9/5/23 CNN: Delta flight forced to turn around because of diarrhea incident ““It’s just a biohazard issue, we had a passenger who had diarrhea all the way through the airplane so they want us to come back to Atlanta,” a DL 194 pilot said to air traffic control.”
When a family member saw this, he wondered if someone on the plane yelled: “Is There a Gastroenterologist on This Plane?”
My take: In this case, as with a lot of GI symptoms, having a good cleaning crew is usually more important than having a good physician. And, what a terrible situation!
The retrospective study by Zimmerman et al involved 170 pediatric patients (IFX (n = 84) and TAC (n = 86)) with acute severe colitis (ASC) form 2005 to 2017; TAC was generally used prior to 2014 and patients were more likely to be receiving 6MP as a long-term maintenance agent; the mean TAC level was 10.7 ng/mL. The mean dose of infliximab (IFX) initially was 7 mg/kg. Key findings:
The rate of colectomy 6 months from rescue therapy was similar whether patients received IFX or TAC (22.6% vs 26.7%, respectively, P = 0.53).
The mean decline in Pediatric Ulcerative Colitis Activity Index scores from admission to discharge in those treated with IFX (31.9) or TAC (29.8) was similar (P = 0.63).
Similar rates of adverse effects were seen. 4 patients in the TAC group experienced neurologic symptoms.
About half of the steroid-refractory ASC patients failing either agent as initial rescue therapy required colectomy, even if they switched to the alternative agent.
17.9% of patients receiving high-dose IFX required colectomy by 6 months compared to 25% in the “typical” IFX dosing group; this was not statistically significant, likely due to limitations of sample size.
In the systematic review/meta-analysis study by Bolia et al., the authors identified 7 studies with 166 children (111 steroid-refractory, 52 steroid-dependent, 3 no steroids). The majority of cases (150/166 [90%]) were naïve to biologics. None of the participants in these studies have been treated recently (only 10 patients since 2014 and none after 2016). The two most recently published studies in 2018 and 2019 had enrollment in 2014-2016 and 2000-2012, respectively. Key findings:
An initial response to tacrolimus therapy was seen in 84%
No difference was observed between children with high (>10 ng/mL) or low tacrolimus levels (127/150 [85%] vs 12/16 [75%], P = 0.3).
The pooled frequency of 1-year colectomy-free survival in children treated with initial oral tacrolimus was 64% (95% CI: 53%–75%). Twelve (7.2%) patients required cessation of therapy because of side effects.
My take: Both of these studies indicate that tacrolimus could be a useful agent for ASC and may find a role as a bridge therapy for biologic agents with slower onset of action.
Treatments for “Bad” Inflammatory Bowel Disease (Part 3) **An alternative agent to cyclosporine is tacrolimus. Hamel B, Wu M, Hamel EO, Bass DM, Park KT. Outcome of tacrolimus and vedolizumab after corticosteroid and anti-TNF failure in paediatric severe colitis. BMJ Open Gastroenterol. 2018;5(1):e000195
A couple good review articles (though behind paywall):
PT Reeves, L James-Davis, M Khan. Neoreviews 2023;24(7):e403-e413. Gastrointestinal Bleeding in the Neonate: Updates on Diagnostics, Therapeutics, and Management This reviews covers the most important etiologies of GI bleeding in the neonate. A few interesting points were the potential use of calprotectin as a potential screen for necrotizing enterocolitis; “the median fecal calprotectin levels in infants with NEC were between 210 and 400 mg/g of stool.” The authors also point out that there is “limited evidence for performing endoscopy in infants with GIB…][In one study] Only 3 of 56 infants underwent therepeutic intervention during endoscopy. Five percent (n=3) of these neonates exhibited gastrointestinal perforation in the acute postoperative period after endoscopy.”
The article notes that meconium is typically passed in 24 to 48 hours after gastrograffin enema and recommends abdominal imaging every 8 to 12 hours after enema administration to exclude perforation along with adequate intravenous hydration (“at least 150 mL/kg per day”).
The actual article has many other useful points. For example:
CFTR is not expressed in hepatocytes; “however, liver injury may occur patients with CF due to proximity to cholangiocytes (which may be inflamed) and/or through increased intestinal permeability.”
Elastase levels are not affected by exogenous pancreatic enzyme supplementation and is expected to display levels within the normal adult range by 2 weeks of age.
Sodium deficiency is common and needs to be prevented with sodium supplementation in first 12 months of life (one-eighth teaspoon (= 12.5 mEq) of salt in first 6 months, and one-fourth teaspoon (=25.2 mEq) from 6-12 months)
The newest CFTR modulator, elexacaftor/tezacaftor/ivacaftor is approved for children 2 years of age and older
There are case reports of in utero exposure to CFTR modulators associated with resolution/prevention of disease (eg. pregnant women starting CFTR-targeted treatment at 32 weeks gestation which resolved meconium ileus).
K McNelis, ME Rogers, S Kocoshis. Neoreviews. 2023 Jul 1;24(7):e431-e439. Pediatric Intestinal Transplantation Management and Outcomes This is another useful review for pediatricians. Pediatric intestinal transplantation is most commonly (65%) related to short bowel syndrome, 20% due to motility disorders, 9% due to mucosal diseases, 5% due to retransplantation and 1% are due to a variety of causes. The evaluation and management of patients needing intestinal transplantation is succinctly summarized. “Overall, survival of pediatric patients after intestinal transplantation is 72.7% at 1 year and 57.2% at 5 years. The most common causes of death are sepsis/multiorgan system failure and cardiovascular/stroke (Fig 2).” Also, “current statistics about organ transplantation can be publicly accessed by health care team members, patients, and families at srtr.transplant. hrsa.gov.” This site also includes data on transplantation for kidney, pancreas, heart, lung and liver.
After a literature review, the authors included 10 studies reporting semen parameters (268 patients with IBD) and 16 studies reporting adverse pregnancy outcomes (over 25,000 patients with IBD). Key findings:
Biologic, thiopurine, or methotrexate use were not associated with decreased sperm count, motility, or abnormal morphology compared with nonexposed patients.
Biologic, thiopurine, or methotrexate use among male patients with IBD are not associated with increased odds of adverse pregnancy outcomes
This retrospective study of patients with trisomy 21 (T21) who underwent EGD between 2000-2020. Key findings:
Among 836 patients with T21, 419 (50.1%) of whom had duodenal histologic abnormalities.
290 of 419 had villous atrophy (VA) and of those, 172 of 290 met celiac disease (CD) diagnostic criteria, while 118 of 290 did not meet CD criteria (nonspecific VA).
Only one of the 118 with nonspecific VA had markedly abnormal celiac serology (TTG IGA >10 times ULN) but had no IELs on biopsy and did not respond to GFD. Four patients with nonspecific VA were later diagnosed with celiac disease over a median of 2.5 years with conversion to abnormal celiac serology.
Among the 129 with duodenitis without villous atrophy, 38 (29%) had increased intraepithelial lymphocytes and two patients were diagnosed with CD many years later (development of VA and positive celiac serology.
The authors offer an algorithm (Figure 2) to assist clinical approach based on biopsy results in this population.
In those with no villous atrophy, if Marsh score of 0/1, biopsies not consistent with celiac disease. In those with Marsh score of 2 (which is rare), consider as consistent with celiac disease (see next bullet point).
In those with villous atrophy consistent with celiac disease, assess response to gluten free diet (GFD). In those without a response, consider RD consult to evaluate exposures and HLA-typing as next steps.
In those with villous atrophy NOT consistent with celiac disease, obtain serology (TTG IgA, EMA, IgA, DGP IgG). If serology is negative, consider peptic duodenitis or SIBO treatments and assess/discontinue medications for potential for mucosal damage. If serology is positive, consider HLA-typing, review pathology slides, assess for competing disorders, and could need f/u endoscopy.
My take: Overall, ~20% of patients with T21 undergoing endoscopy, will have pathology consistent with celiac disease; this represents ~40% of those with abnormal histology. In the other 60% with abnormal histology, many have alternative explanations for the histologic findings (like peptic duodenitis). Some will evolve to meeting the diagnostic criteria for CD with time indicating need for ongoing monitoring. This study highlights the diagnostic uncertainty in those with potential for seronegative celiac disease.
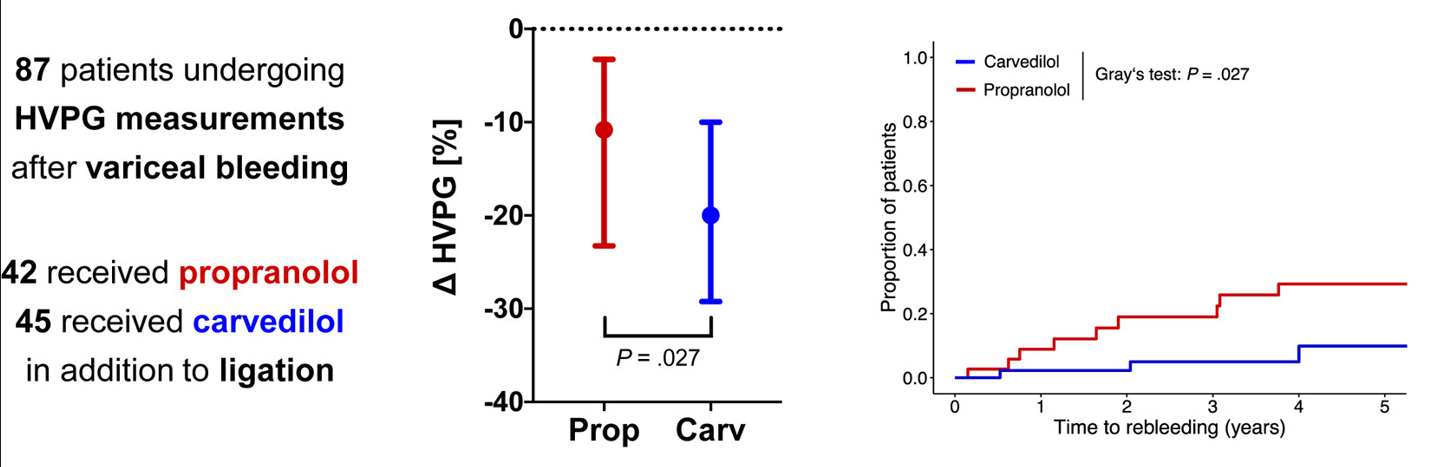
In a retrospective cohort comprising 87 adult patients receiving NSBB (non-selective beta blocker) in addition to band ligation after variceal bleeding, carvedilol induced more profound decreases in hepatic venous pressure gradient compared with propranolol. The higher rate of chronic hepatic venous pressure gradient response to carvedilol (53.3% vs 28.6%; P = .034) was paralleled by lower rates of variceal rebleeding, liver-related death, and further nonbleeding decompensation.
In the discussion and the editorial, it is noted that there is high-quality evidence that carvediol is superior for primary variceal prophylaxis in adults. “Carvedilol increasingly is used for the prevention of variceal bleeding, 2 and, based on the recent landmark PREDESCI study, overall hepatic decompensation/ascites3 in compensated cirrhosis, because it induces HVPG response (a ≥10% decrease in HVPG is sufficient in primary prophylaxis17) in up to 75% of patients vs 50% when using propranolol. However, it induces more pronounced decreases in blood pressure, which may be detrimental in patients with (refractory) ascites.15“
Though there are concerns about dropping blood pressure, the editorial notes that “up to two-thirds of patients with compensated cirrhosis” have high blood pressure. The editorial concludes that “the study still strongly suggests that carvedilol is at least as safe as propranolol…. I am in complete agreement with the authors in suggesting that carvedilol is likely to represent the best NSBB in the treatment of portal hypertension regardless of the clinical scenario, including prevention of decompensation, ascites, first bleeding, or recurrent bleeding.” The author notes that the “recent Baveno VII recommendations declare carvedilol as the preferred NSBB, and support its use in all compensated patients with direct (HVPG ≥10 mm Hg) or indirect signs of clinically significant portal hypertension.”(J Hepatol. 2022; 76: 959-974. Baveno VII: renewing consensus in portal hypertension)
My take: In adults, Carvediol is the best NSBB for portal hypertension. In children, who may be more prone to hypotension, more data is needed.
At the start of my training in pediatric gastroenterology, the serological testing was not reliable and as a result, very few cases of children who did not have a ‘classical’ phenotype (eg. abdominal distention, poor growth, anemia) were diagnosed. The main exception was the diagnosis in children already recognized as high risk (eg. children with type 1 diabetes).
This recent retrospective study indicates that even with improvement in celiac serology, there are cases of seronegative celiac disease (SN-CD) that are difficult to diagnose. In this study, SN-CD diagnosis required clinical correlation and either confirmatory genetics or follow up endoscopy on a gluten-free diet. Key findings:
Of the 424 patients who met celiac disease (CD) criteria, 4.7% (n = 20) fulfilled the criteria for SN-CD
Nearly 65% of SN-CD were IgA sufficient compared with 98.4% in the seropositive group
All SN-CD patients were symptomatic whereas 82% of seropositive group was symptomatic
The discussion notes that it has been understood that the sensitivity of TTG IgA is about 95% and specificity about 96%. However, the authors caution that this may be “largely overestimated due to failure to account for verification bias. Only 3.6% of IgA-ATTG negative individuals were referred for biopsy” in Hujoel et al meta-analysis (J Clin Gastroenterol 2021; 55: 327-334); thus, the sensitivity could be as low as 57% based on this meta-analysis. In addition, gluten restriction prior to serological testing can further reduce the sensitivity of serological tests.
An important limitation of the study is proving that SN-CD was in fact SN-CD and not one of the mimics for CD (eg. inflammatory bowel disease, autoimmune disorders, medication effect). However, they noted that their cohort had followup over 6-9 years and with symptom resolution with a gluten free diet.
My take: Identifying SN-CD is difficult since so many children have similar digestive symptoms unrelated to celiac disease. Most children with vague digestive complaints do not need to undergo endoscopy; as such, SN-CD can be easily overlooked.
Ten males [mean 15.1 years, standard deviation (SD) 2.2] with NASH were randomized to once daily treatment with Elafibranor: 80 mg (n = 5) or 120 mg (n = 5). Elafibranor, a dual peroxisome proliferator-activated receptor α/δ agonist, has been proposed as a treatment for nonalcoholic steatohepatitis (NASH, aka Metabolic dysfunction-associated steatohepatitis (MASH)). Key findings:
End of treatment mean ALT was 52 U/L (SD 20) for the 120 mg group, with a relative mean ALT change from baseline of −37.4% (SD 23.8%) at 12 weeks.
Elafibranor was rapidly absorbed and well tolerated.
My take: I think we are on the verge of identifying medications which will be able to improve outcomes for those with steatotic liver disease.
In this study, 133 ot 184 patients in clinical remission agreed to switch to subcutaneous infliximab. Key findings:
At visit 3, a relapse occurred in 10.2% (n = 6 of 59), 7.3% (n = 3 of 38), 16.7% (n = 3 of 18), and 66.7% (n = 10 of 15) (P < .001) of patients receiving 5 mg/kg every 8 weeks (5Q8W), 10Q8W, 10Q6W, and 10Q4W, respectively.
Dose escalation to 240 mg every other week led to recapture clinical remission in 93.3% (n = 14 of 15).
Infliximab serum levels increased after the switch (P < .0001) except for patients receiving 10 mg/kg every 4 weeks.
Conclusion (borrowed from authors): Switching from intravenous to subcutaneous infliximab 120 mg every other week is safe and well accepted, leading to a low risk of relapse in IBD patients except for those receiving 10Q4W; these patients likely require 240 mg every other week
Reduced (41.7%) or stable (36.8%) serum levels of IFX after the switch (difference: V1-V0) were associated with higher risk of relapse than increased serum levels (>1 μg/mL; 12.7%; P = .020 and P = .019, respectively)
Patients receiving IV infusion of IFX 10Q4W had a higher risk of relapse (odds ratio, 12.4; P = .017). In addition to having significantly higher serum levels than in other IFX IV regimens, this group of patients did not see a rise in IFX concentrations at V1, in contrast to other IFX regimens.
Being overweight increases the clearance of CT-P13 SC, with an increase in clearance of 43.2% for a weight increase from 70 to 120 kg. The presence of antibodies to IFX also increases clearance by 39%. Finally, a decrease in serum albumin level (42 g/L vs 3.2 g/L) increases the clearance by 30.1%.
My take:
Monitoring IFX levels would be helpful in patients switching from IV to SC administration, especially in higher risk groups (eg. high baseline dosing, positive anti-drug antibodies, low serum albumin, overweight individuals)
My experience with SC biologics has been that there is a much higher rate of non-adherence than with IV infusions. If/when SC biologics are used more often, I will need to implement more intensive followup to assure patients receive both the needed medication and the needed monitoring.
A powerful lobbyist convinced a federal agency that doctors can be forced to pay fees on money that health insurers owe them. Big companies rake in profits while doctors are saddled with yet another cost in a burdensome health care system…
In August 2017, a federal agency with sweeping powers over the health care industry posted a notice informing insurance companies that they weren’t allowed to charge physicians a fee when the companies paid the doctors for their work. Six months later, that statement disappeared without explanation.
The vanishing notice was the result of a behind-the-scenes campaign by the insurance industry and its middlemen that has largely escaped public notice — but that has had massive financial consequences that have rippled through the health care universe. The insurers’ invisible victory has tightened the financial vise on doctors and hospitals, nurtured a thriving industry of middlemen and allowed health insurers to do something no other industry does: Take one last cut even as it pays its bills.
Insurers now routinely require doctors to kick back as much as 5% if they want to be paid electronically. Even when physicians ask to be paid by check, doctors say, insurers often resume the electronic payments — and the fees — against their wishes...
Dr. Alex Shteynshlyuger, a urologist who runs his own clinic in New York City, made it his mission to take on both the insurers and the federal bureaucracy. He began filing voluminous public records requests with CMS.
My take: This article shows another layer of a broken health care system where the ‘frauds are legal.’



















{kind=link}