Children’s Healthcare of Atlanta Hope & Will blog: Common Batteries Pose Danger For Kids

Related blog posts:

Children’s Healthcare of Atlanta Hope & Will blog: Common Batteries Pose Danger For Kids
Related blog posts:
With nonalcoholic fatty liver disease (NAFLD), it is well-documented that adverse cardiovascular events influence mortality more than any other factor. Dyslipidemia plays an important role in these outcomes.
A recent study (KE Harlow et al. J Pediatr 2018; article in press. DOI: https://doi.org/10.1016/j.jpeds.2018.02.038) indicates that “clinically actionable dyslipidemia” is present in more than half of pediatric patients with NAFLD.
This multicenter, longitudinal cohort study included children (n=585) with NAFLD enrolled in the National Institute of Diabetes and Digestive and Kidney Diseases Nonalcoholic Steatohepatitis Clinical Research Network.
Key findings:
My take: Assessing/managing dyslipidemia is an important component of NAFLD care.
Link to abstract: Clinically Actionable Hypercholesterolemia and Hypertriglyceridemia in Children with Nonalcoholic Fatty Liver Disease
Related blog posts:

Two interesting commentaries on the saline shortages:
The first explains that large quantities of saline bags are needed each month –more than 40 million bags per month! While saline is inexpensive, the production requires meticulous care to avoid contamination and there have been supply issues since 2014, prior to Hurricane Maria. However, the problem has been much worse since Hurricane Maria which damaged Puerto Rico. Puerto Rico supplies 44% of the IV bags in the U.S. These fluids are given to virtually all hospitalized patients, either for IV fluids or as a component with medications/flushes.
Other points:
The article by Patino et al provides Brigham and Women’s Hospital Oral Rehydration protocol. Key points:
Another study (SP Paul et al. JPGN 2018; 66: 641-44) has shown that high anti-TTG IgA levels are reliable in establishing the diagnosis of celiac disease in asymptomatic children from high-risk groups. In this study with prospectively-collected data from 2007-2017, 84 of 157 children had anti-TTG titers >10x ULN. 75 of these 84 were from high-risk groups, mainly type 1 diabetes (36), and first degree relatives (24)
Key finding:
Related blog posts:
Related study: R Mandile et al. JPGN 2018; 66: 654-56. This prospective study showed that 19 of 35 (54%) patients with potential celiac disease had a complete clinical response on a gluten-free diet to symptoms like abdominal pain and diarrhea. Thus, in many patients with potential celiac disease, a gluten-free diet will not be effective.
Related blog posts:
Everyday parents ask me if Miralax (polyethylene glycol) is safe; this has been driven by social media claims of neurotoxicity and by articles in the NY Times (see prior blog references) indicating that more testing is needed.
A recent study (KC Williams et al. J Pediatr 2018; 195: 148-53) examines one of the areas of concern, whether miralax could result in toxic levels of glycols. In this study with 9 treated children (ages 6-12 years) and 18 controls, careful study of potentially toxic agents, ethylene glycol (EG), diethylene glycol (DEG), and triethylene glycol (TEG), were measured every 30 minutes for 3 hours after receiving 17 g of PEG 3350.
Key findings:
With regard to TEG toxicity, in the discussion, the authors note that, based on animal studies, “very large doses of TEG are needed to cause side effects.” Even doses of 4000 mg/kg of TEG daily for 90 days did not result in local or systemic toxicity. The authors note that TEG concentration in PEG 3350 is “approximately 22.1-30.6 mcg per 17 gram dose of PEG 3350.”
With regard to EG and DEG, “the average EG and DEG content of the PEG samples in this study were a 100 and 800 times less, respectively, than this required 0.2% cutoff” [FDA limit]. The agency of Toxic Substances and Disease Registry profile for EG, has indicated that “EG blood levels greater tan 0.2 mg/mL are needed for acute toxic poisoning. The average level of EG at the 90-minute peak of 1100 +/- 350 ng/mL was 182 times lower than this level.” For chronic exposure EG toxicity, the authors estimate that one would need to take “40 capfuls [17 gram each] of PEG 3350 per day for up to a year.” The EPA also has advisories with regard to EG. To achieve toxic levels for a 10-kg child, this would necessitate that the child “would have to drink 1 L of water with 50 capfuls (858 g) in 1 day or 15 capfuls (258 g) per day for 10 days.”
An important limitation of this study is that there may be other metabolites that are not measured that could cause neurotoxicity.
My take: This study shows that the theoretical risk of glycol toxicity is highly unlikely. My advice for miralax usage: (borrowed from expert review): “Generally speaking, if your child has been prescribed PEG 3350 as part of his/her treatment plan, and you feel this medicine provides benefit, you should feel safe continuing PEG 3350. At this time, PEG 3350 appears to be safe based on current medical literature. We recommend discussing any concerns you have about the safety of PEG 3350 with your child’s health care provider. If you would prefer for your child to stop taking PEG 3350, discuss other treatments options with your child’s health care team before stopping PEG 3350 therapy. Although abruptly stopping PEG 3350 is not considered dangerous, it could lead to a relapse/worsening of constipation.”
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Related blog posts:

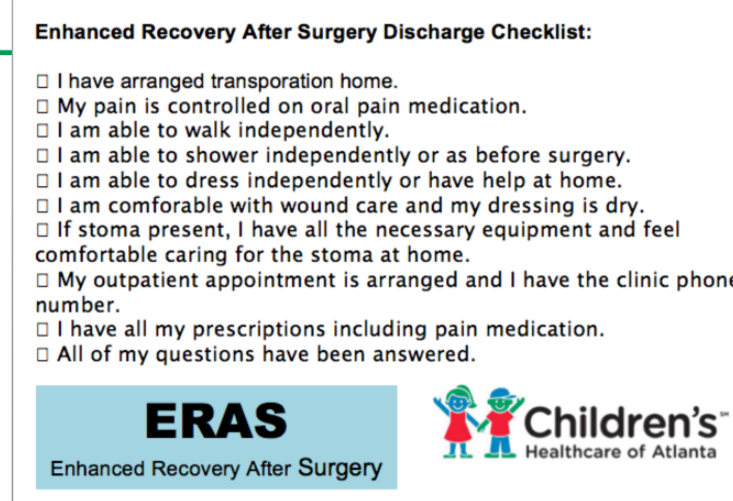
At a recent ImproveCareNow population management meeting for our group, Dr. Kurt Heiss provided an update on the expanding use of ERAS. In addition to colorectal surgery, uses at our hospital system have included bariatric surgery, craniofacial surgery, and umbilical hernia repairs. The results of this bundled care show fewer complications, less pain/less narcotics (more blocks), and shorter hospital stays (without increased readmission rates).
For those who are not as familiar as they would like (and for patients), I recommend a 7 minute Lego ERAS YouTube link: LEGO Surgery -Enhanced Recovery After Surgery
Related blog post: ERAS -Enhanced Recovery After Surgery (2016) With full slide set explaining ERAS further



A recent retrospective single-center study (J Satkunasingham et al. Liver Transplantation 2018; 24: 470-77) shows that MRI is a good tool to assess hepatic steatosis. In total there were 144 liver donor candidates; a subset of 32 underwent liver biopsy.
When examining magnetic resonance spectroscopy (MRS) and MRI -proton pump density fat fraction (PDFF), the authors found that MRS-PDFF and MRI-PDFF had 95% and 100% negative predictive value in identifying patients with clinically significant histologic steatosis (≥10%).
The associated editorial by James Trotter (pg 457-58) makes several important points:
My take (borrowed from editorial): “Noninvasive estimation of hepatic steatosis is sufficiently accurate to forgo liver biopsy in most donors, although ultimately this decision will continue to rest with the individual center.”

A recent retrospective study (NE Burr et al. Clin Gastroenterol Hepatol 2018; 16: 534-41) with 3517 patient’s with Crohn’s disease (CD) and 5349 with ulcerative colitis (UC) examined the frequency of opioid prescriptions and the relationship to fatal outcomes.
Key findings:
This study is in agreement with other data showing increasing use of opiate prescriptions worldwide for chronic noncancer pain (although there has been a drop in the past year). As with other studies of patients with inflammatory bowel disease, this study shows an association between opioid use and mortality.
My take: Needing an opioid may be a marker for more severe disease. Whether the opioid use directly contributes to mortality remains unclear.

A survey (O Waisbourd-Zinman, et al. JPGN 2018; 66: 447-49) of 44 pediatric hepatologists (with 935 years of clinical practice) examined the issue of splenic rupture and spleen guards. ~90% of those surveyed reported following at least 30 patients with portal hypertension and splenomegaly.
While I did not participate in this survey, the one patient with chronic liver disease that I followed who had a splenic rupture had fallen down a flight of steps; fortunately, he recovered with supportive care.
My take: This survey shows that there is wide variability in the use of spleen guards. In almost all cases of splenic rupture, this was precipitated by severe trauma. Though, patients with portal hypertension may avoid high contact sports and thus the risks are for these sports is unclear.
Related blog post:

Foggy Morning in Sandy Springs
Full Text Link: ACG Clinical Guideline: Management of Crohn’s Disease. GR Lichtenstein et al. Am J Gastroenterol 2018; 113:481–517
A few of the recommendations from Table 1:
From Table 2:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

