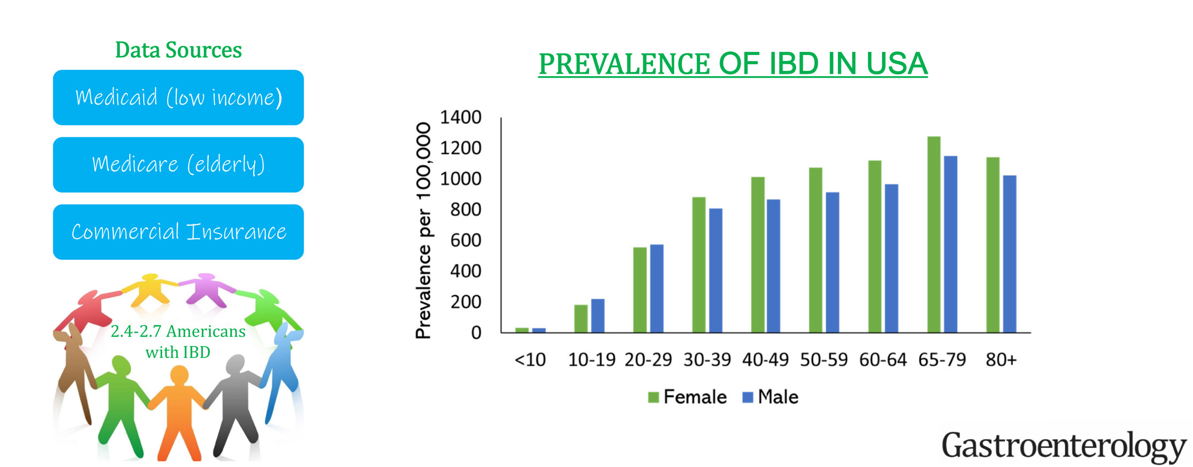
This “INPUT” (INcidence, Prevalence, Treatment and OUTome in Patients with IBD) study used 4 different data sets to provide “the clearest depiction to date of IBD [epidemiology] in the U.S.
Key findings:
The age-, sex- and insurance-standardized prevalence of IBD was 721 per 100,000 population. This equates to estimated 2.39 million Americans with IBD.
Sub-category prevalence: the prevalence of IBD per 100,000 population was 812 in White, 504 in Black, 403 in Asian, and 458 in Hispanic Americans.
My take: The prevalence of IBD continues to increase and the U.S. has one of the highest rates in the world.
Background: Stool H pylori testing “has become available and is based on the detection of mutations in H pylori genome associated with antimicrobial resistance and corresponds well with resistance determined by culture”
Methods: The authors obtained stool susceptibility testing using a novel NGS-based analysis and compared results with the current “gold standard” of gastric biopsy culture via agar dilution in 20 pediatric patients with evidence of H pylori in gastric biopsies. Stool samples were sent to American Molecular Laboratories (description in supplemental material). Gastric samples were sent to Mayo Laboratories.
Key findings:
Stool NGS-based antimicrobial susceptibility analysis was highly concordant with agar dilution (gastric biopsies) for no resistance (100% agreement), as well as clarithromycin, levofloxacin, and amoxicillin resistance (100%, 67%, and 100% agreement, respectively) but not concordant for metronidazole in our cohort of patients.
35% of patients had antibiotic resistance identified
My take: Since H pylori is difficult to treat, identifying susceptibility patterns can be very helpful. This study shows that stool specimens have good agreement with gastric biopsy testing. While the results for metronidazole are not as good, resistance to metronidazole can often be overcome as part of multidrug regimens.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A new and promising approach — which Dong, Rao, and their colleagues describe in the journal Nature — focuses on curbing intestinal inflammation rather than fighting the bacteria directly…
In response to the toxin, the sensory neurons secrete the neuropeptides substance P and calcitonin gene-related peptide (CGRP), while the pericytes, which surround blood vessels, produce pro-inflammatory cytokines. In a mouse model, this drove intense neurogenic inflammation and tissue damage —the same kind of damage that occurs in patients…
FDA-approved drugs already exist to block the triggering neuropeptides. Aprepitant, used for nausea and vomiting, blocks substance P signaling. Small molecules related to olcegepant or monoclonal antibodies such as fremanezumab, used for migraines, inhibit CGRP signaling.
In the mouse model, these drugs reduced inflammation and tissue damage. Somewhat surprisingly, they even reduced the burden of C. diff bacteria in the animals’ intestines.
My take: Clinical trials are needed to see if these therapies can improve outcomes more than current treatments.
Situation: Brand name Flovent HFA will no longer be manufactured after December 31, 2023.
Background: • Flovent HFA is a commonly utilized swallowed topical steroid treatment for patients with eosinophilic esophagitis (EoE). It works by the patient swallowing the aerosolized medication dispensed by a metered dose inhaler (MDI). • Both Medicaid and many private insurance formularies have transitioned to breath-actuated inhalers as their preferred inhaled steroid formulation, which cannot be used for EoE because they cannot be swallowed. • GlaxoSmithKline will be discontinuing manufacture of brand Flovent HFA after December 31, 2023. While an authorized generic fluticasone HFA is available, it is not listed on many insurance formularies and for those that do include it, it is typically not listed as a preferred medication. • Two other steroid MDIs are available on the market – Alvesco HFA (ciclesonide) and Asmanex HFA (mometasone). Limited data is available regarding dosing and efficacy in EoE 1,2. • We are actively working to raise these concerns with major payors.
Assessment & Recommendation: Given upcoming Flovent HFA discontinuation, patients needing this formulation of drug could be switched to generic fluticasone HFA. For many insurances this may require a prior authorization, which may delay initiation of the medication and families should be counselled accordingly.
In those whom generic fluticasone HFA is denied despite submission of a prior authorization, alternative options include: • Oral viscous budesonide • Swallowed topical Asmanex (mometasone) HFA or Alvesco (ciclesonide) HFA. Data on dosing in EoE is limited and these medications are also likely to require a PA.
References: 1. Tytor J, Larsson H, Bove M, Johansson L, Bergquist H. Topically applied mometasone furoate improves dysphagia in adult eosinophilic esophagitis – results from a double-blind, randomized, placebo-controlled trial. Scand J Gastroenterol. 2021 Jun;56(6):629-634. doi: 10.1080/00365521.2021.1906314. Epub 2021 Apr 8. PMID: 33831327. 2. Nistel M, Nguyen N, Atkins D, Miyazawa H, Burger C, Furuta GT, Menard-Katcher C. Ciclesonide Impacts Clinicopathological Features of Eosinophilic Esophagitis. J Allergy Clin Immunol Pract. 2021 Nov;9(11):4069-4074. doi: 10.1016/j.jaip.2021.06.058. Epub 2021 Jul 19. PMID: 34293498.
The information provided is intended solely for educational purposes and not as medical advice. It is not a substitute for care by a trained medical provider. NASPGHAN does not endorse any of these products and is not responsible for any omissions. For additional information please email floventquestions@naspghan.org.
Any substitution should only be done under the recommendation and supervision of a healthcare professional.
I have not been an enthusiastic early adopter of teduglutide. Though it has been shown to reduce HAL volumes in those with short bowel syndrome (SBS), this tends to revert with cessation of treatment. In addition, it has a very high cost and long-term adverse effects are unclear. Currently the manufacturer recommends a colonoscopy after 1 year of treatment.
This case report by Salazar et al identified two children who developed foveolar hyperplastic gastric polyps after receiving teduglutide.
Discussion points:
“There have been increasing reports of both benign and malignant small bowel polyp development. In trials of pediatric patients, limited to 12 and 24 weeks, initial upper endoscopy and colonoscopies were not required. In addition, postexposure upper endoscopy and colonoscopy was not the standard of care (9,13,16). Thus, the incidence of intestinal polyp formation on teduglutide treatment in pediatric patients remains unknown.”
“A recent retrospective review of adult patients with SBS showed increased small bowel polyp formation in 8 out of 35 patients (22.9%) on long-term teduglutide use… 3 were identified as adenomas with low-grade dysplasia… (14)”
“In general, isolated foveolar hyperplasia has not been identified as a premalignant lesion…The connection between foveolar hyperplasia and development of dysplasia, though, remains poorly understood, and further work delineating the natural history of foveolar polyps in the context of teduglutide is important.”
Related article: A Fifi et al. JPGN 2023; 77: 666-671. This is a post-hoc analysis showing improving stool consistency in 101 patients treated in open-label studies. Patients had mean drop of 20 mL/kg/day in parental fluid volume (compared to 7 mL/kg/day in the standard care treatment group).
My take: This case report indicates that endoscopic monitoring (possibly both upper endoscopy and colonoscopy) is needed in teduglutide-exposed patients. In addition, careful consent of the patients is prudent indicating the uncertain long-term effects. Finally, it would be a good idea to enroll all patients in a registry as well.
JB McCannon et al. NEJM 2023; 389: 1902-1911. Case 35-2023: A 38-Year-Old Woman with Waxing and Waning Pulmonary Nodules
In this case report, A 38-year-old woman was evaluated because of dyspnea, chest discomfort, and waxing and waning pulmonary nodules. She had a prior history of ulcerative colitis. This article reviews reasons for pulmonary nodules including cancer, infection, vasculitis, connective tissue disorders, sarcoidosis and inflammatory bowel disease (IBD) which has a number of pulmonary manifestations including necrobiotic nodules.
In this case, the granulomatous lung disease was attributed to be an extraintestinal manifestation of IBD. She was treated with TNF-alpha targeted therapy which has been effective in a prior case report (J Crohns Colitis 202; 14: 480-489).
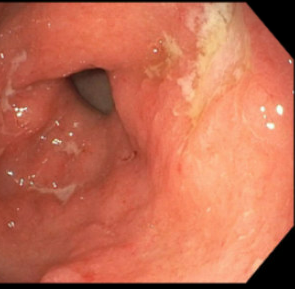
My first reaction to this article — I have seen this! However, our case was atypical in that the 15 year old patient presented with respiratory symptoms (no preceding GI diagnosis). It was noted that her gastric wall was severely thickened as an incidental finding on her chest CT which showed extensive tiny pulmonary nodules. Her endoscopy showed disease isolated to her stomach. Both her gastric findings and CT of her chest resolved with infliximab treatment. This included mucosal healing of her stomach on followup endoscopy.
CT scan showing severely thickened gastric wallMucosal appearance of stomach with erythema and numerous ulcerations prior to treatment
Related blog post: IBD Update January 2015 (Part 1)NEJM 2014; 371: 2418-27 -case report of 9 yo with Crohn’s Disease and pulmonary nodules
In this Swedish cross-sectional cohort study with 162 children who had been diagnosed with celiac disease (CD) between 2013-2018, the authors examined the outcomes of children who had continued follow-up compared to those who had not been seen in 24 months. The average disease duration of study participants was 5.3 years.
Key findings:
Similar rates of TTG IgA normalization: 94% vs 91% for those without and those with follow-up respectively
Similar rates of very good dietary adherence 65% vs 72% for those without and those with follow-up respectively
Lack of follow-up was not significantly associated with growth, symptom scores, or HRQoL.
It is possible that there is a selection bias in that patients without symptoms may be less likely to followup.
My take: Based on this study, it looks like good education after diagnosis is crucial and that regular follow-up is less important in achieving good outcomes.
In this retrospective single-center study with 76 pediatric patients with Hirschsprung’s disease (HD), the authors compared the outcomes of those who had associated syndromes (or neurocognitive issues) (SA-HD, n=24) to those with isolated (I-HD, n=52). Most patients had undergone a Soave procedure (n=67). Only 11 patients were available for followup data at 10 years of age.
Key findings:
SA-HD patients became bowel continent at a significantly older age (mean age 8.43 vs 4.94 years)
SA-HD patients had urinary incontinence at a significantly older age (P = 0.0136, 5 years)
SA-HD patients had more constipation at all ages: at age 3 years (29% vs 17%), at age 5 years (55% vs 22%), and at 10 years (83% vs 20%)
SA-HD included Down syndrome (38%), cognitive impairment (29%), MEN (8%), hypoventilation syndrome (aka Ondine) (8%), oro-facio-digital (8%), Smith-Lemli-Opitz (4%) and Bardet-Biedl (4%). The authors note that expected toilet training completion for Down syndrome is between 4.7-6.6 years of age compared to 2.3-3.4 years for neurotypical kids.
My take: Since SA-HD includes children with high rates of cognitive impairment, it is not surprising that there were delays in toilet training, higher rates of constipation and higher rates of urinary retention.
Diagrams of 3 common pull-through operations for Hirschsprung disease. From left to right: full-thickness rectosigmoid dissection (Swenson), a recto-rectal pouch procedure (Duhamel), and an endorectal dissection (Soave). JPGN 2023; 76(4):533-546.
In this single-center retrospective cohort, the authors analyzed 67 pediatric patients with rectal prolapse who had surgical evaluation; the median duration of follow-up was nearly 4 years.. Key findings:
The resolution rate with surgery as initial management was 79% (n = 11/14). Medical management included stool softeners, avoiding straining, and minimizing time on toilet.
The resolution rate was 33% (n = 8/24) with sclerotherapy alone and additional 21% (n = 5/24) resolving after a subsequent surgical procedure
Medical management was successful in 100% (n=29) (patients who responded would not need subsequent procedural approach); 27 of these patients were less than 5 years of age.
82% of patients had constipation
A psychiatric comorbidity was noted in 24 patients, 19 of whom had either sclerotherapy (n=12) or surgery (n=7).
The authors note that rectal prolapse is often self-limited with reported spontaneous resolution of 60-90%. The treatment algorithm proposed by the authors is for medical management alone if less than 5 years of age. In children older than 5 years, they recommend initial sclerotherapy (with D50W) followed by surgical correction (rectopexy or transanal resection of the prolapsing segment) if not successful after one session.
My take: I have not had to refer a patient for surgical management in more than 25 years of clinical GI practice. However, in patients older than 5 years, surgical approaches (rectopexy or resection of prolapse) may be needed in highly selected patients, like in this study which only included patients seen by surgery (referral bias).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This article starts off discussing a recent trend of how medical problems are often described as a “journey.” However, the main focus is the trend of hospitals developing expensive amenities further adding to huge medical bills.
An excerpt:
So much of being seriously ill has been rebranded in American health care as a kind of adventure…But on these journeys, you don’t get to go anywhere—except maybe the hospital or doctor’s office, which is likely, too, to have bought into the travel concept. In the past two decades, American hospitals have gotten into the business of hotel-like hospitality (illness can be fun!) rather than confine themselves to the business of disease (what a downer). And although the care might stay solid, the focus on luxurious amenities and the fancy new buildings that house them is one of the factors that have helped send costs for patients soaring that much higher, to prices well above those in other developed countries…
In recent years, tight budgets, staffing shortages, and burnout have hit American hospitals. At the same time, many health centers in the U.S.—including the most prestigious ones, and even some community hospitals—have morphed into seven-star hotels…A hospital might now boast about its views, high-thread-count sheets, or food provided by a Michelin-starred chef…
Back in 2008, researchers at the National Bureau of Economic Research estimated that a hospital investing in amenities would increase demand by 38 percent, whereas a similar investment in clinical quality would lead to only a 13 percent increase…
These amenities have a cost, and they are not worth nearly what we’re paying for them as we’re billed for $100,000 joint replacements and $9,000 CT scans. Room charges in many hospitals can exceed $1,000 a night. And “facility fees” for outpatient procedures and even office visits can reach hundreds of dollars, and simply don’t exist elsewhere. A hospital’s function is to diagnose and to heal, at a price that sick people can afford. I dream of a no-frills Target- or Ikea-like hospital for care…
How about focusing on the very basic things that health systems in the U.S. should do, but—in my experience—in many cases do not, like making it easier for patients to schedule appointments? Shortening the now lengthy wait times to see physicians who take insurance plans? Paying for adequate staffing on nights and weekends, so patients don’t linger in bed pointlessly for two days until social workers return on Monday? Or ending those two-day stays in emergency rooms when all inpatient beds are full?