From Nationwide Children’s and ImproveCareNow: Managing Life with IBD This 2 minute video, geared to patients and kids, discusses ways of managing stress, 504 plans, and potential help from therapists.
Another two videos:

From Nationwide Children’s and ImproveCareNow: Managing Life with IBD This 2 minute video, geared to patients and kids, discusses ways of managing stress, 504 plans, and potential help from therapists.
Another two videos:
An interesting retrospective study (S Wang et al. JPGN 2018; 66: 876-81) looks at a total of 218 endoscopies in 164 children and examines findings in relation to gastrointestinal symptoms. The results focus mainly on upper endoscopy as there were only 20 who had isolated colonoscopy.
Key findings.
An important point in the discussion. The authors take an exception to the idea that normal findings are reassuring. “When procedures are performed despite the expectation of normality this has not been shown to lead to better clinical outcomes of patients…abdominal pain was unaffected by whether or not the patient had undergone endoscopy>”
My take: I agree with the authors that the histologic findings are more likely significant than macroscopic findings in the majority of patients. However, it is worth noting that mild histologic findings are of dubious importance in many cases. Ultimately, identifying strategies to maximize diagnostic yield is needed to provide more cost-effective care and minimize the risks of unnecessary procedures.



A recent study (BD Reed et al. J Pediatr 2018; 197: 97-103) showed that prenatal antibiotic exposure was associated with lower rates of necrotizing enterocolitis (NEC) or death.
In this secondary analysis of a progressive study with 580 infants (<32 weeks) that were cared for in Level III neonatal intensive care units, the authors examined the outcomes of the neonates in relation to whether their mothers had prenatal antibiotics within 72 hours of delivery.
Key findings:
The authors indicate that their initial hypothesis was that maternal antimicrobials (w/in 72 hours of birth) would increase the risk of NEC but in fact provided a 3-fold protection and reduced the risk of death. The effects presumably would be mediated by changes in the infant microbiome related to infant’s exposure to microbial environment at birth and/or transplacental passage of antibiotics. The authors note that their study did not consider mothers to be in the exposure to antibiotics group if their only exposure was antibiotics at the time of cesarean section due to limited time to effect neonate. They did review this group and noted that if they were included in the exposure group that it would not have significantly changed the findings.
My take: This intriguing finding that NEC and death occurred less often in infant’s whose mothers received antibiotics prior to delivery needs further study as does the long-term effect.

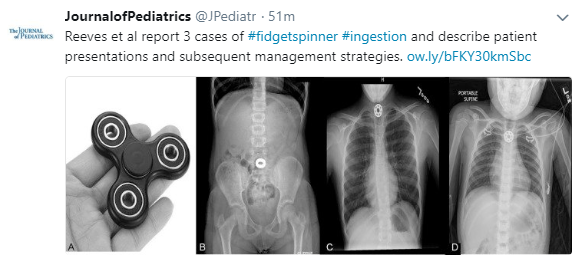
A recent study (PT Reeves et al. J Pediatr 2018; 197: 275-9) reviews 3 new cases of fidget spinner ingestion; there had already been 13 cases reported to Consumer Product Safety Risk Management System since 2016.
Key points:
Related blog posts:
Two studies show that increased digital media exposure (DME) is inversely related to a child’s well-being.
In the first study (S Ruest et al. J Pediatr 2018; 197: 268-74), the authors analyzed more than 64,000 U.S. children (2011-2012). ages 6-17 years. Only 31% reported <2 hours per day of DME. 2-4 hrs/day of DME was noted in 36%, 4-6 hrs/day in 17%, and >6 hrs in 17%. There was an inverse relationship between DME and 5 markers of well-being: completing homework, caring about academics, finishing tasks, staying calm when challenged, and showing interest in learning.
In the second study (P-Y Pin et al. J Pediatr 2018; 197: 262-7), the authors conducted a 1 year prospective trial with 1861 adolescents. They found that 23% had internet addiction at baseline, with internet addiction based on the Chen Internet Addiction Scale. 59 students (3.9%) developed new self-harm/suicidal behaviors. Internet addiction risk conferred a 2.41 relative risk of emerging self-harm/suicidal behaviors.
My take: These studies document a strong association between digital media exposure/internet addiction and worrisome behaviors/worsened well-being.

Pine Mountain Trail


“You should never assume. You know what happens when you assume. You make an ass out of you and me because that’s how it’s spelled.”
–Attributed to multiple individuals (but I heard this first when I watched Bad News Bears as a kid)
The increasing frequency of many conditions like inflammatory bowel disease cannot be explained by our genetics. The search for environmental triggers are ongoing. Broadly, the main suspects are dietary, antimicrobials, and pollutants. (Related blog post: Nutrition Week (Day 7) Connecting Epidemiology and Diet in Inflammatory Bowel Disease)
The latest concern is now Splenda:
“The Artificial Sweetener Splenda Promotes Gut Proteobacteria, Dysbiosis, and Myeloperoxidasse Reactivity in Crohn’s Disease-Like Ileitis” A Rodriguez-Palacios et al. Inflamm Bowel Dis 2018; 24: 1005-20. Editorial 1055-6 by B Chassaing and AT Gewirtz.
This highly technical study involved research in ileitis-prone SAMP mice and includes a huge amount of data and cool figures.
The authors note in their discussion: “The term ‘Western diets’ implies a proven shift of the microbiota that enhances the susceptibility to adherent-invasive E coli infections and intestinal inflammation in mice. In this study, we report similar findings due solely to the administration of a minor component of the diet.”
Some of the key points in the editorial:
My take: I think the influences on the microbiota are difficult to tease out. Thus, this study (in mice) indicates —don’t assume that nonabsorbed agents are harmless

Mystery NY Times Case: Why Did the Young Woman’s Heartburn Keep Getting Worse?
An excerpt:
The radiologist who read the scan made an interesting observation. In each of the three visits to the E.R., the patient’s blood had been tested. All three tests showed an elevated white-blood-cell count. That could suggest an infection — but in her tests a quarter of those white blood cells were a cell type known as eosinophils, which normally make up only a tiny fraction of the white blood cells in the circulation. ..
When the radiologist saw the elevated level of eosinophils, however, he recalled an unusual and relatively new disorder known as eosinophilic gastroenteritis (EGE). He added this rarity to the list of possible causes of the patient’s abnormal CT findings on his report…
EGE is thought to be an unusual type of allergic reaction to foods. Food exposure triggers the recruitment of eosinophils to the gut, but once they have a toehold, repeated exposure isn’t necessary to keep them there. The disorder was first described in a series of patients in the United States in 1993 but since then has been found to occur throughout the developed world. Because it’s a relatively new disease, and because our understanding of allergy is still emerging, it’s not well understood. As recognition of the disorder expands, so, too, do the number of cases. Patients are usually started on an elimination diet and given steroids to further suppress the immune system. An elimination diet — one in which the foods most frequently linked to allergic reactions, like milk, eggs and wheat, are not consumed — has been shown to be helpful up to 90 percent of the time.
Related blog posts:
.
A terrific commentary (Bill Gates, NEJM 2018; 378: 2057-60) explains how we are NOT preparing for the next pandemic and what we should be doing and why.
Key points:
My take (borrowed): “”If it were a military weapon [threat], the response would be to de everything possible to develop countermeasures. In the case of biologic threats, that sense of urgency is lacking. But the world needs to prepare for pandemics in the same serious way.”