A recent study (JA Silvester et al. Gastroenterol 2020; 158: 1497-99) examined the diet of 18 participants with celiac disease who endorsed no intentional gluten ingestion.
From BeyondCeliac website: CELIAC DISEASE RESEARCHERS EXAMINE THE CONTENT OF PATIENTS’ DOGGIE BAGS
There are two ways you could interpret the name of the new Doggie Bag study, which investigates how much gluten people with celiac disease are getting in their diets. And each would be correct.
Participants in the study provided portions of all the food they ate over 10 days – what you could think of as the doggie bag you bring home from a restaurant. They also provided stool samples, which might bring to mind the bags dog owners use to clean up after their pets.
Either way, the name reflects the commitment made by 18 celiac disease patients on the gluten-free diet who took part in the 10-day review of all the gluten going in and coming out of their bodies. Urine samples were also collected.
Celiac disease researchers tested all the samples for the presence of gluten immunogenic peptides (GIP) and concluded that 66 percent of the patients trying to follow a strict gluten-free diet showed evidence, by one measure or another, of being exposed to gluten. The amount of gluten varied from .23 milligrams (mg) to more that 40 mg with each exposure. Up to 10 mg of gluten per day is generally considered a safe level of gluten consumption for most people with celiac disease, according to the University of Chicago Celiac Disease Center.
Key findings:
- 25 of 313 (8%) of food samples from 9 participants had detectable gluten with a median of 11 parts per million
- 12 of 18 with good or excellent GFD adherence based on standardized self-report were exposed to gluten within the 10-day study period
- Among the 12 with gluten detected in their diet, 5 (42%) had abnormal TTG IgA antibody levels and 8 (66%) had Marsh 3A histology; in the 6 with no gluten detected, 2 (33%) had abnormal TTG IgA antibody levels and 2 (33%) had Marsh 3A histology
My take: For many patients with celiac disease, a “GFD may be more aspirational than achievable, even by highly committed and knowledgeable individuals.”
Related blog posts:
- #NASPGHAN19 Postgraduate Course (part 2)
- Celiac Disease: “”80 percent of success is just showing up”
- Improving Care Process in Celiac Disease
- Closer followup for Celiac disease & pediatric guidelines
- “Gluten-Related Disorders” (Part 1)
- Celiac Disease: “Ten Things That Every Gastroenterologist Should Know” | gutsandgrowth
- Oats OK for Celiac Disease
- How Slow Do Objective Markers of Celiac Change After Treatment? | gutsandgrowth
- Northern Latitudes –Higher Prevalence of Celiac in U.S.
- Celiac Disease Epidemic (High rate of celiac disease reported in Denver children)
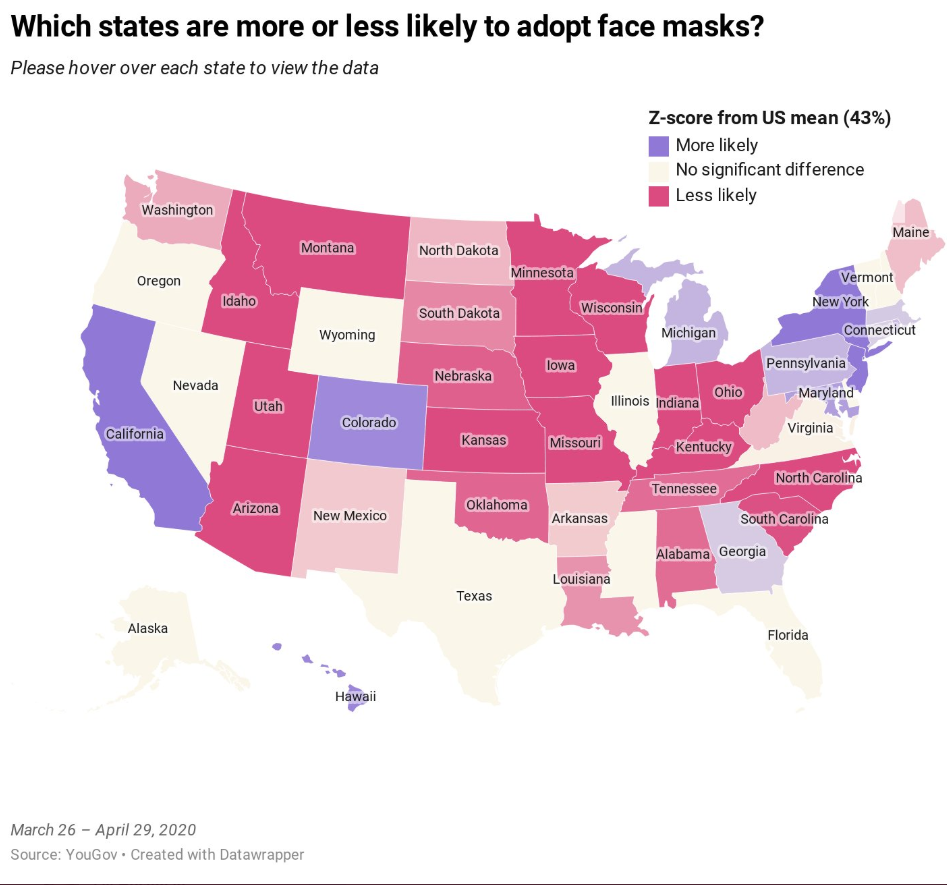
From YouGov survey: The states that are more and less likely to adopt face masks
- Methodology: The survey is based on the interviews of 89,347 US adults aged 18 and over between March 26-April 29, 2020. All interviews were conducted online and the results have been weighed to be nationally representative.
- During the course of April, the share of Americans who wore face masks while out in public surged from 17 percent at the start of the month to 63 percent by month’s end
- A state-by-state analysis reveals some states are significantly more likely to adopt face masks than others. Georgia was ahead of nationwide average during study period (45% compared to 43% nationwide)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition