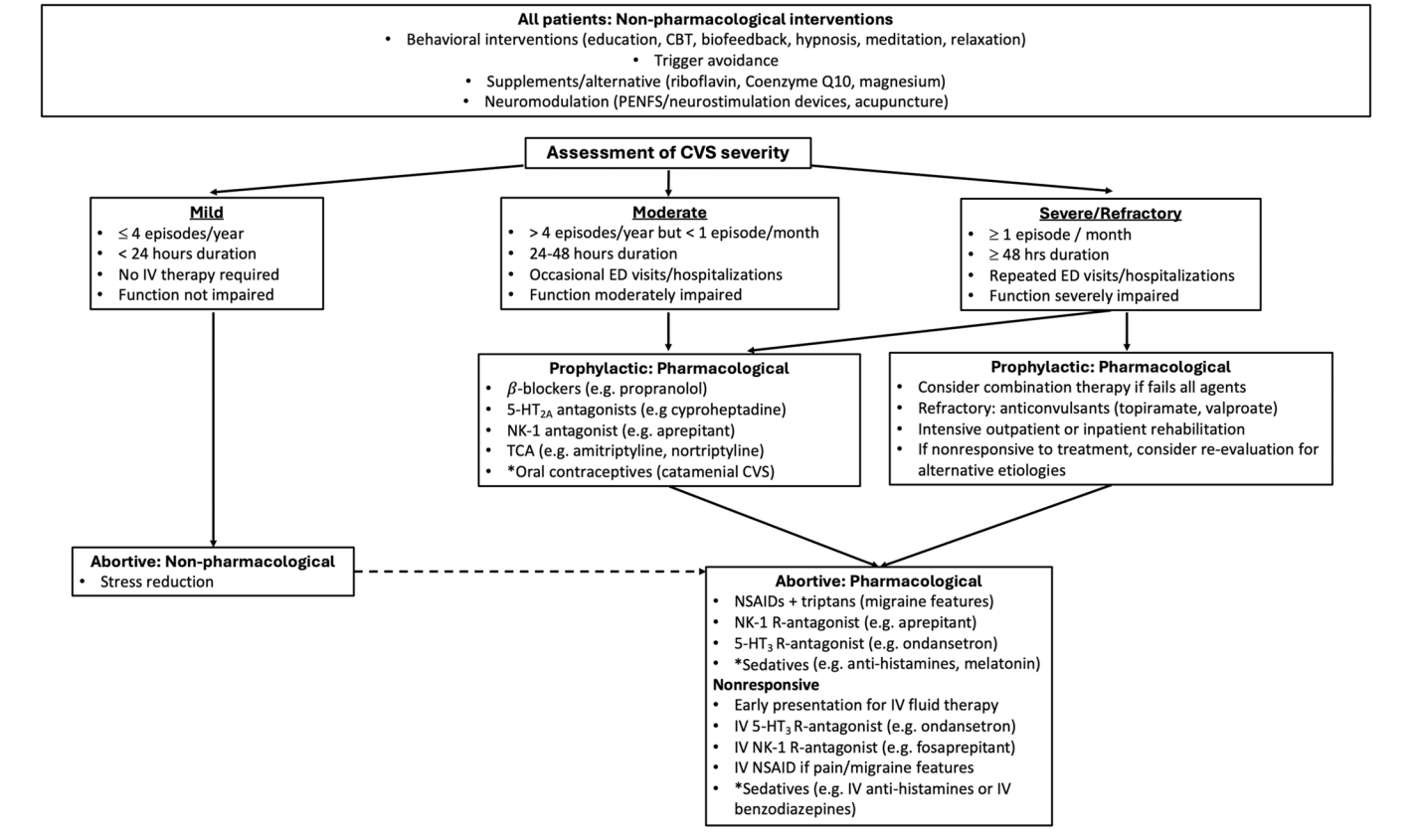
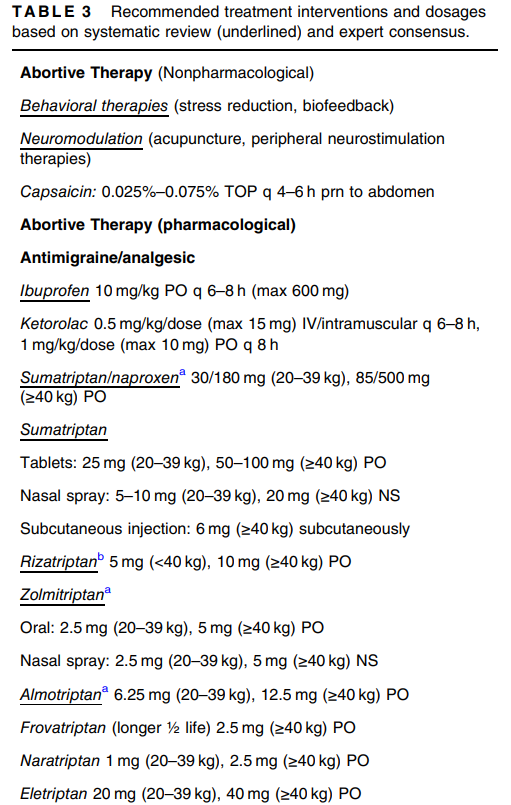
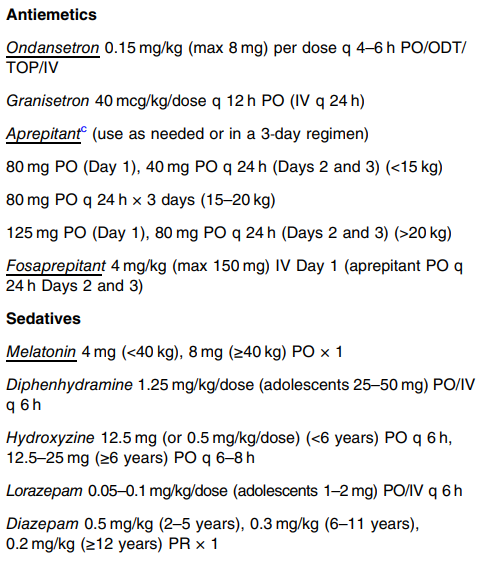
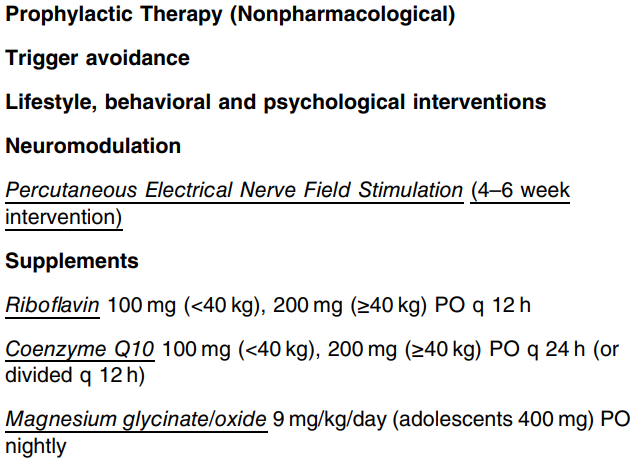
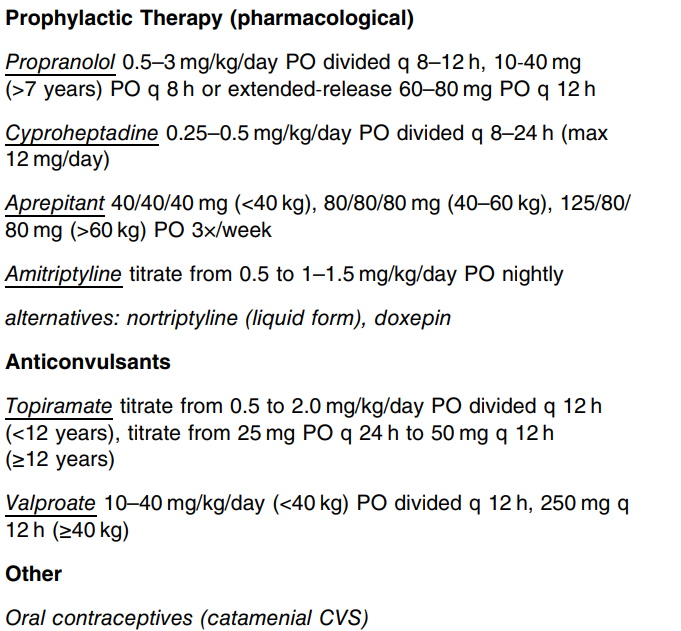
This is an excellent CVS guideline (36 pages). There is a lot of information and advice that is not easily summarized. Some important points:
Epidemiology: “The prevalence of pediatric CVS is estimated between 1.9% and 2.3% with an incidence of 3.2 per 100,000 children/year.1–3, 16 CVS peaks among school-aged children and often evolves into migraine headaches in adolescent years…17 56% of children experience resolution of CVS during a median follow-up of 29 months (range 6 months to 7 years)…A long-term follow-up study demonstrated progression to migraine in 26% of those with pediatric CVS.1“
Autonomic dysfunction: “An underlying autonomic dysregulation is also supported by clinical features during attacks (diaphoresis, listlessness, palpitations, and peripheral vasoconstriction), and a study shows that 40% of pediatric patients with CVS develop chronic dysautonomia during adolescence.18“
Cannabinoid hyperemesis syndrome: “CHS is considered a probable subtype of CVS that presents after prolonged and excessive cannabis use…26 Topical capsaicin, benzodiazepines, and droperidol or haloperidol have all been proposed as possible treatments for acute CHS episodes…50 Adult guidelines recommend that CHS patients be offered the same therapies as CVS patients…Complete cannabis cessation is the only known effective long-term treatment for CHS.”
Sato-variant: “This subtype manifests elevated levels of adrenocorticotropin hormone, cortisol, antidiuretic hormone, catecholamines, and prostaglandin E2, consequently presenting with hypertension and profound lethargy.25 While there is no published data for guidance, electrolyte monitoring is warranted, and episodic hypertension is generally managed by short-acting agents such as lisinopril or labetalol.”
L-carnitine: “The panel did not find evidence of efficacy other than when used in combination with coenzyme Q10 and cautioned against use based on concerns for atherosclerosis in animals.”
Propranolol: “The panel cautioned for use in patients with reactive airway disease…Retrospective studies showed high long-term efficacy of propranolol (57%–81%) when used as a first-line agent for pediatric CVS.155, 156 Two prospective, observational studies in pediatric CVS showed a high response rate to propranolol (77%–93%).157, 158 A larger (n = 81) randomized (uncontrolled and unblinded) trial demonstrated long-term effects of propranolol 1 mg/kg/day on both frequency and severity of CVS attacks with a 92% response rate and superiority over amitriptyline (53% response rate).159“
Cyproheptadine: “Using criteria of ≥50% improvement in outcomes of interest (episode frequency and duration), 55%–75% (retrospective to randomized) met this threshold. In pediatric migraine, 83% had a positive response.”
Aprepitant: “The use of aprepitant two or three times per week for prophylaxis resulted in significant improvement in several essential outcomes, including episode frequency, duration, intensity, symptom-free periods, hospitalization rates, and school attendance.69, 169 At the 12-month follow-up, 82% of children [n=95] achieved either partial or complete treatment response.”
Tricyclic Antidepressants (TCAs): “The panel suggests that this medication be reserved for those with more frequent and severe disease who have not responded to therapies with more favorable side effect profiles. Caution for possible behavioral changes, including suicidality, is indicated in all children and adolescents….Using the common criteria of ≥50% improvement as definition of response (complete or partial), 57% of pediatric and 81% of adult CVS patients responded.”
Anticonvulsants: “The guideline panel suggests not using anticonvulsants (e.g., topiramate or valproate) for preventing CVS episodes in children and adolescents, except for refractory CVS.”
My take: While data for CVS remains limited, these guidelines are likely to influence how CVS is managed in children.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
The United States will withdraw its financial support of Gavi, the global organization that helps purchase vaccines for children in poor countries, Robert F. Kennedy Jr., the United States secretary of Health and Human Services, told the group’s leaders on Wednesday, accusing them of having “ignored the science” in immunizing children around the world…
“Any decision made by Gavi with regards to its vaccine portfolio is made in alignment with recommendations by the World Health Organization’s Strategic Advisory Group of Experts on Immunization (SAGE), a group of independent experts that reviews all available data through a rigorous, transparent and independent process,” Gavi’s statement said…
Dr. Atul Gawande, a surgeon who led global health work in the Biden administration, called Mr. Kennedy’s remarks “stunning and calamitous…”
The United States was the largest donor to Gavi, whose work is estimated to have saved the lives of 17 million children around the world over the past two decades…
Gavi had hoped to raise $9 billion for the 2026-30 period, funds the organization said would allow it to purchase 500 million childhood vaccinations and to save at least eight million lives by 2030. ..
The decision to end U.S. support for Gavi — which was included in the rescission package passed by Congress and now being considered by the Senate — leaves the organization with an immense hole in its budget…The Gates Foundation is maintaining its funding at a stable level from previous years — about $350 million in each of the next four years — as is the United Kingdom.
My take: It is no exaggeration to say that the shift in U.S. vaccine policy may result in hundreds of thousands of deaths every year. In addition, U.S. travelers will be more likely to be exposed to vaccine-preventable illnesses as well.
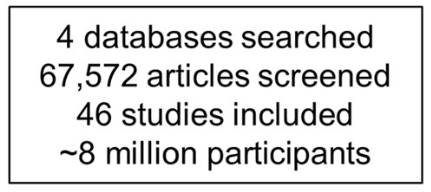
A total of 46 studies fulfilled the eligibility criteria, comprising approximately 8 million participants from 21 countries.
Key findings:
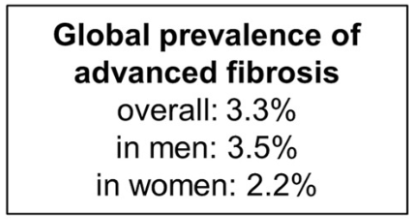
The pooled prevalence rates of advanced liver fibrosis and cirrhosis in the general population were 3.3% (95% CI, 2.4%–4.2%) and 1.3% (95% CI, 0.9%–1.7%) worldwide, respectively
Risk factors for cirrhosis were viral hepatitis, diabetes, excessive alcohol intake, obesity, and male sex
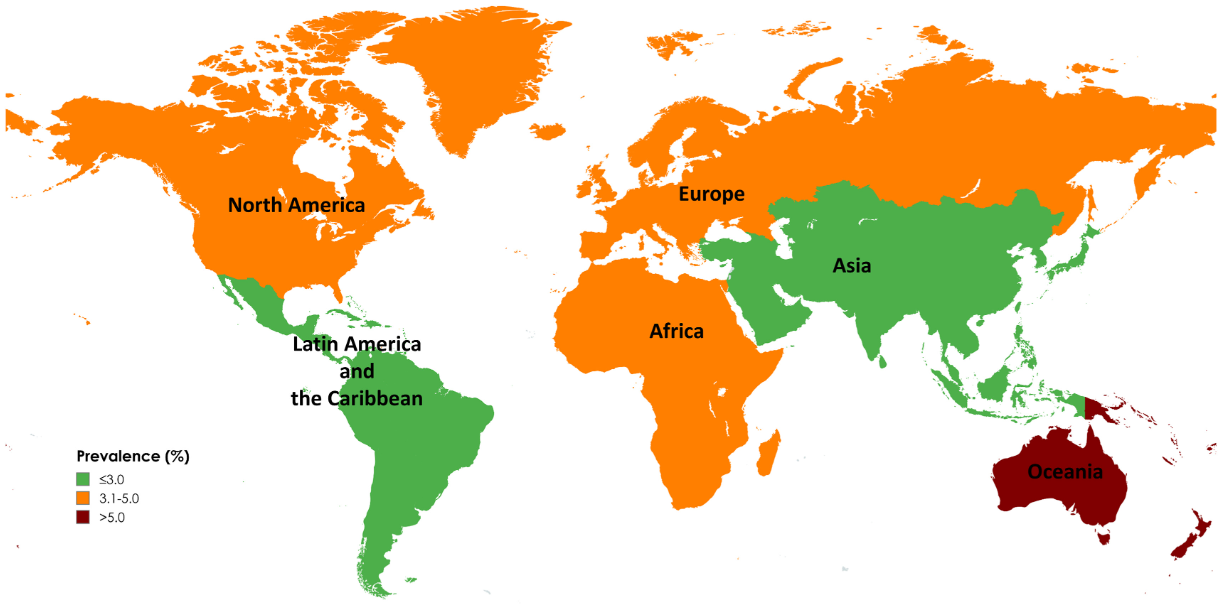
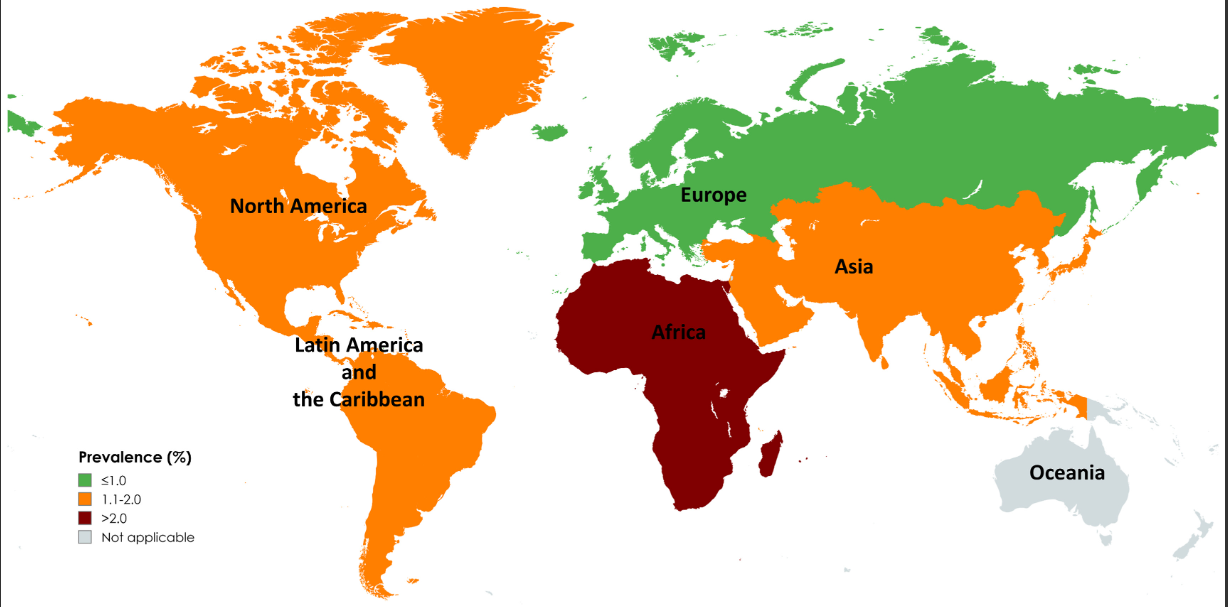
Limitations: 1. All included studies used noninvasive tests to diagnose advanced fibrosis and cirrhosis, which might overestimate prevalence in general populations. The diagnostic performance of these tests is influenced by baseline prevalence, leading to a higher rate of false positives in low-prevalence populations 2. Significant differences in prevalence by geographic region and time period. However, these differences could be influenced by variations in health care infrastructure, access to health care, and disease awareness, which may only partially reflect the true prevalence of advanced liver fibrosis and cirrhosis. In addition, the data is influenced by the number of studies (eg. Oceania had only 1 individual study).
Map of Global Prevalence of Advanced FibrossiMap of Global Prevalence of Cirrhosis
My take: This study provides estimates of the high and increasing prevalence of advanced liver fibrosis and cirrhosis. This data is essential in determining if we are making progress and how to mitigate the disorders leading to advanced liver disease.
Recently Dr. Balistreri gave our group an excellent lecture. I have taken some notes and shared some slides. There may be inadvertent omissions and mistakes in my notes.
Key Points:
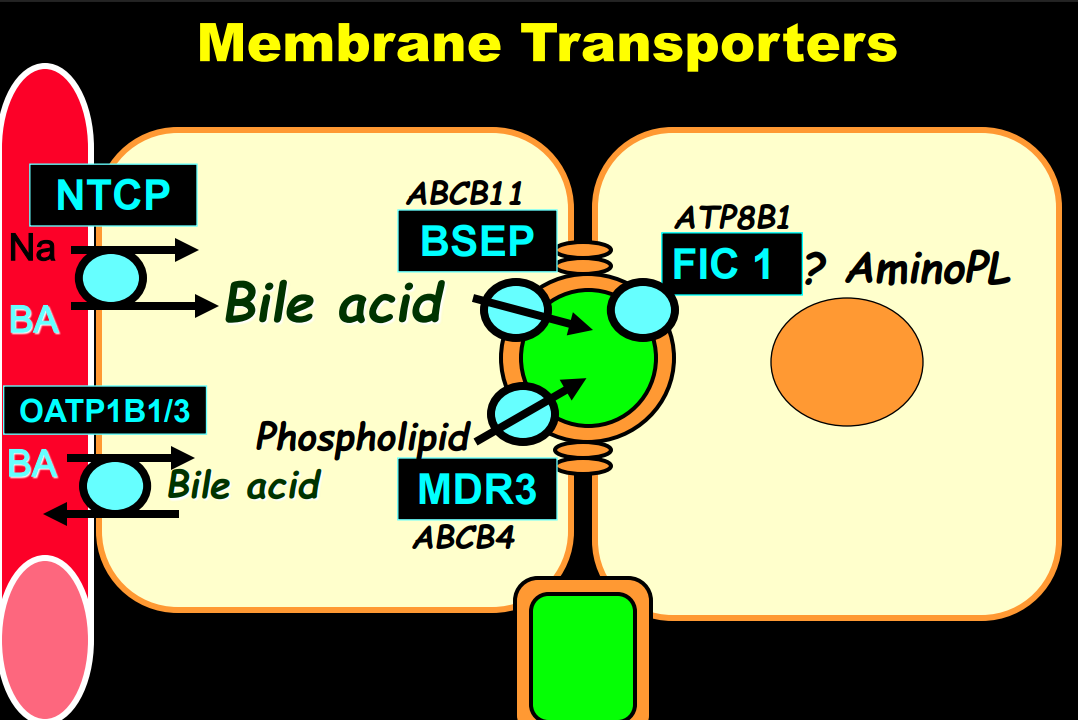
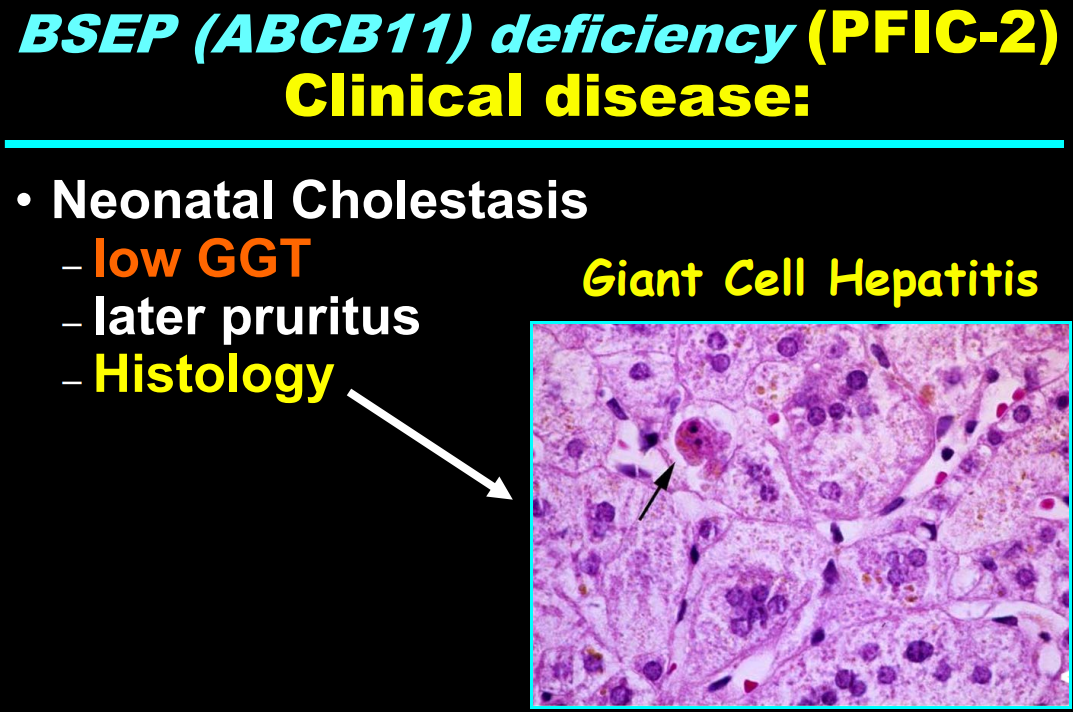
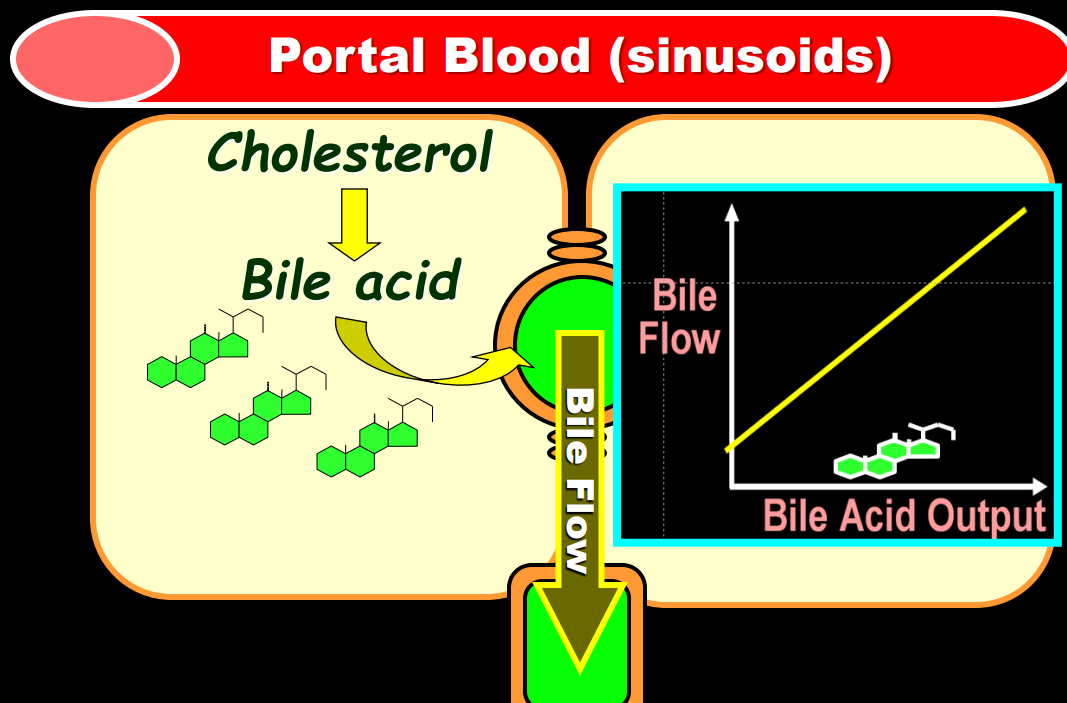
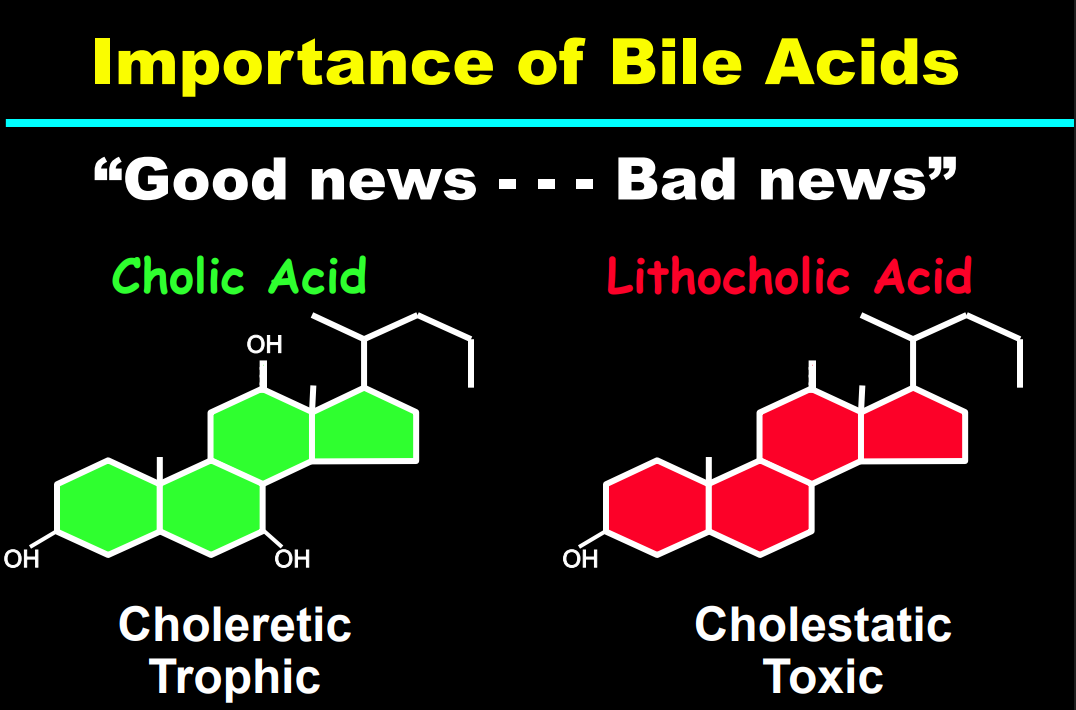
Producing enough bile acids and recycling bile acids in enterohepatic circulation is crucial for bile acid flow. In addition, there are ‘good’ bile acids like cholic acid that have trophic properties and ‘bad’ bile acids like lithocholic acid that cause liver toxicity
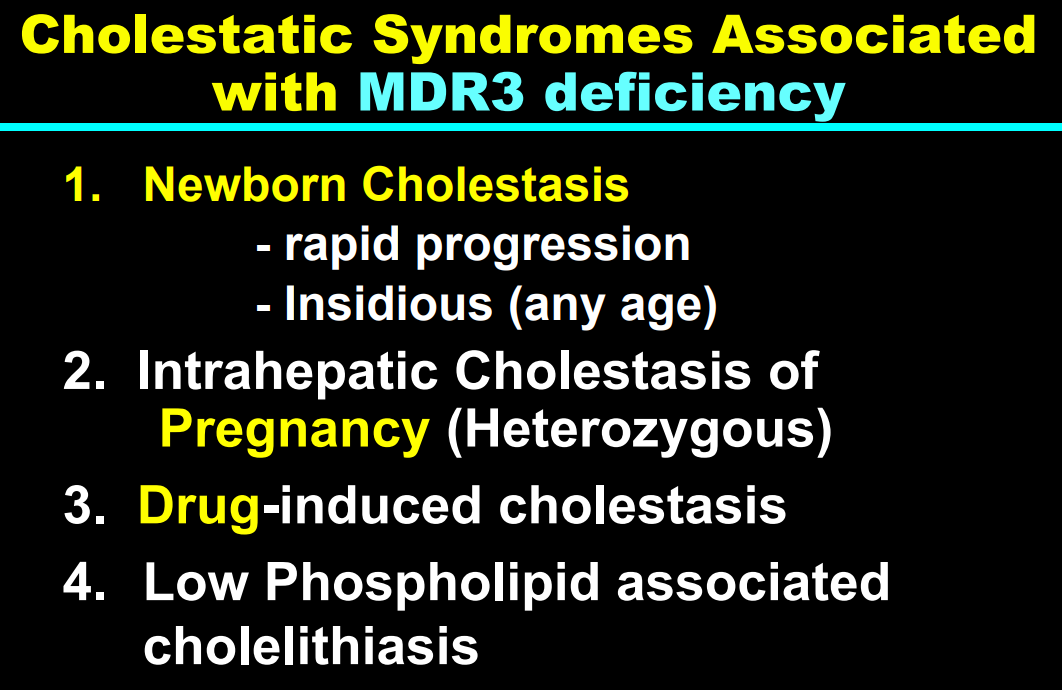
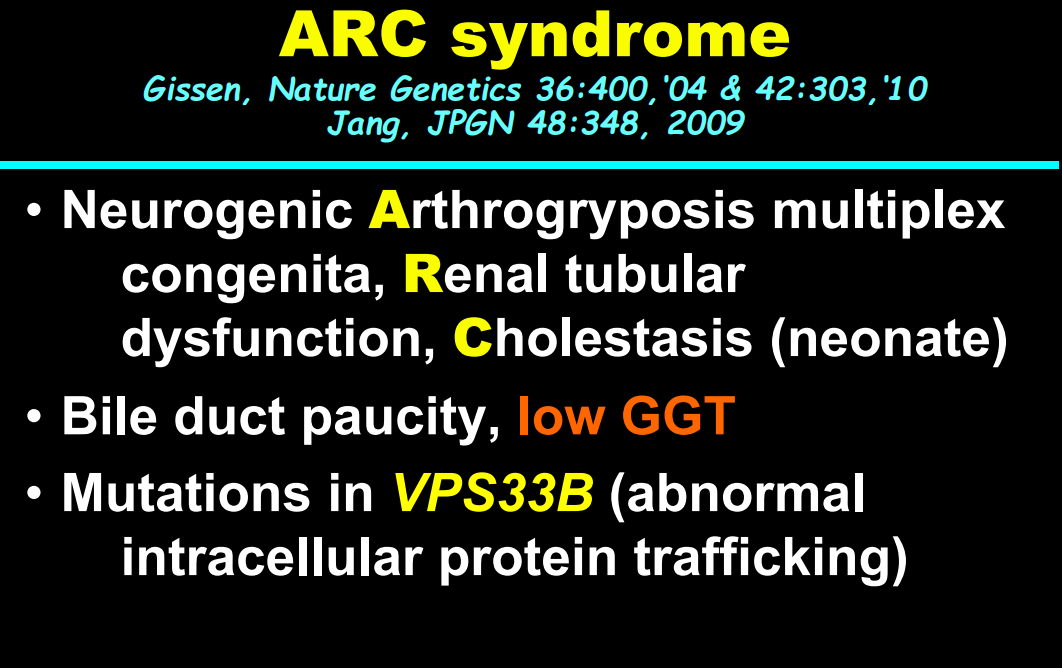
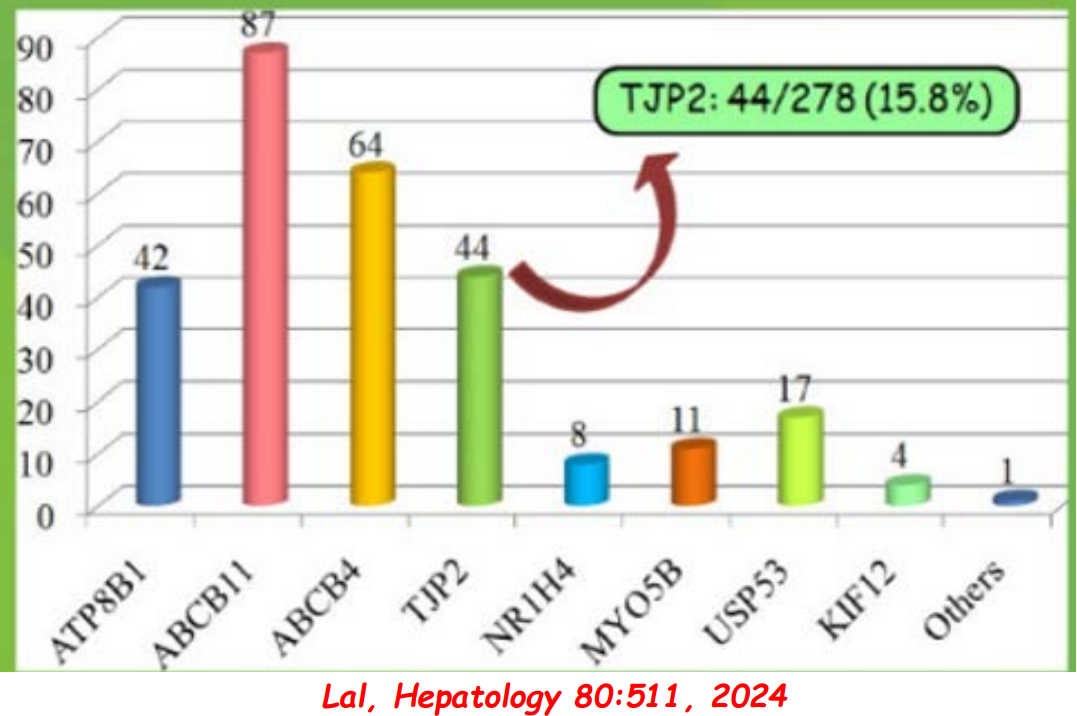
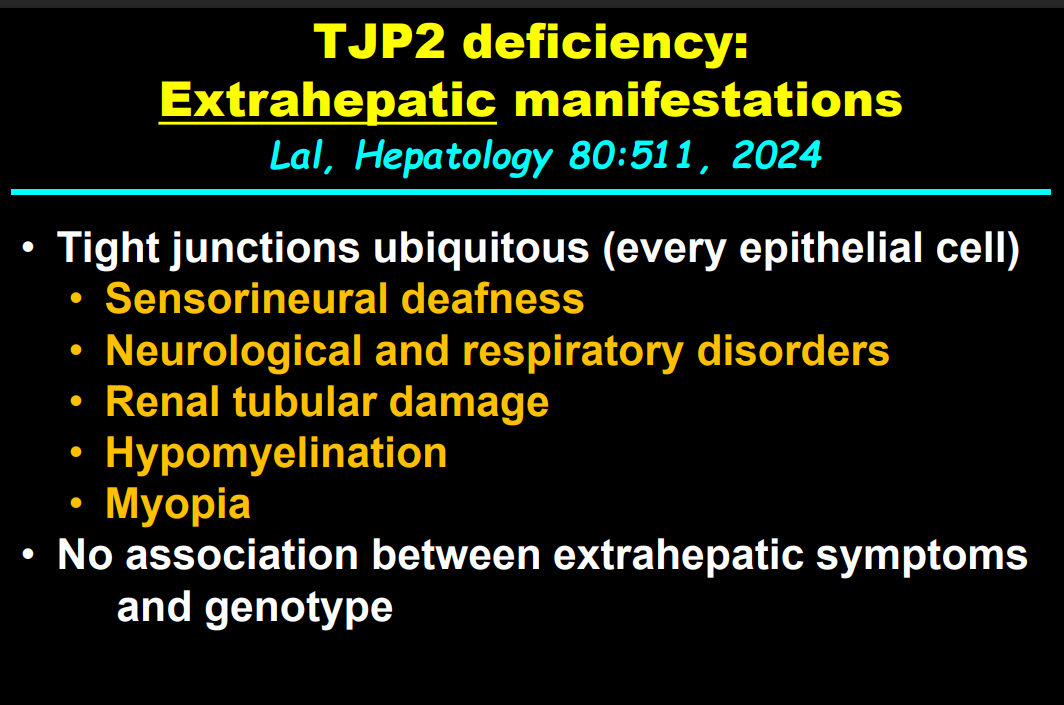
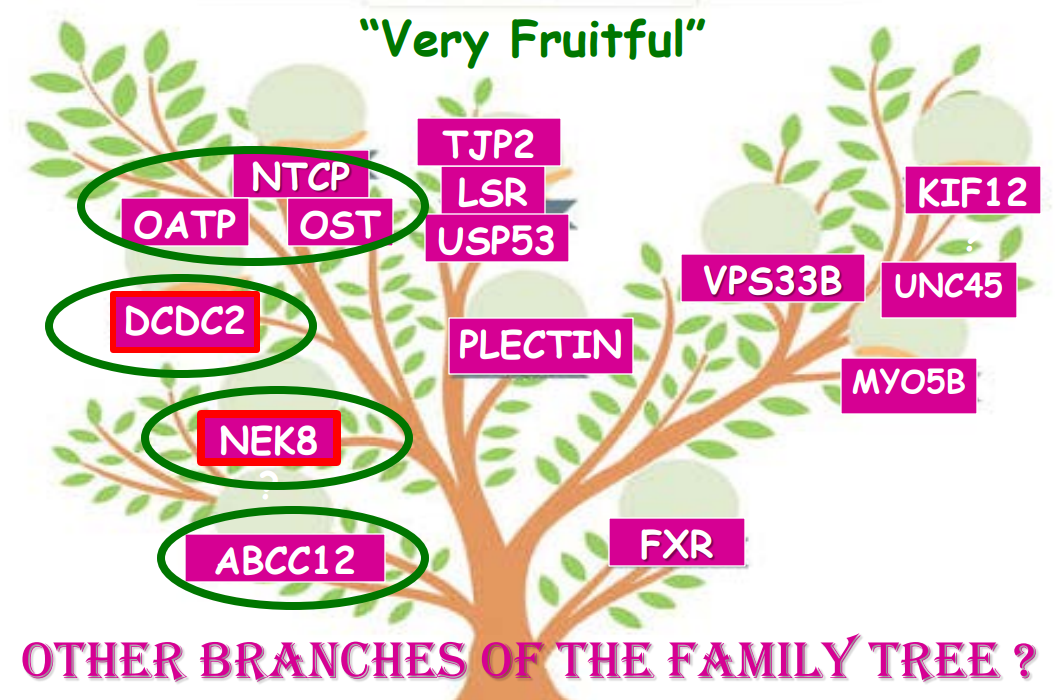
In addition to defects in the metabolic pathway of bile acids, discoveries identified defects in the membrane transporters (eg. FIC1, BSEP, MDR3), trafficking proteins (eg. MYO5B, VPS33B), nuclear control receptors (eg. FXR), and tight junction proteins (eg. TJP2). Tight junction protein defects are associated with bile leakage from bile canaliculus
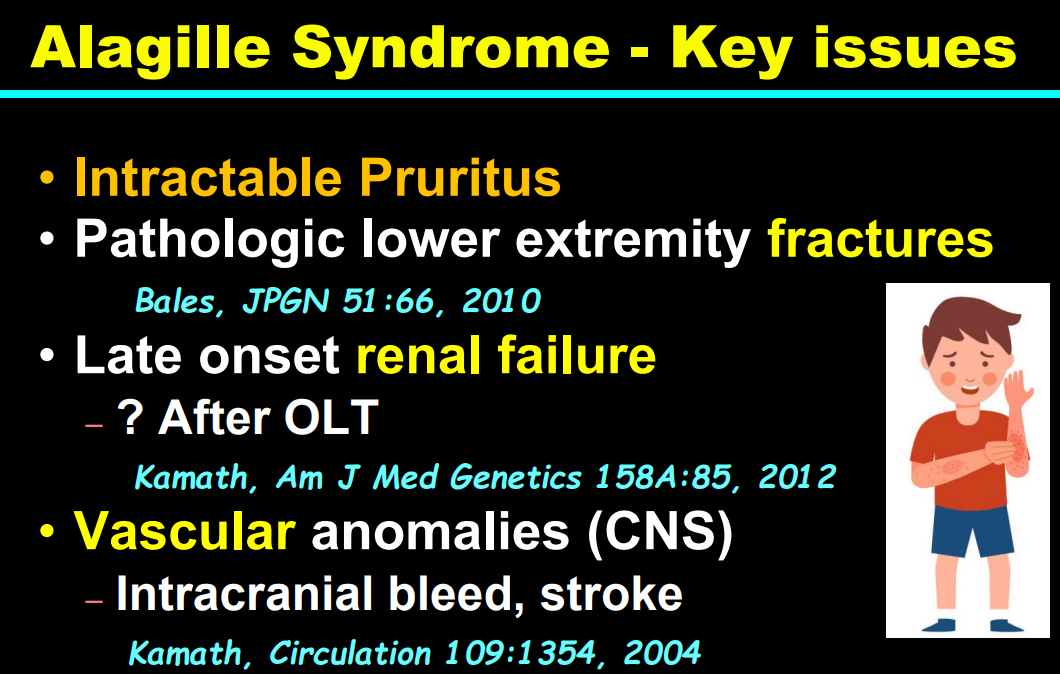
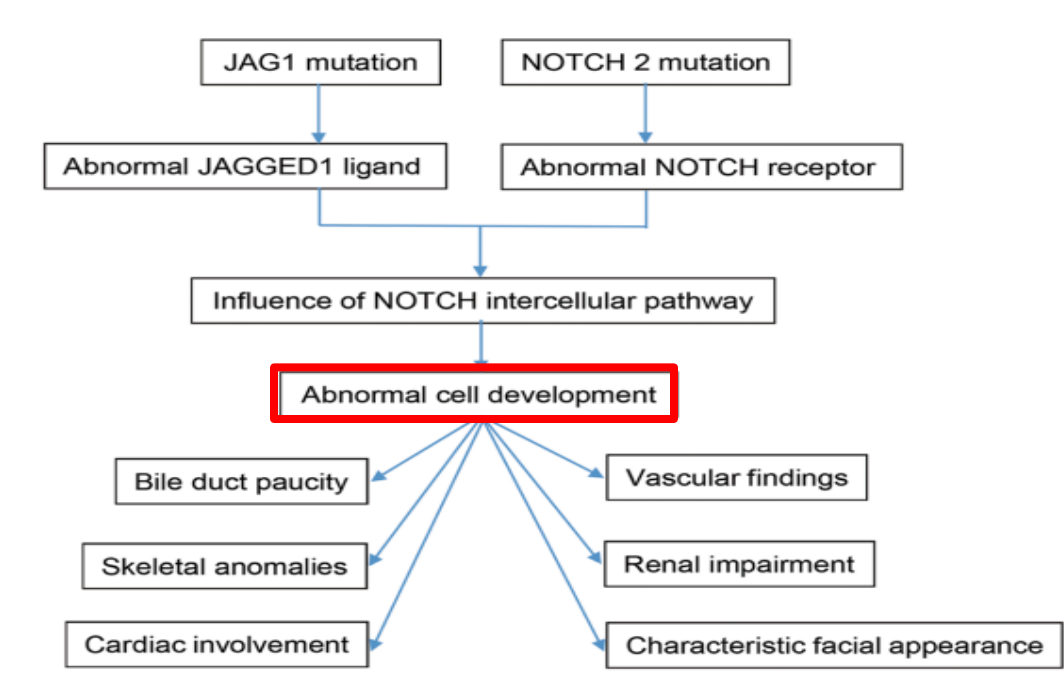
Alagille syndrome, a disorder of embryogenesis, related to JAG1-NOTCH2 signaling pathways affects organs throughout the body
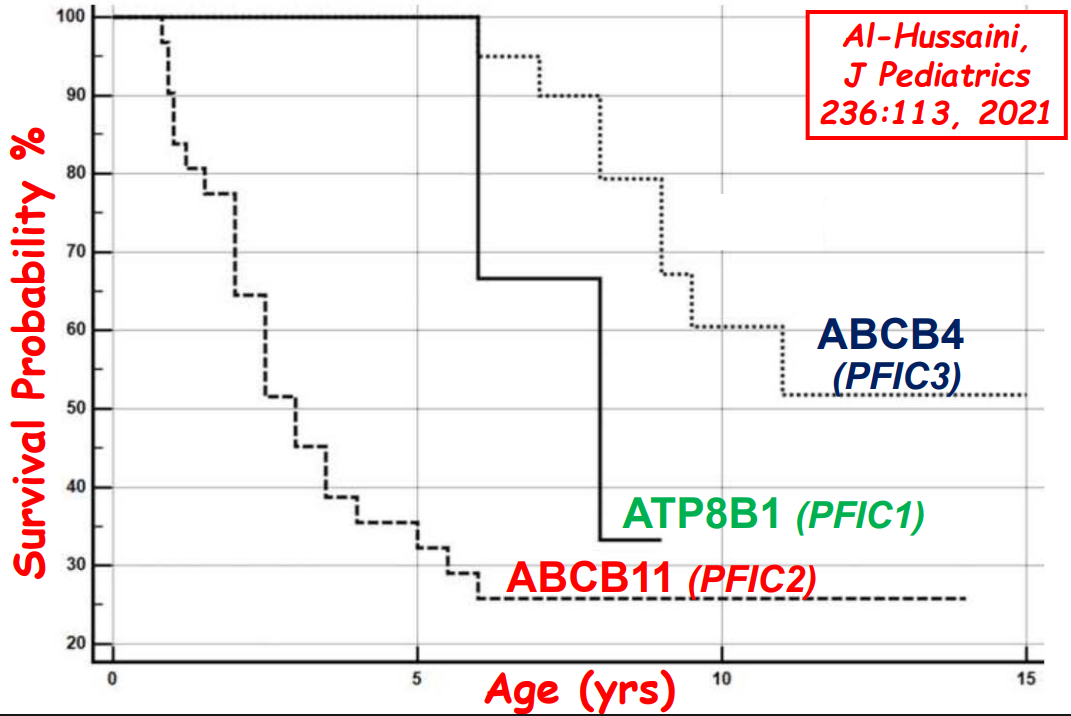
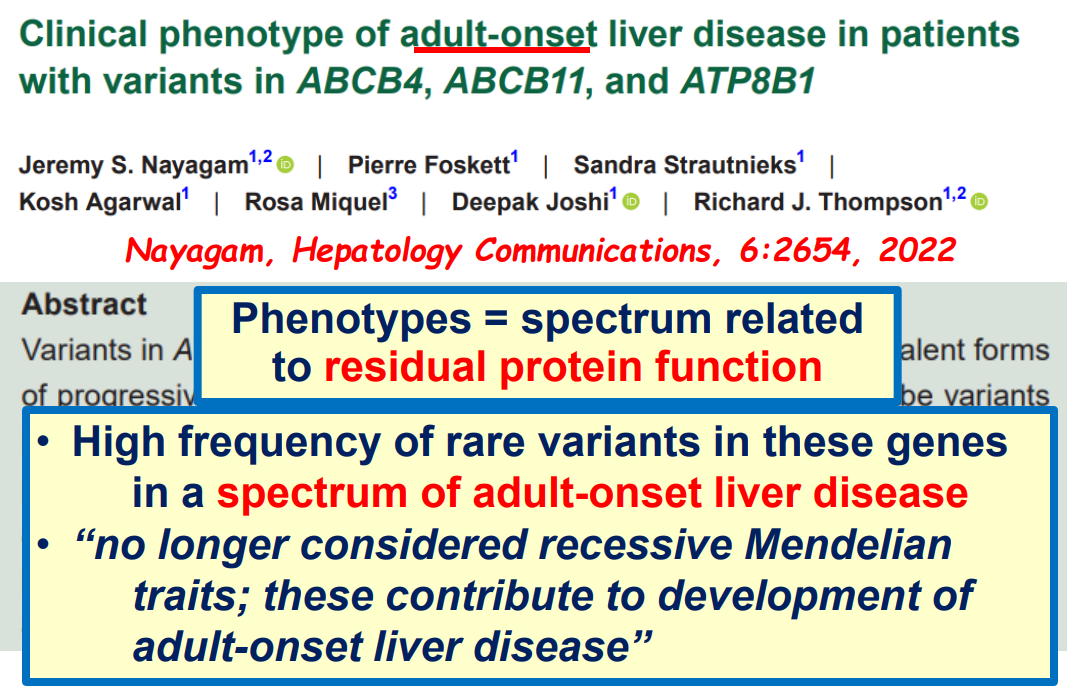
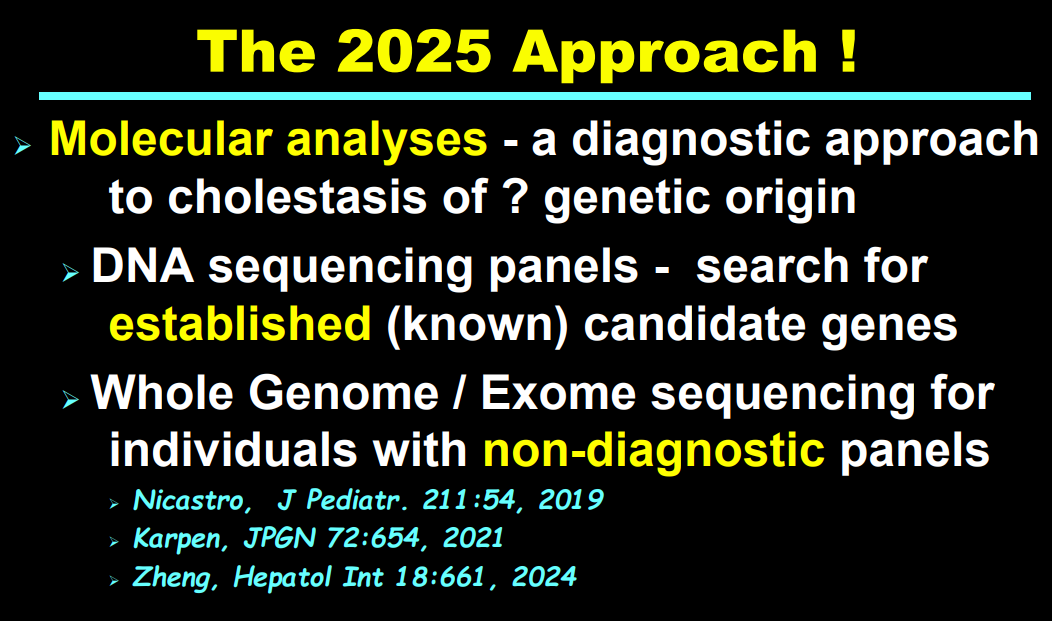
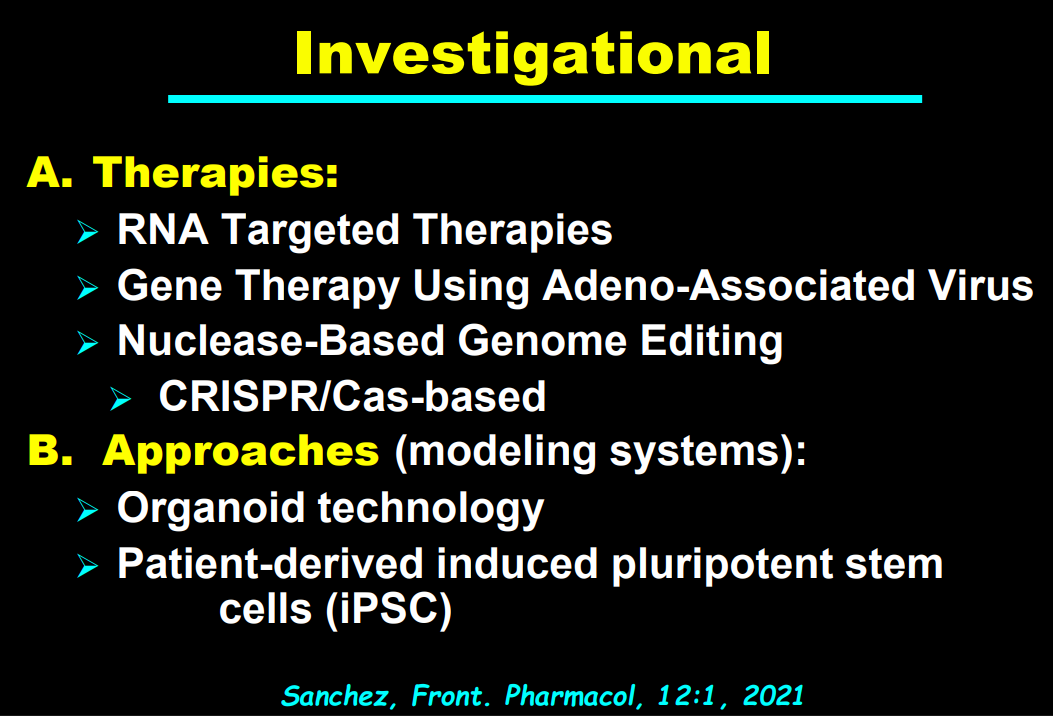
Many of these genetic mutations are now being identified in adults with unexplained liver diseases (eg. intrahepatic cholestasis of pregnancy and cryptogenic cirrhosis)
Cholestasis panels and whole exome sequencing are important tools
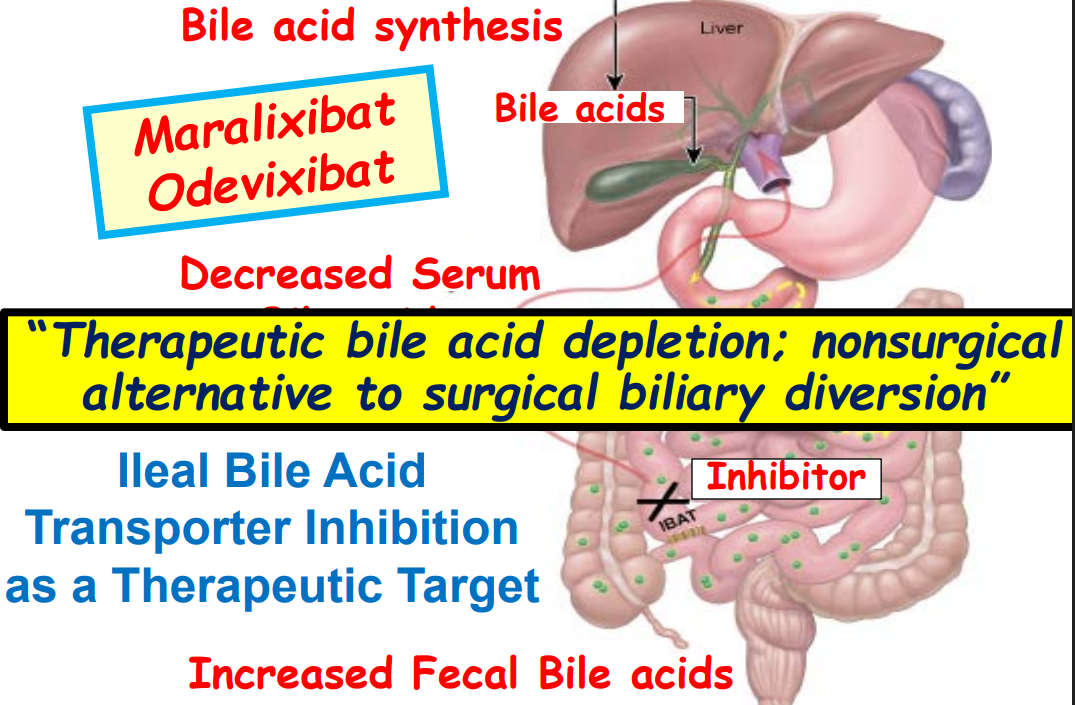
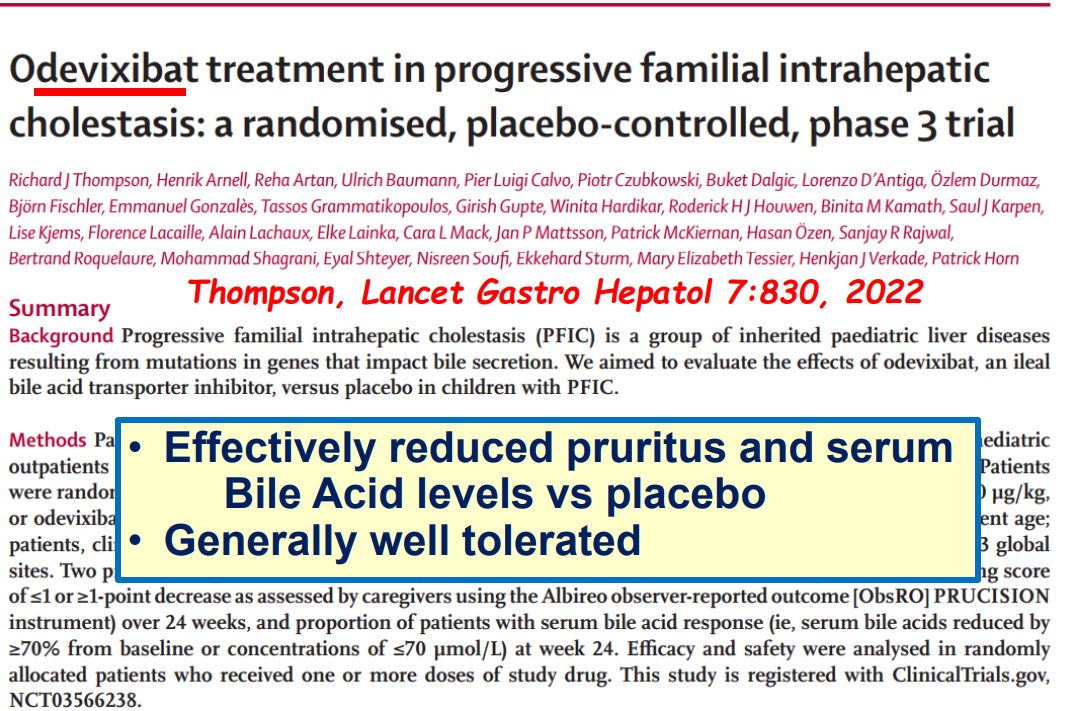
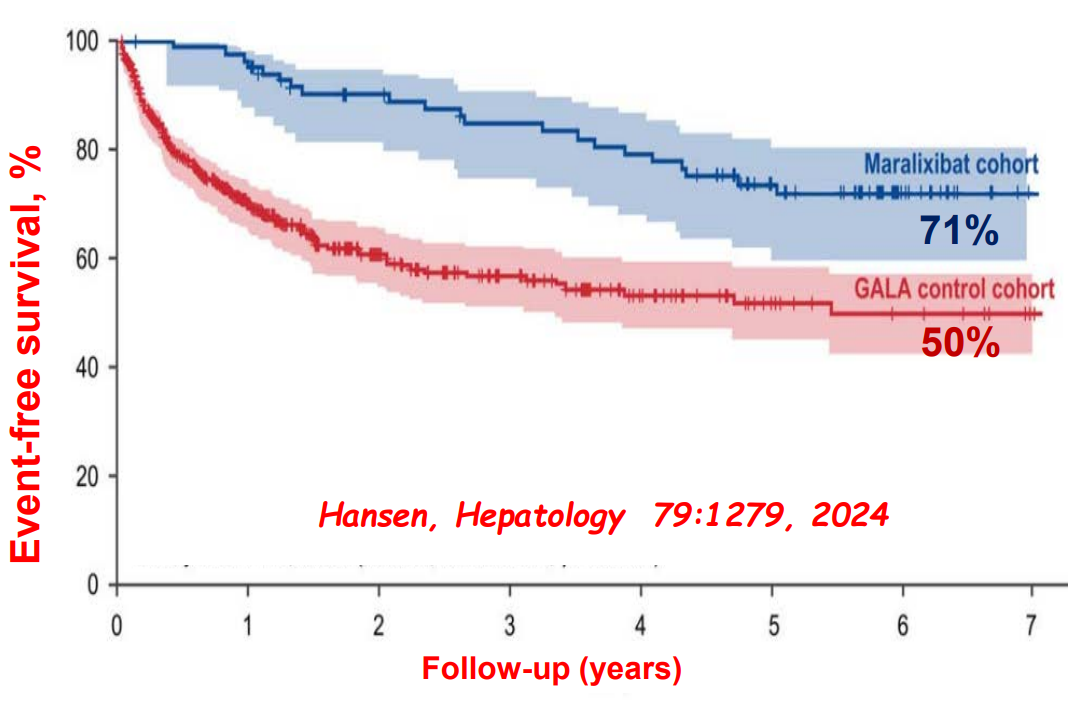
Ileal bile acid transporter (IBAT) inhibitors have emerged as important therapies for conditions like Alagille which were previously treated with biliary diversion
My take: This lecture really shows how the field of pediatric liver disease has been a puzzle. Now one can see how almost all of the pieces of the puzzle work together.
Recently Dr. Balistreri gave our group an excellent lecture. I have taken some notes and shared some slides. There may be inadvertent omissions and mistakes in my notes.
In my view, Dr.Balistreri’s contributions to our field of pediatric gastroenterology, hepatology and nutrition are unsurpassed by any other individual. This is due to his leadership roles (division director, president of AASLD and NASPGHAN), his editor roles (Journal of Pediatrics, and JPGN), his extensive publications/research including sentinel discoveries in bile acid pathophysiology and treatment, and through education (lectures and mentorship).
Key points:
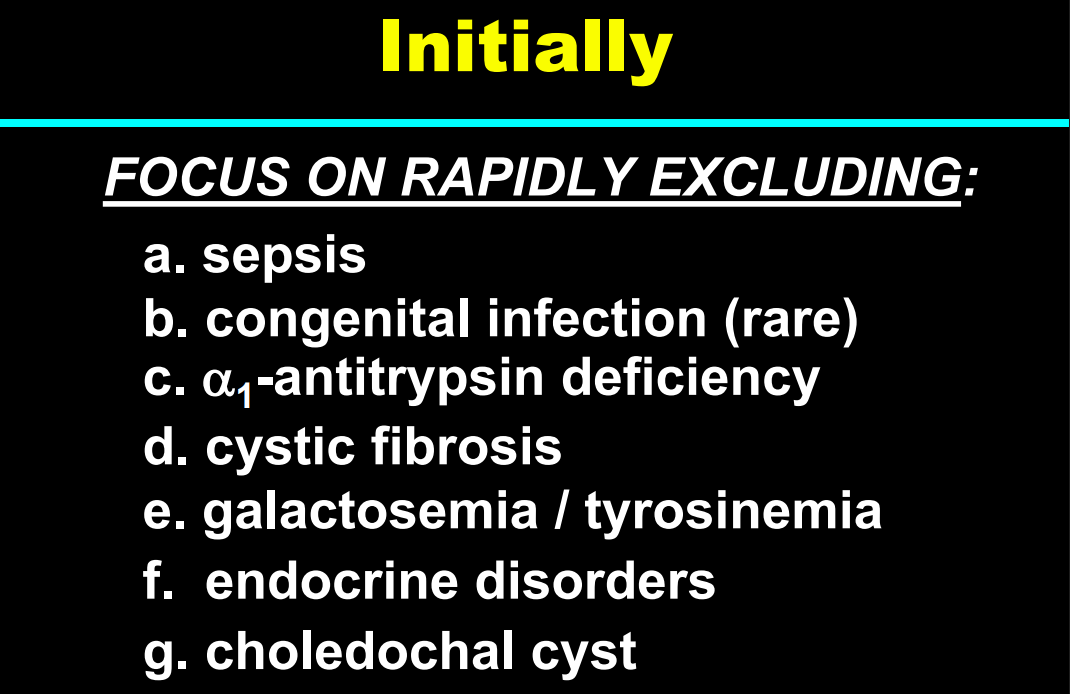
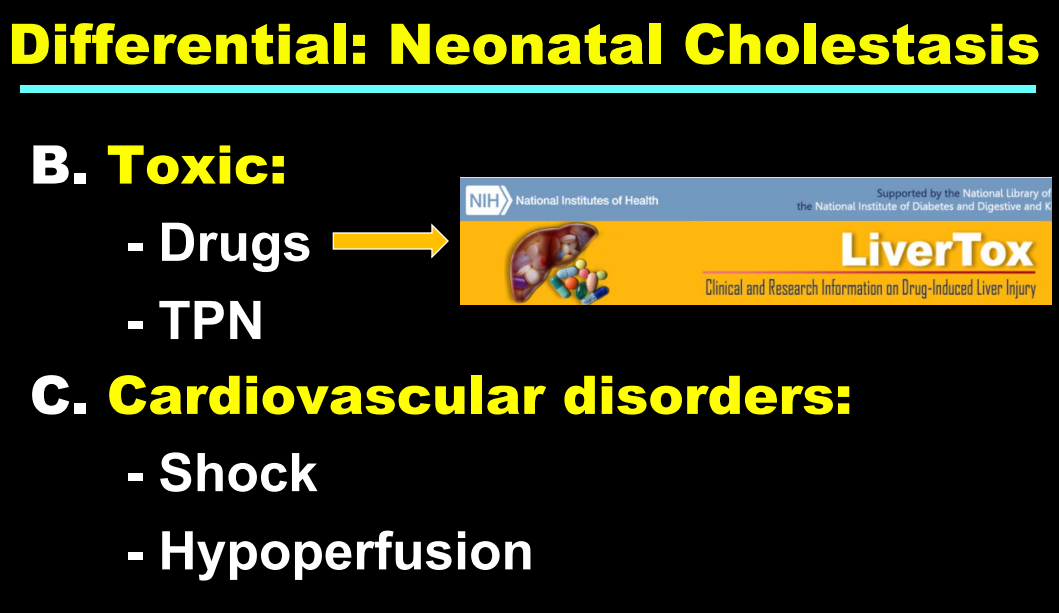
Fifty years ago, ~65% of neonatal cholestasis cases were poorly understood and lumped together under the heading of “Idiopathic Neonatal Hepatitis” (INH). The discovery of Alpha-One Antitrypsin (A1AT) Deficiency was instrumental, indicating that there were specific medical diseases mislabeled as INH
A1AT deficiency proved that many cases were NOT “idiopathic,” NOT necessarily “neonatal,” and NOT “hepatitis”
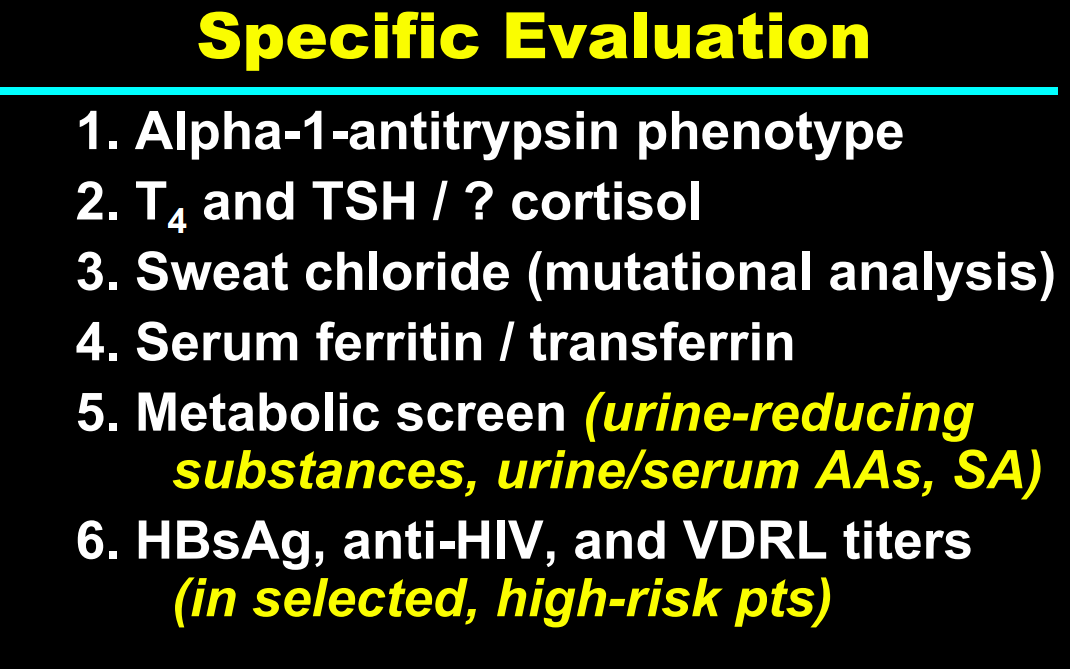
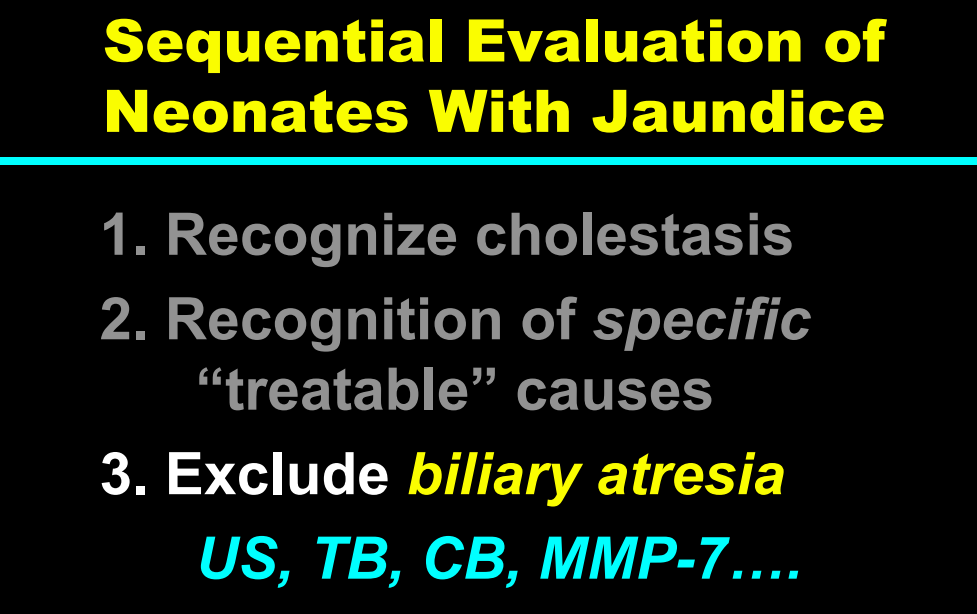
Currently, less than 10% of infants with neonatal cholestasis are unspecified. Dr. Balistreri’s goal has been to make sure every patient receives a precise diagnosis
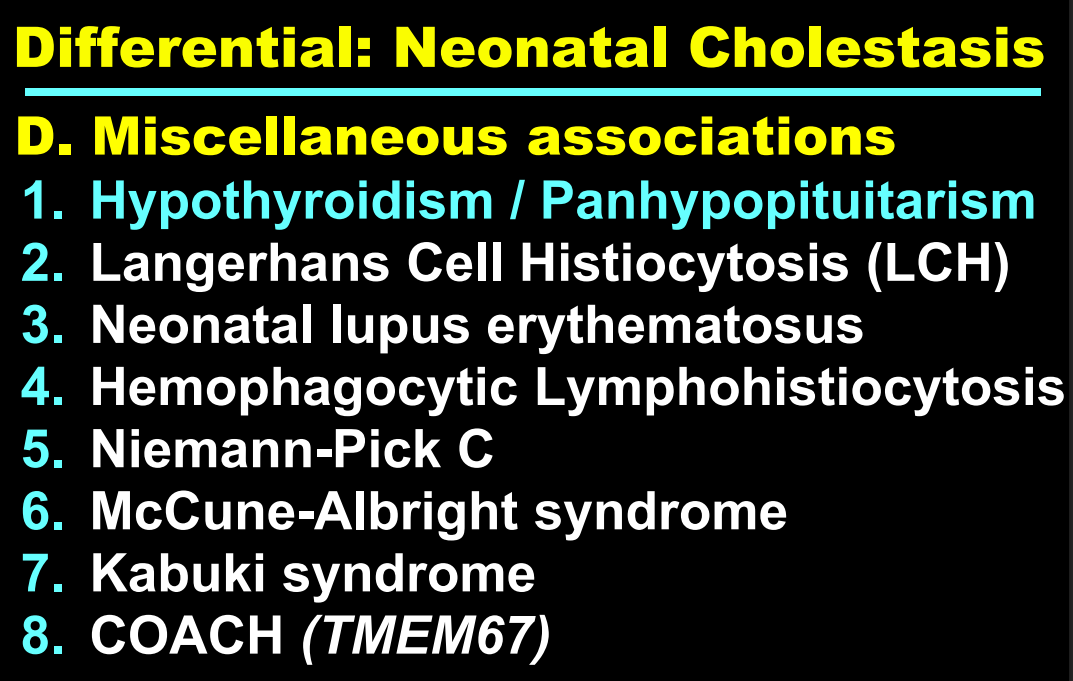
Now more than 90 genetic conditions have been recognized as causing neonatal cholestasis
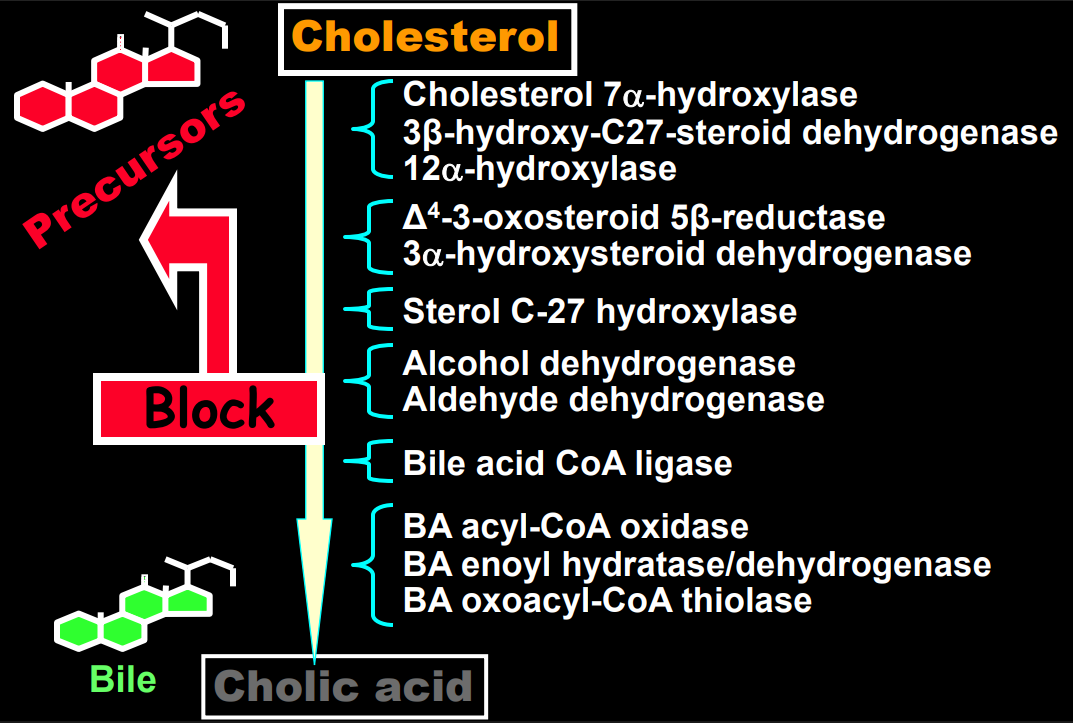
The journey of unraveling the reasons for neonatal cholestasis includes the referral of two infants from Atlanta by Dr. Saripkin to Cincinnati. These infants who had an older sibling who had died at 4 months of age were determined to have an inborn error of bile acid metabolism. Subsequently, they were treated successfully with cholic acid which suppressed production of toxic precursors via feedback inhibition
There are 11 steps in the conversion of cholesterol to bile acids; thus, it was hypothesized and later proven that there would be many other inborn errors of bile acid metabolism
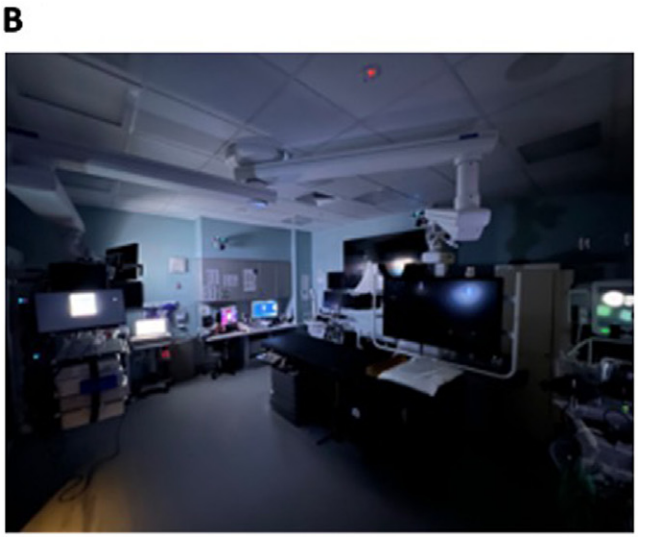
Background: “Unlike diagnostic radiology, GI endoscopy requires the concerted efforts of a proceduralist, anesthesiologist, nurse, and technician. Moreover, several of these individuals are often performing tasks that do not involve looking at a monitor. The advent of laparoscopic surgery presented surgeons with similar lighting challenges. In response to this problem, some operating rooms have been equipped with green lights to achieve high contrast and low glare on monitors while still allowing for the safe and efficient practice of other tasks in the operating room. The choice of green light is based on the fact that the human eye is most sensitive to light with a wavelength around 555 nm, in the green portion of the visible spectrum. This wavelength provides optimal contrast and sharpness under low-light conditions.”
Methods: The authors “conducted a single-center cross-over study comparing image classification on video monitors and the performance of multiple nonmonitored based physical tasks in the endoscopy suite using green light and dim light.”
Key findings:
Performance of physical tasks was significantly faster with green light, including endoscopy setup (43.1 vs. 62.1 s), biopsy sample time (35.8 s vs. 80.1 s), and feeding wire (34.3 vs. 99.1 s)
There was no difference in polyp detection rate under the 2 light conditions. However, color detection of anesthesia medication tapes and endoscopic tools was better with dim light.
Eye strain score was significantly better with green light compared with dim light (10.3 vs. 4.1)
My take: Use of green light in endoscopy suites is likely beneficial particularly in more technically-demanding procedures. It makes common tasks easier/quicker and with less eye strain.
(A) Endoscopy suite under green light. (B) Endoscopy suite under low light.
Congress passing the controversial One Big Beautiful Bill Act could leave millions without insurance and lead to at least 16,000 annual preventable deaths, according to research published in Annals of Internal Medicine…
Arthur L. Caplan, PhD, a professor and founding head of the division of medical ethics at NYU Grossman School of Medicine, told Healio that the authors’ “warnings about what will happen should the Big Beautiful Bill go through have to be taken very seriously.”
“I think the fallout in terms of impact on Medicaid populations … people losing coverage who would then lose access [to health care] is morally staggering and unacceptable,” he said. “We are taking some of the most vulnerable people in society … and cutting back what is often somewhat meager benefits to begin with…”
A brief recently published by the Robert Wood Johnson Foundation also examined the potential impact of Medicaid cuts. Researchers revealed that, if the bill passes, national health care spending would drop by $797 billion over the next 10 years… They found that physicians would see an $81 billion cut, but hospitals would see the biggest decline in spending, at $321 billion.
Enactment of the House bill advanced in May would increase the number of uninsured persons by 7.6 million and the number of deaths by 16 642 annually, according to a mid-range estimate…These estimates may be conservative. They rely on CBO’s assumption that states would replace half of the federal funding shortfall…Medicaid cuts would likely also increase uncompensated care, stressing hospitals and safety-net clinics and causing spillover effects on other patients…
ACA boosted enrollment to more than 90 million. Today, despite its many shortcomings, Medicaid enjoys wide support from the electorate and serves as the foundation of the nation’s health care safety net. The cuts under consideration, intended to offset the cost of tax cuts that would predominantly benefit wealthier Americans, would strip care from millions and likely lead to thousands of medically preventable deaths.
My take: Yogi Berra is attributed with the saying, “It’s tough to make predictions, especially about the future.” While this is true, it is highly likely that huge cuts in Medicaid funding will result in huge numbers who lose health insurance with subsequent increases in mortality and other adverse outcomes.
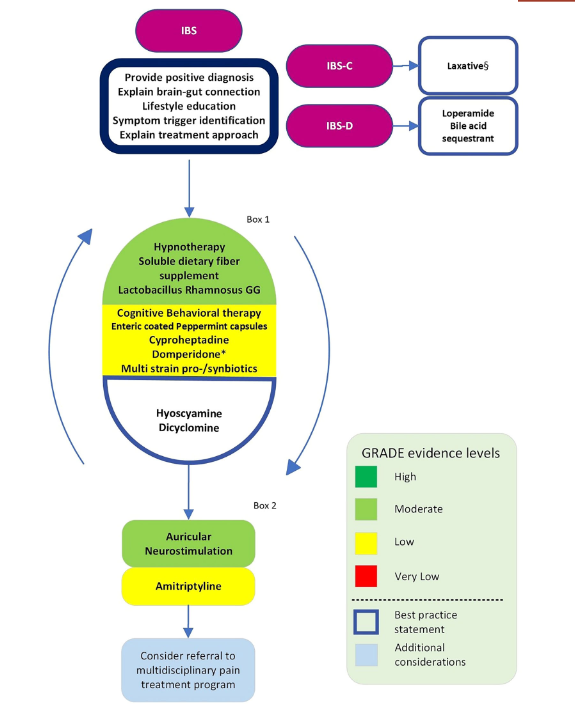
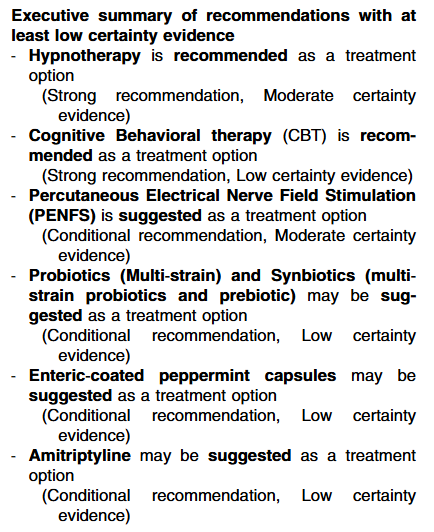
Overall, this article notes that the evidence based for most treatments for pediatric irritable bowel (IBS) is often lacking.
Specific recommendations:
Executive summary of Best Practice Statements‐ The Guideline Development Group (GDG) notes that a crucial emphasis should be placed on education regarding the abdominal pain‐related disorders of gut–brain interaction.
My take: This is a helpful guideline and likely to influence practice.