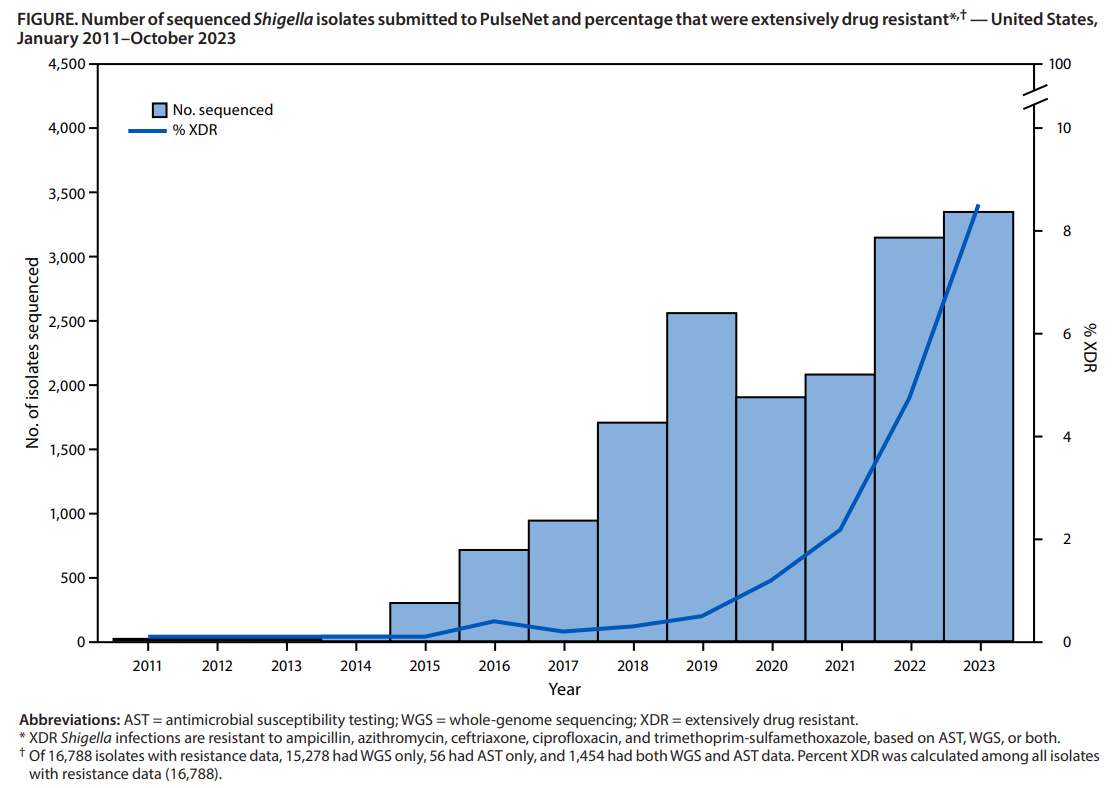
Logan N, Birhane MG, McDonald SL, et al. MMWR Morb Mortal Wkly Rep 2026;75:173–178. Open Access! Emergence of Extensively Drug-Resistant Shigellosis — United States, 2011–2023. DOI: http://dx.doi.org/10.15585/mmwr.mm7513a1
Background: “Shigellosis is a nationally notifiable diarrheal illness caused by gram-negative bacteria. Shigella infection is spread through fecal-oral transmission (infection can occur with as few as 10 organisms) and sexual contact. Although most infections are self-limited, antibiotics are indicated for severe illness or to reduce transmission in settings with high risk for spread. Since 2015, a growing proportion of cases has been caused by extensively drug-resistant (XDR) Shigella species, defined as being resistant to ampicillin, azithromycin, ceftriaxone, ciprofloxacin, and trimethoprim-sulfamethoxazole. No Food and Drug Administration–approved oral antimicrobial agents are available to treat these XDR infections.”
Key finding:
- The percentage of Shigella isolates with resistance data that were XDR increased from 0% during 2011–2015 to 8.5% in 2023
Limitations included the following:
- “Surveillance likely underestimated XDR Shigella isolate incidence: not all isolates were sequenced or had AST, many specimens that were positive by culture-independent diagnostic tests were not cultured, underdiagnosis and incomplete reporting occurred>”
My take (borrowed from authors): “It is concerning that resistance is increasing.”XDR Shigella infection is an emerging concern in the United States. Because no oral antimicrobial agents are FDA approved, prevention, early detection, AST-guided therapy, and timely reporting are important to protect populations at higher risk for XDR Shigella infection”
Related blog posts: