PA Ubel et al. NEJM 2025; 392: 729-731. Out of Pocket Getting Out of Hand — Reducing the Financial Toxicity of Rapidly Approved Drugs
Key points:
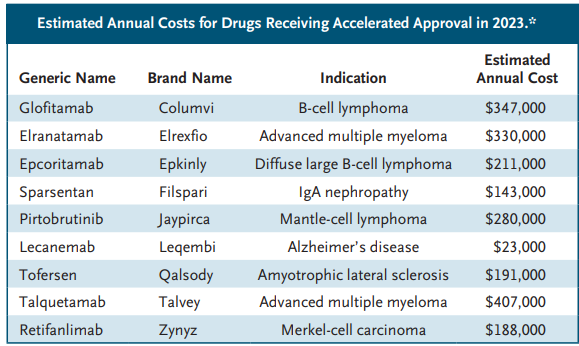
In 2023, the median list price of new drugs was $300,000 per year. The FDA does not consider drug cost as part of its approval process.
Many new drugs have uncertain benefits despite FDA approval. “Since the FDA is authorized to approve drug labeling, it could consistently require that labeling indicate when a drug’s approval was based on results from uncontrolled trials or from trials with surrogate measures…might reduce the chances that patients, seeing that a drug has FDA approval, will mistakenly assume that it has been proven to provide substantial benefits..[however] . In the face of serious illness, people frequently prefer action to inaction, even when they would ultimately be harmed by taking action.”
Optimally, “congress would need to pass legislation giving the agency authority to consider financial harms when making decisions about drugs with unclear benefits, and the FDA would need to gain expertise in evaluating the budgetary implications of new drugs.”
My take: The financial burdens of newer medications leave patients unable to afford other necessary medical and non-medical expenses. This is especially problematic when a new medication offers minimal benefit.
Background: This study aimed to identify biomarkers by conducting a Danish nationwide genome-wide association study (GWAS) on severe vs less severe ulcerative colitis.
Methods: Severe ulcerative colitis: Patients with severe ulcerative colitis were defined as having at least 1 major ulcerative colitis–related operation, at least 2 ulcerative colitis–related hospitalizations exceeding 2 days, and/or use of at least 5000 mg of systemic corticosteroids within 3 years of diagnosis
The authors utilized two source populations
The Center for Molecular Prediction of Inflammatory Bowel Disease (PREDICT) neonatal blood spot cohort (NBS) includes individuals born in Denmark and diagnosed with ulcerative colitis from 1981 to 2022
The North Denmark Biobank study is a population-based cohort of patients from Northern Denmark with inflammatory bowel disease from 1978 to 2020 (NorDIBD)
The combined cohort included 4491 patients (4153 from NBS and 338 from NorDIBD) with a mean (SD) age at diagnosis of 23.3 (8.4) years; 53% of patients were female and 27% had severe disease.
Key findings:
The association with HLA-DRB1*01:03 (Figure 1) had an OR of 6.38 for major operation, OR of 5.24 for at least 2 hospitalizations, and OR of 2.30 for use of at least 5000 mg of systemic corticosteroids in carriers vs noncarriers
Carriage of HLA-DRB1*01:03 allele was 2.8% in these cohorts
Limiation: Danish cohort -may not be applicable to other populations
My take: HLA-DRB1*01:03 is a low-frequency allele, carriers have a significantly higher risk of severe ulcerative colitis.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
E Park. NEJM 2025; DOI: 10.1056/NEJMp2501855. Medicaid on the Chopping Block
An excerpt:
A top priority for Congress and President Donald Trump is extending and expanding tax cuts expiring at the end of 2025…Republican leaders in the House intend to make at least $880 billion in Medicaid cuts over 10 years to offset some of the tax cuts’ $4.5 trillion cost…
Medicaid, however, is more essential than it has ever been. It provides affordable, comprehensive health coverage to more than 72 million low-income Americans1…Medicaid covers about 40% of all children and births in the United States. It covers more than one third of people with disabilities and 44% of children with special health care needs…
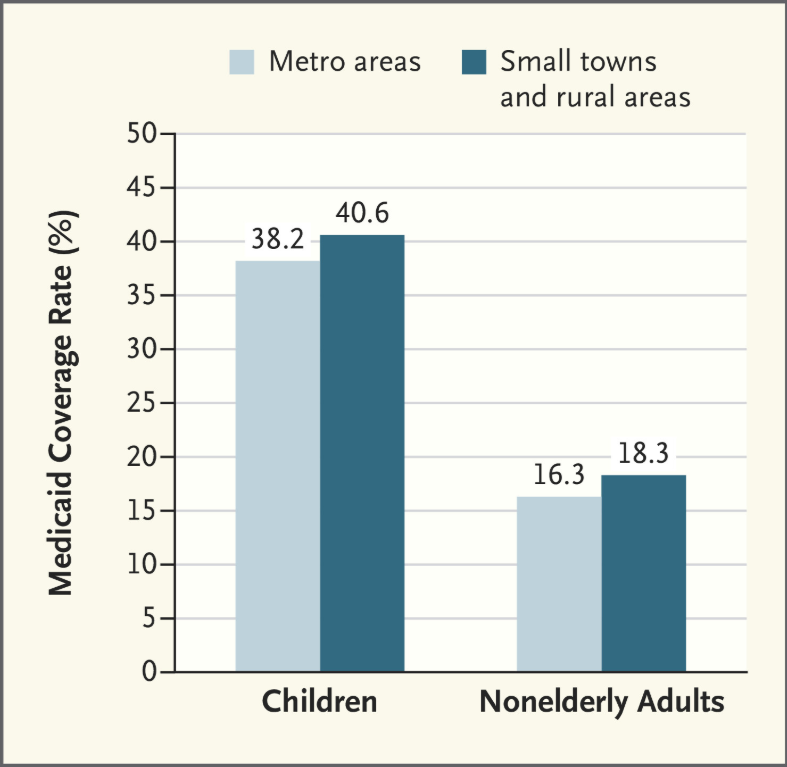
Medicaid is especially vital for rural communities. Residents of small towns and rural areas disproportionately rely on Medicaid…
Under many of these proposals, states would face drastic reductions in federal Medicaid funding….states would have to choose among three painful options. They could dramatically raise income and sales taxes. They could deeply cut other parts of their budgets, such as budgets for K–12 education and higher education, which account for about 43% of states’ own spending. Or — the option most states would have to choose — they could slash their Medicaid programs by substantially narrowing Medicaid eligibility, restricting benefits, making it harder for eligible people to enroll in and renew coverage, and making sharp cuts to already low reimbursement rates for hospitals, physicians, and nursing homes.
As a result, many low-income children, parents, people with disabilities, older adults, and others would be at risk for becoming uninsured and forgoing needed care…As opposition becomes increasingly public, widespread, and vocal, congressional Republican leaders could ultimately view severe Medicaid cuts as too politically difficult and decide they need to drop them from budget reconciliation.
My take: This article elaborates on all the ways that Congress could curtail Medicaid spending. Ultimately, all of them will leave the states with additional costs if they are to maintain current coverage levels. Even with the proposed cuts to Medicaid, the tax cut plan is projected to add two trillion dollars each year during this administration.
Related article: 3/2/25 Patricia Murphy, AJC: Medicaid cuts from Washington would gut this Georgia pediatrician’s practice (behind paywall) “A South Atlanta pediatrician [Dr. Dorsey Norwood] says 85% of her patients are covered by government health care program…For at least one Georgia pediatrician, cutting Medicaid benefits for her young patients would leave a wound in her practice that even she couldn’t heal.”
There is very little that Americans can agree on these days…
But one thing nearly everyone agrees on? Vaccines are good.
This simple fact has been overshadowed by fears about what will happen to vaccine policy under Robert F. Kennedy Jr., the new secretary of health and human services. He has a long history of vaccine skepticism, and critics fear his leadership could lead to interference with vaccine programs or even withdrawal of vaccines from the market. Such moves are already roiling some state health programs. In Louisiana, the Health Department will “no longer promote mass vaccination,” instead leaving vaccine education to medical providers…
Recent reports in the news media and medical journals highlight a decline in the proportion of kindergartners who have received the measles, mumps and rubella shot. In the past five years, national coverage has fallen to 93 percent, from 95 percent, and in some states like Idaho, it is as low as 80 percent. But while these numbers fall short of the national goal of 95 percent required to maintain herd immunity for measles, they remain a resounding show of confidence…
Some 92 percent of American children received the polio vaccine by age 2, and more than 90 percent were vaccinated against hepatitis B. And it’s not just because of school requirements. Nearly nine in 10 Americans — including 86 percent of Republicans — say the benefits of childhood vaccines outweigh the risks...
Emphasizing the popularity of vaccines is not merely a matter of correcting the record. Studies have shown that presenting vaccines as a subject of debate or controversy can unintentionally reinforce vaccine hesitancy by making the issue appear less settled. For instance in one study, researchers found that college students who were asked to read a news report on vaccine safety that presented both sides in a falsely balanced fashion came away with the mistaken impression that the science on vaccine safety was in flux…
Routine vaccinations are just that: routine. Nearly all children receive them, and millions have benefited by being spared painful diseases and death. Leaders who undermine this basic tool may find themselves on the wrong side of both science and voters.
My take: Caitlin Rivers provides a lot of useful advice regarding infectious diseases. She has frequent (~weekly) substack articles with up-to-date information regarding infection prevalence (eg. Flu, COVID, norovirus, etc). Link to substack: Force of Infection
Methods: Using two large administrative databases, MarketScan and Medicare, the authors estimated annual prevalence of EoE, as well as age- and sex-stratified estimates, standardized to the U.S. population. Health care utilization, including medications and endoscopic procedures, was quantified, and annual EoE-associated costs were calculated.
Key findings:
There was a 5-fold increase in prevalence in both databases since 2009.
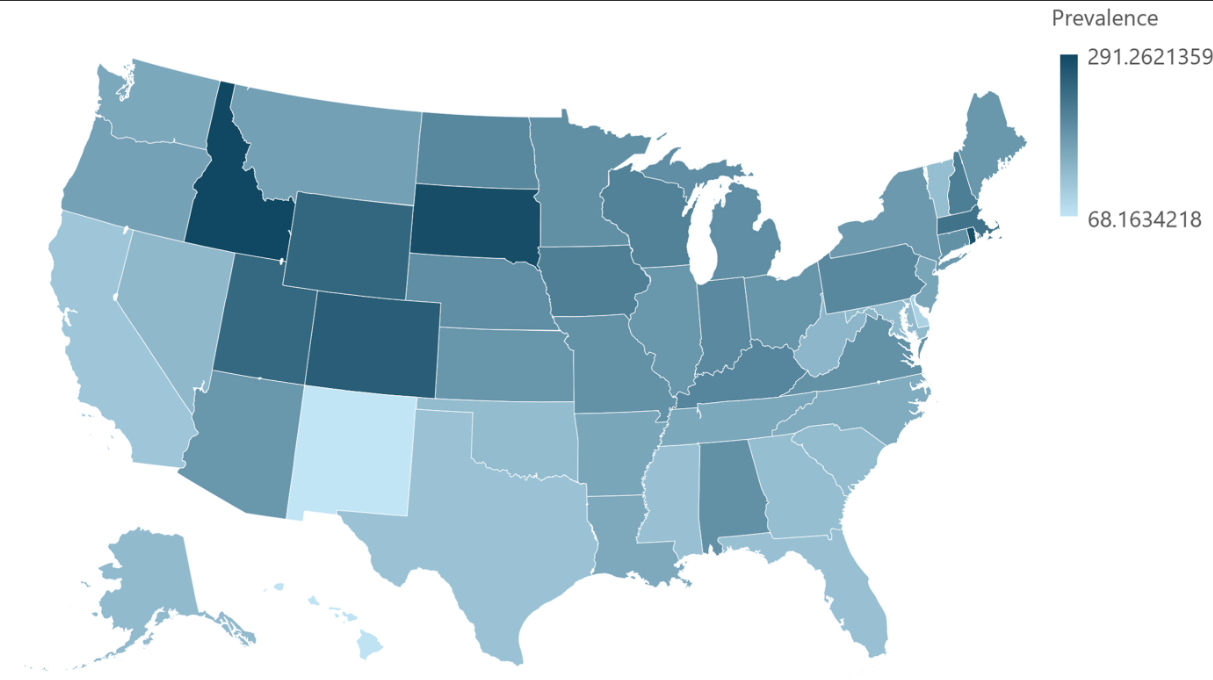
Standardized to the U.S. population, the prevalence of EoE was 142.5/100,000, extrapolating to 472,380 cases. This equates to ~1 in 700 persons.
Total EoE-associated annual health care costs were estimated to be $1.32 billion in 2024 dollars after accounting for inflation.
PPIs were used more commonly than steroids for treatment. For Marketscan in 2022, PPIs were used in 41% and steroids in 26%.
There has been a 5-fold prevalence increase since 2009Prevalence by State. Overall, ~1 in 700 EoE Prevalence in U.S.
My take: There is likely a true increase in the number of affected individuals, though some changes in prevalence are due to an increased recognition/testing of eosinophilic esophagitis.
In the REPREVIO study, a double-blind, randomized, placebo-controlled trial, 80 adults received either vedolizumab (300 mg IV) (n=43) or placebo (n=37) at weeks 0, 8, 16 and 24 following ileocolonic resection and had one or more risk factors for recurrence.
Key findings:
At week 26, the probability of a lower modified Rutgeerts score with vedolizumab versus placebo was 77·8% (95% CI 66·4 to 86·3; p<0·0001).
Severe endoscopic recurrence was observed in ten (23·3%) of 43 patients in the vedolizumab group versus 23 (62·2%) of 37 patients in the placebo group (difference –38·9% [95% CI –56·0 to –17·3]; p=0·0004).
Adverse effects were noted in three patients who received vedolizumab (bilateral tubo-ovarian abscesses, thrombosed hemorrhoids, and pancreatic adenocarcinoma) and two patients who received placebo (intestinal perforation related to Crohn’s disease and severe abdominal pain)
My take: This study shows that vedolizumab is another biologic capable of reducing postoperative recurrence following ileocolonic resection in Crohn’s disease. Infliximab has been shown to reduce recurrence as well (shown in the PREVENT study).
In this sample of 113 pediatric patients with IBD, 77% of initial denials for biologic therapy were ultimately approved.
The median time to receiving medication was 18 days, with administrative time (prior authorization and appeal) requiring a median of 180 min.
More than half (60%) of patients experienced adverse outcomes or worsened quality of life due to delays in treatment.
My take (borrowed in part from authors): “Barriers to treatment by payors, of which 77% are ultimately approved, result in substantive treatment delay, patient harm, and hospitalization.” While 18 days (or more) may not seem like a lot, it is when you know the right therapy at the outset and delays lead to suffering and worsened outcomes. In addition, the insurance companies and PBMs (pharmacy benefit managers) know that exhausting valuable physician/office staff time is a disincentive. It makes physicians determine whether it is worth the fight.
The sickest patients are supposed to get priority for lifesaving transplants. But more and more, they are being skipped over…For decades, fairness has been the guiding principle of the American organ transplant system…today, officials regularly ignore the rankings, leapfrogging over hundreds or even thousands of people when they give out kidneys, livers, lungs and hearts…
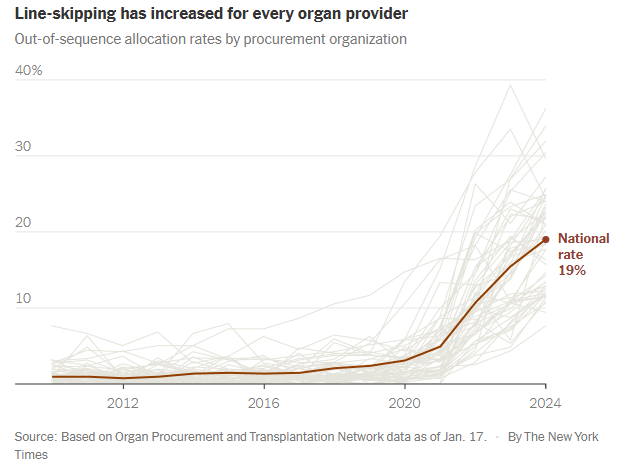
Last year, officials skipped patients on the waiting lists for nearly 20 percent of transplants from deceased donors, six times as often as a few years earlier. It is a profound shift in the transplant system, whose promise of equality has become increasingly warped by expediency and favoritism…
Under government pressure to place more organs, the nonprofit organizations that manage donations are routinely prioritizing ease over fairness. They use shortcuts to steer organs to selected hospitals, which jockey to get better access than their competitors.
These hospitals have extraordinary freedom to decide which of their patients receive transplants, regardless of where they rank on the waiting lists. Some have quietly created separate “hot lists” of preferred candidates...
More than 100,000 people are waiting for an organ in the United States, and their fates rest largely on nonprofits called organ procurement organizations…
The procurement organization is supposed to offer the organ to the doctor for the first patient on the list. But the algorithms can’t necessarily identify exact matches, only possible ones. So doctors often say no, citing reasons like the donor’s age or the size of the organ…
Until recently, organizations nearly always followed the list. On the rare occasion when they went out of order and gave the organ to someone else, the decision was examined by the United Network for Organ Sharing — the federal contractor that oversees the transplant system — and a peer review committee. Ignoring the list was allowed only as a last resort to avoid wasting an organ...
Procurement organizations regularly ignore waiting lists even when distributing higher-quality organs. Last year, 37 percent of the kidneys allocated outside the normal process were scored as above-average…
Skipping patients is exacerbating disparities in health care. When lists are ignored, transplants disproportionately go to white and Asian patients and college graduates…
How a rare shortcut became routine
In 2020, procurement organizations felt under attack. Congress was criticizing them for letting too many organs go to waste. Regulators moved to give each organization a grade and, starting in 2026, fire the lowest performers... the organizations increasingly used a shortcut known as an open offer. Open offers are remarkably efficient — officials choose a hospital and allow it to put the organ into any patient...
Open offers are a boon for favored hospitals, increasing transplants and revenues and shortening waiting times. When hospitals get open offers, they often give organs to patients who are healthier than others needing transplants…Healthier patients are likelier to help transplant centers perform well on one of their most important benchmarks: the percentage of patients who survive a year after surgery...
It is impossible to gauge whether line-skipping prevents wasted organs. But data suggests it does not. As use of the practice has soared, the rate of organs being discarded is also increasing.
My take: This article was eye-opening for me as I am not actively involved in listing patients for transplantation. I was unaware of this increasing tendency of line-skipping and open source allocation. It is disturbing to see the distribution process undermined in this manner –better oversight is needed to assure fairness for those whose lives are at stake.
M Cananzi et al. J Pediatr Gastroenterol Nutr. 2025;80:260–270. Current practice in the management of paediatric autoimmune liver disease in Europe
Methods: Thirty-six centers from 22 European countries responded to the survey that was sent to European Reference Network for Rare Liver Disorders (ERN RARE-LIVER) and members of the Hepatology Interest Group (HIG) of the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN)
Key findings:
All centers use predniso(lo)ne as first-line therapy, alone (15/36) or with azathioprine (21/36)
Azathioprine and mycophenolate are the preferred second-line options in centres using first-line steroid monotherapy (11/15) or combined steroid-azathioprine (19/21)
Tacrolimus is used as third-line agent in 15/36 centers
Proactive measurement of drug metabolites and target levels vary widely among centers. About 27/36 centers have thiopurine methyltransferase (TPMT) genotyping available, of which 21 (58%) routinely perform this test before prescribing AZA. Among the 12 centres that reported target metabolite levels, 10 aim for levels between 200 and 300 pmol/8 × 108 red blood cells (RBC).
About 24/36 centers routinely incorporate PPIs into steroid treatment protocols, seven prescribe PPIs solely when there are risk factors for peptic ulcer disease, and the remainder refrain from using PPIs unless gastrointestinal symptoms occur.
My take: There is a great deal of variation in the management of autoimmune hepatitis indicating the need for more collaborative efforts to advance evidence-based therapeutic strategies.
MT Fioretti et al. J Pediatr Gastroenterol Nutr. 2025;80:300–307. A decade of real-world clinical experience with 8-week azithromycin–metronidazole combined therapy in pediatric Crohn’s disease
Methods: This retrospective study over 10 years examined the efficacy of azithromycin-metronidazole for induction treatment in 44 children. All patients were given metronidazole (15–20 mg/kg/day two times daily, maximum of 1000 mg/day) administered daily for 8 weeks and azithromycin (7.5 mg/kg to a maximum of 500 mg/once a day) administered 5 days per week for the first 4 weeks, followed by 3 days per week for the final 4 weeks as per the initial publications.17, 18
Key findings:
After 8 weeks, the overall remission rate was 64%.
Of the 38 patients who completed the CD AZCRO course, 28 patients (74%) entered remission (Group 1) and 10 (26%) did not (Group 2)
After 8 weeks, Group 1 showed improved CRP levels and higher albumin and hemoglobin levels than Group 2. Median FC declined significantly from 650 mcg/g at baseline to 190 mcg/g at Week 8 in Group 1 (p < 0.001).
The authors conclude that “a combination treatment of azithromycin and metronidazole represents an alternative induction therapy for mild to moderate pediatric CD, offering benefits in terms of cost and practicalities compared to EEN and in side effects compared to steroids.”
My take: There are a small number of children with mild Crohn’s disease who could benefit from this induction regimen. An alternative would be the use of a more modest dietary approach (eg. Mediterranean diet)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.