NY Times article that summarized recent Lancet study: Medical Workers Should Use Respirator Masks, Not Surgical Masks
Original Lancet Study (DK Chu et al. June 1, 2020
https://doi.org/10.1016/S0140-6736(20)31142-9): Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and
COVID-19: a systematic review and meta-analysis
An excerpt from NY Times article:
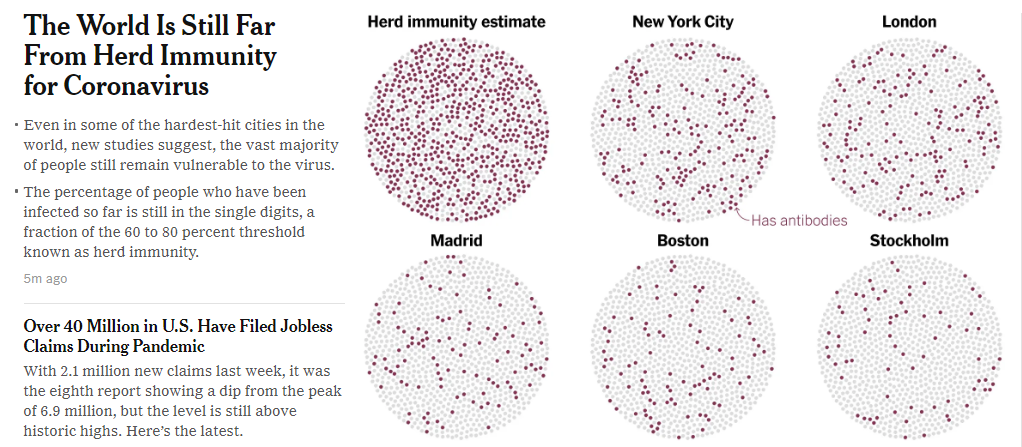
The surgical masks used in risky settings like hospitals offer much less protection against the coronavirus, an analysis found…
The results, published on Monday in The Lancet, make it clear that the W.H.O. and the Centers for Disease Control and Prevention should recommend that essential workers like nurses and emergency responders wear N95 masks, not just surgical masks
N95 masks offered 96 percent protection, the analysis found, while the figure for surgical masks was 77 percent. The findings are particularly important as the United States moves to reopen the economy, Dr. Michaels said…
Workers in health care settings are not the only ones at high risk of coronavirus infection: employees in meatpacking plants and some farms are all also at high risk of coronavirus infection and could benefit from N95 masks..
The new analysis also suggests that covering the eyes with face shields, goggles and glasses may provide additional safeguards for health care workers and people in the community.
Related blog posts:
- @Atul_Gawande: How to Reopen
- How to Protect Healthcare Workers from COVID-19: Lessons from Hong Kong and Singapore
- Nationwide Coronavirus Data Skewed & More on Masks | gutsandgrowth
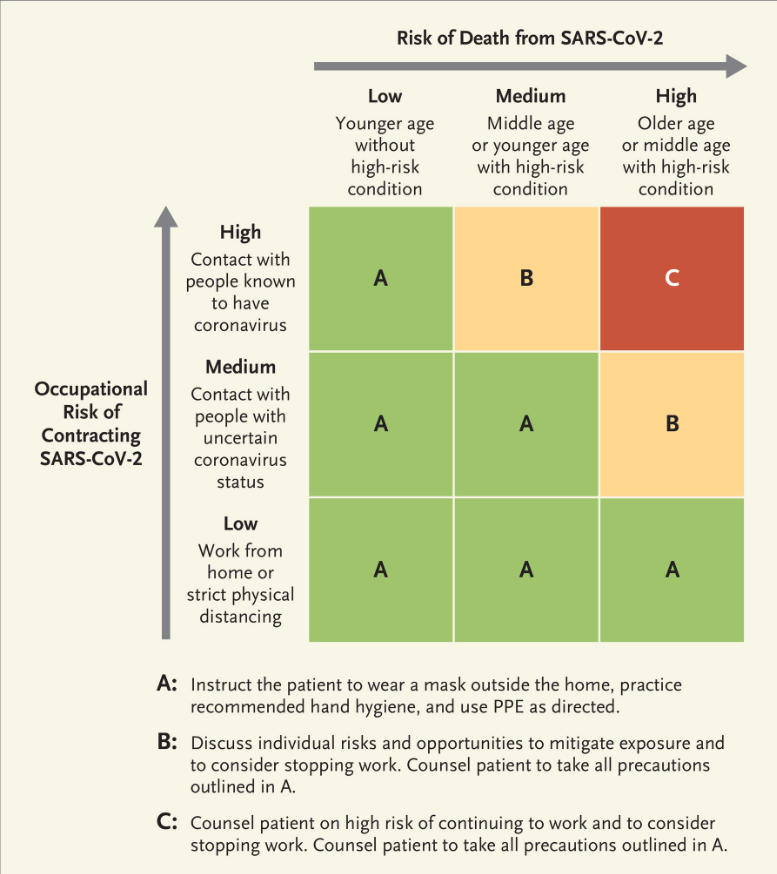
- Is It Safe for Me to Go to Work? | gutsandgrowth
- COVID-19 Posts