Personal pet peeve: I receive so many unwanted promotional materials from pediatric hospitals and pediatric gastroenterology divisions from across the country. This is such a waste of paper and effort. Presumably, this is an endeavor to raise the profile of these institutions and programs.
If anyone reading this blog has any role in this, please stop sending this crap and only send this material to alumni or those that request (opt-in) it.
“Alex Benigno, 45, has spent the past 10 months riding his ElliptiGO stand up bike around town, picking up nails, screws and other little annoying things that cost drivers tons of money.” Now he has picked up more than 280 pounds of metal off the street.
“Clark Howard gets a hug from his son Grant Howard before the start of the Atlanta Habitat for Humanity dedication of the 98, 99, and 100th Howard’s sponsored homes in Atlanta on Saturday, April 13, 2024.”
My take: Recently, one of my patients who had been neglected was being taken care of by elderly couple. In addition to this infant, this couple had helped about 80 children over several decades. Everyday I see people who are making this world a better place -not all of them are in the news. It really is an inspiration.
This study included 9 RCTs involving a total of 445 participants. Key findings:
Though some of the study findings seemed to favor prebiotics, all evidence was of very low certainty.
“There may be no difference in occurrence of clinical relapse when adjuvant treatment with prebiotics is compared with adjuvant treatment with placebo for maintenance of remission in UC.”
“Adjuvant treatment with prebiotics may result in more total adverse events when compared to adjuvant treatment with placebo for maintenance of remission. The evidence was of low certainty.”
My take: Currently, there is no solid evidence to recommend prebiotics in patients with ulcerative colitis.
“The Federal Trade Commission on Tuesday said employers could no longer, in most cases, stop their employees from going to work for rival companies.
The sweeping action could help create jobs, raise wages and increase competition among businesses, the agency said. But the action is all but certain to be challenged in court by businesses that say they need to protect trade secrets and confidential information…Noncompetes cover about 30 million U.S. workers..”
[It is estimated that] “the decision would lead to the creation of 8,500 start-ups in a year and up to $488 billion in increased wages for workers over the next decade.”
“The rule would become law 120 days after it is published in the Federal Register, which will probably happen in a few days. But legal challenges could delay or block the change…It orders employers to notify nonexecutive employees bound by an existing noncompete that it will no longer be enforceable.”
There is a carve out: STAT (4/23, Bannow, Subscription Publication) reports: “Crucially for the health care industry, the noncompete ban does not apply to nonprofit companies, as the FTC determined it only has jurisdiction over for-profit companies.” This “means the ban likely won’t apply to most of the country’s hospitals, the majority of which are nonprofit, and some of the country’s biggest health insurers.”
My take: Noncompete agreements at the time of a job offer occur when prospective employees are vulnerable and have limited negotiating power. Established business with market dominance will need to use other ways besides coercion to keep talented employees when noncompete clauses go away.
This lengthy article details “a little-known data analytics firm called MultiPlan. It works with UnitedHealthcare, Cigna, Aetna and other big insurers to decide how much so-called out-of-network medical providers should be paid. It promises to help contain medical costs using fair and independent analysis.”
“But a New York Times investigation, based on interviews and confidential documents, shows that MultiPlan and the insurance companies have a large and mostly hidden financial incentive to cut those reimbursements as much as possible, even if it means saddling patients with large bills. The formula for MultiPlan and the insurance companies is simple: The smaller the reimbursement, the larger their fee.”
The backdrop on MultiPlan was a scandal 15 years ago. The NY Attorney General concluded that the insurance companies had “a payment system riddled with conflicts of interest had been shortchanging patients, and at its core was a data company called Ingenix. Insurers used the company, a UnitedHealth subsidiary, to unfairly lower their payments and shift costs to patients, the probe found…UnitedHealthcare, Cigna, Aetna and other major insurers agreed to replace Ingenix with a nonprofit that would provide independent pricing data…The companies were required to use the nonprofit database for only five years.” Subsequently, the insurance companies turned to Multiplan. In a 2015 email, a Cigna risk officer:: “We cannot develop these charges internally (think of when Ingenix was sued for creating out-of-network reimbursements). We need someone (external to Cigna) to develop acceptable” rates, she wrote.
Some of the examples of out-of-network charges in the article included:
Gail Larson had surgery on a non-healing chest wound. “UnitedHealthcare, advising that Dr. Rabinowitz would be paid $5,449.27 — a small fraction of what he had billed the insurance company. That left Ms. Lawson with a bill of more than $100,000.”
“Kelsey Toney, who provides behavioral therapy for children with autism, who was receiving a payment of half the medicaid rate for providing care.”
“Cari Campbell, who received fertility treatment in Minnesota, was charged thousands of dollars.”
“Justin Dynlacht, who has Crohn’s disease, paid extra for a plan that covered such visits. After seeing two in-network doctors about persistent abdominal pain, he went to an outside specialist who discovered a hernia containing abdominal tissue. Aetna sent the specialist’s claims to MultiPlan, and Mr. Dynlacht was left with thousands of dollars in bills.”
My take: Insurance companies in coordination with Multiplan rip off their policy holders by not providing reasonable coverage for their out-of-network medical care. Ultimately, patients will be increasingly affected as many physicians/hospitals walk away from insurers who are offering low reimbursement rates to in-network providers too. Insurance companies are incentivized to not care.
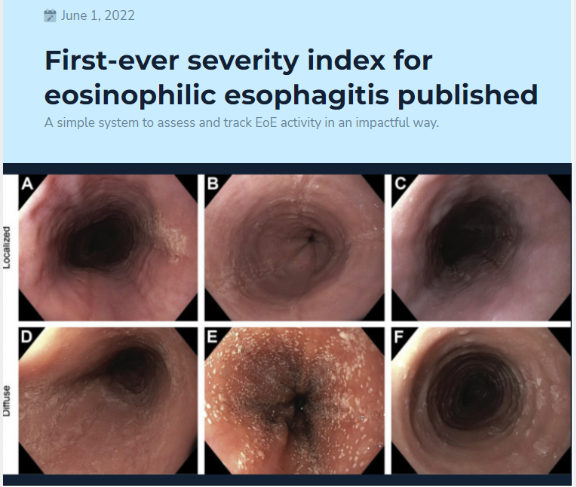
This was a retrospective analysis on a prospectively enrolled cohort of children at a single center who were treated as part of routine clinical care. I-SEE was calculated at the diagnostic and follow-up endoscopies over a mean of 6.6 years.
Key findings:
Of 67 children who met study criteria of at least 3 endoscopies over at least 2 years of follow-up time, 43%, 36%, and 21% had mild, moderate, and severe I-SEE scores at baseline, respectively.
By the last instance, the overall I-SEE score dropped to 3.9 (P < .001). Body mass index <5% and poor feeding were more common in the children with severe I-SEE scores at baseline, and both improved by the last instance.
The discussion notes that I-SEE metric was developed to determine EoE severity and for tracking purposes to gauge effectiveness of therapy. They note that most patients improved but a score of 0, indicating deep remission, was difficult to achieve at the population level. They also anticipate further modifications to I-SEE “such as age or an assessment of symptoms that reflects inflammatory or fibrotic disease.”
My take: I-SEE provides a way to objectively assess and follow EoE severity at all ages.
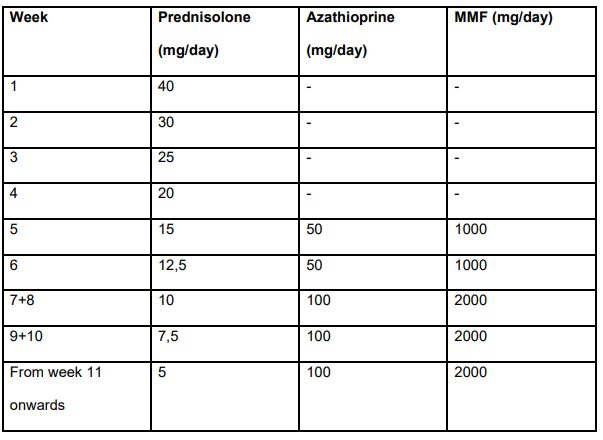
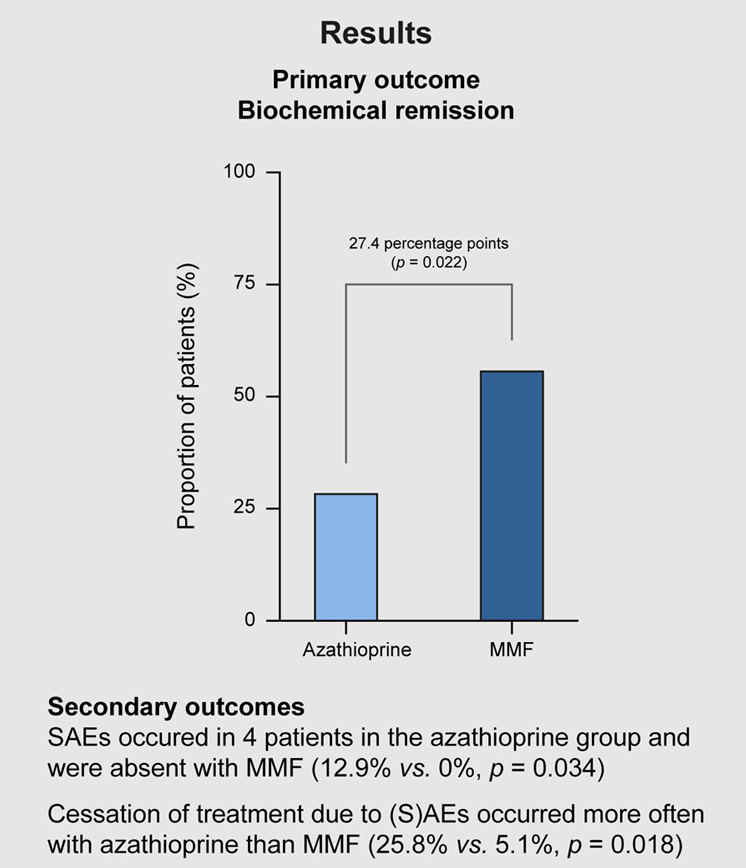
Methods: In this 24-week, prospective, randomised, open-label, multicentre superiority trial, 70 patients (mean age 57.9 years) with treatment-naive AIH received either MMF or azathioprine, both in combination with prednisolone. The primary endpoint was biochemical remission (BR) defined as normalisation of serum levels of alanine aminotransferase and IgG after 24 weeks of treatment.
Treatment dosing in study (Table S2):
Key findings:
56.4% of the MMF group and 29.0% of the azathioprine group achieved BR
No serious adverse events occurred in patients who received MMF (0%) but serious adverse events were reported in four patients who received azathioprine (12.9%) (p = 0.034)
Excerpts from the discussion:
“The evidence for the current standard induction therapy in AIH with azathioprine and prednisolone is limited and stems from the early seventies of the last century.”
“Patients assigned to azathioprine were significantly more prone to discontinuing treatment because of intolerance or SAEs, with nausea and vomiting as the main reasons for cessation of treatment.”
“MMF exhibits high teratogenicity. MMF should not be used during pregnancy and may only be used with strict contraceptive measures in women of childbearing age and men planning to father a child, as its use is absolutely contraindicated during pregnancy.”
“In addition, MMF must be administered twice daily, while azathioprine is given as a single dose daily…relevant for a disease that requires lifelong treatment.”
My take: This study needs to be replicated in the pediatric age group. Though many patients have some frequent side effects with MMF, the overall safety (and possibly effectiveness) appears improved with MMF compared with azathioprine.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this Swedish study with 294 randomized participants who had with moderate to severe I.B.S, 96 assigned to the LFTD (low FODMAPs with IBS advice) diet, 97 to the low-carbohydrate diet, and 101 to optimised medical treatment. Response was defined as a reduction of 50 or more in IBS-SSS compared with baseline.
Key findings:
Response rate after 4 weeks: 73 (76%) of 96 participants in the LFTD diet group, 69 (71%) of 97 participants in the low-carbohydrate diet group, and 59 (58%) of 101 participants in the optimised medical treatment group
An excerpt: “A new study suggests that certain dietary changes may be more effective than medication..When she checked on the participants during the trial, one from the low-FODMAP group cried when she described how much better she felt on the diet. Another in the low-carbohydrate group said she “never in her life had felt so good in her stomach,” Dr. Nybacka said…
Dr. Chey said the study was well done and provided “real data” to support what many doctors have observed: That “diet therapy is at least as good and probably better” than medication.
My take: Dietary therapies and psychological therapies are underutilized in the management of IBS. For those using dietary therapies, counseling with a nutritionist is a good idea.
“GLP-1 RAs (eg, semaglutide, tirzepatide, exenatide, liraglutide, albiglutide, dulaglutide, and lixisneatide) mimic incretins, which are hormones released after eating that prompt glucose-dependent insulin release from the pancreatic islets, stimulate satiety centers, inhibit glucagon release, and result in diminished gastric emptying.”
Because GLP-1 RAs diminish gastric emptying, they can increase the risk of residual gastric contents prior to surgery and endoscopy.
AGA Recommendations:
“If patients taking GLP-1 RAs solely for weight loss can be identified beforehand, a dose of the medication could be withheld before endoscopy with likely little harm, although this should not be considered mandatory or evidence-based. Nevertheless, it is unclear if withholding the medication for only one dose would be reliably adequate for an individual’s gastric motility to return to normal. ..there is insufficient evidence to suggest this practice be performed for patients taking these medications to treat diabetes”
“Generally, in patients on GLP-1 RAs who have followed standard perioperative procedures (typically an 8-hour solid-food fast and a 2-hour liquid fast) and who do not have symptoms of nausea, vomiting, dyspepsia, or abdominal distention, we advise proceeding with upper and/or lower endoscopy.”
“When possible, placing patients on a liquid diet the day before sedated procedures may be a more acceptable strategy, in lieu of stopping GLP-1 RAs.”
My take: This guidance provides useful advice given the increasing use of GLP-1 RAs. If these medications are being used for obesity, holding a dose prior to endoscopy is a good idea.
Related article: S Sen et al. JAMA Surgery 2024; doi:10.1001/jamasurg.2024.0111.Glucagon-Like Peptide-1 Receptor Agonist Use and Residual Gastric Content Before AnesthesiaKey finding: Use of a GLP-1 RA was independently associated with increased residual gastric content (1.5 mL/kg of clear liquids on gastric ultrasonography) on preprocedural gastric ultrasonography: 56% (35 of 62) in patients with GLP-1 RA use (exposure group) compared with 19% (12 of 62) in patients who were not taking a GLP-1 RA drug (control group).
This is at the entrance to the Westside Reservoir Park. I had the chance to go there as part of a Westside Beltline Tour in Atlanta.This reservoir is as deep as the Statue of Liberty is tall and can hold 2.4 billion gallons of water for the city of Atlanta
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
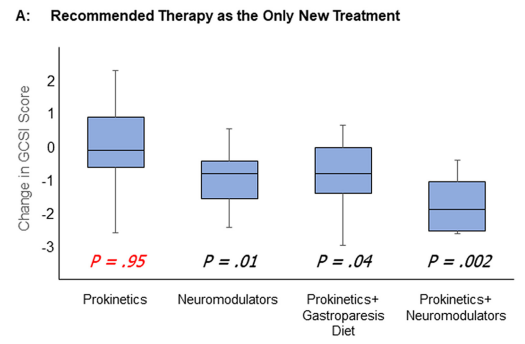
Methods: In this prospective study of patients (n=129) with suspected gastroparesis, the authors examined longitudinal outcomes focusing on responses to prokinetics and other therapies. This included gastroparesis diets and neuromodulators. Patients underwent validated gastric emptying testing (wireless motility capsule and gastric emptying scan) before recommending new treatments.
Prokinetics included dopamine antagonists, motilin agonists, acetylcholinesterase inhibitors, and pyloric botulinum toxin injection.
Key findings:
“Initiating prokinetics as solo new therapy had little benefit for patients with symptoms of gastroparesis.”
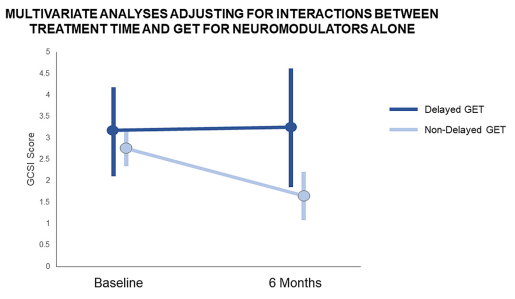
“Neuromodulators as the only new therapy decreased symptoms other than nausea and vomiting”
Combination therapy of a prokinetic with a neuromodulator appeared to be the most effective
Neuromodulators were mainly effective in those without delayed gastric emptying times
My take: Our therapies for gastroparesis are not very good. And, neuromodulators are likely to be more helpful than prokinetics.