I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Yesterday, a ICU colleague indicated that she really does not like to work on summer holiday weekends. While she is a hard worker, what she doesn’t like is seeing kids with drowning and firework injuries. All of a sudden a happy time becomes tragic. With that in mind, here are a few tips to prevent drowning.
Also, firearm deaths are the leading cause of death in children in the U.S. and motor vehicle accidents are second. So, firearms need to be secured and drive safely on the way to the pool, lake, river or beach.
CP Duggan, ZA Bhutta. NEJM 2025; DOI: 10.1056/NEJMp2503243. “Putting America First” — Undermining Health for Populations at Home and Abroad
This article initially lays out the historical context of U.S. involvement in global health dating back to aiding famine in Belgium (1917), WHO (1948), USAID (1961). Also, the CDC and NIH have played important roles following WWII. Subsequently, the commentary outlines the impact of dismantling U.S global health efforts. In the two related articles cited afterwards, it is clear that the cuts to foreign aid and other DOGE activities may result in millions of deaths and at the same time expand the federal deficit.
An excerpt:
In the initial months of the Trump administration, numerous executive orders have led to a chaotic dismantling of U.S. foreign-assistance and global health efforts. These orders have already had, and will continue to have, severe adverse effects on vulnerable populations globally. But they also have serious implications for people in the United States…
Often missing from these success stories are the financial and health-related benefits these programs have had in the United States….One of the earliest and most fundamental examples of reciprocal innovation was the discovery and implementation of oral rehydration therapy (ORT)…Widespread use of ORT has helped drive substantial reductions in childhood deaths from diarrhea and has led to a new standard of care for childhood diarrhea in high-income countries and to commercial products in the United States…
Perhaps no program epitomizes these dual advantages better than the President’s Emergency Plan for AIDS Relief (PEPFAR). Early in the HIV epidemic, the NIH promoted multinational scientific collaborations to identify the virus, develop effective treatments, and implement global prevention and treatment programs, which led to PEPFAR’s creation in 2003. PEPFAR has saved 26 million lives, and economic growth in countries with PEPFAR programs has benefited the United States and other trading partners…[and] have contributed enormously to current knowledge about HIV and AIDS.
Another essential initiative, the FIC — the NIH institute responsible for supporting research training and partnerships in global health — has …directly benefited health in the United States by advancing early cancer detection and the development of sickle cell disease therapies, point-of-care diagnostics for infectious diseases, and treatments for child malnutrition. More than three quarters of FIC grants involve a U.S. grantee or investigator, which further emphasizes the institute’s direct benefits to the U.S. economy…
Since U.S. foreign assistance accounts for about 1% of the federal budget, we are skeptical of cost-savings–based arguments for its elimination…
The Trump administration’s gutting of USAID and other foreign-assistance programs marks a break from decades of evidence-based practices that have improved lives throughout the world. In addition to pushing millions of people into poverty and leading to an estimated 160,000 or more avoidable child deaths each year,4 these reforms will undermine health and the economy in the United States…
Withdrawal from the WHO reduces the United States’ ability to influence reform and restructuring of the world’s global health coordinating body. The elimination of U.S. funding for Gavi, the Vaccine Alliance, also endangers the health of vulnerable populations internationally and in the United States…
Critical to the success of advocacy efforts will be evidence of the ways in which the withdrawal of foreign aid and global disengagement undermine health and economic well-being in the United States and threaten global health and economic security.
My take: By the time the extent of the damage is understood, it will be too late to fix what this administration has destroyed. The toll in terms of death and suffering both in the U.S. and abroad will be hard to justify and not further the aim of making ‘America First.’
Related articles:
D Wallace-Wells, NY Times 5/8/25: The $200 Billion Gamble: Bill Gates’s Plan to Wind Down His Foundation “He is committing the foundation to 20 more years of generous aid, more than $200 billion in total, targeting health and human development…The news comes at a time that will seem to many as a perilous one, given the Trump administration’s recent assault on foreign aid and indeed on the idea of global generosity itself….The journal Nature suggested that an overall cessation of U.S. aid funding could result in roughly 25 million additional deaths over 15 years.”
J Riedl, The Atlantic 5/8/25: The Actual Math Behind DOGE’s Cuts “As an effort to meaningfully reduce federal spending, however, DOGE remains wholly unserious…The DOGE website now claims $165 billion in savings. However, it still details only a fraction of the supposed cuts, and earlier accounting errors have given way to new ones…Even assuming that the website’s stated savings have become twice as accurate as they were in February, annual savings would reach perhaps $15 billion, or 0.2 percent of federal spending…Total federal outlays in February and March were $86 billion (or 7 percent) higher than the levels from the same months a year ago, when adjusted for timing shifts. This spending growth—approximately $500 billion at an annualized rate—continues to be driven by the three-quarters of federal spending allocated to Social Security, Medicare, Medicaid, defense, veterans’ benefits, and interest costs. These massive expenses have been untouched by DOGE’s focus on small but controversial targets such as DEI contracts and Politico subscriptions…The bad news is that the project seems quite likely to expand long-term budget deficits. Slashing IRS enforcement will embolden tax evasion and reduce revenues by hundreds of billions of dollars over the decade. Laying off Department of Education employees who ensure collection of student-loan repayments will increase the deficit. Illegally terminated federal employees are already being reinstated with full back pay, leaving the government with little to show for its trouble besides mounting legal fees…None of this is to say that DOGE has failed. Musk might not have followed through on his unfocused and evolving promises to eliminate payment errors, balance the entire budget, and implement regulatory reform. But he has successfully given the White House cover to purge and intimidate the civil service, helped Congress justify exorbitant tax cuts, rewarded MAGA voters with revenge against their perceived enemies, and granted himself the ability to access sensitive government data and possibly ensure his companies’ continued government contracts. Sure, annual budget deficits remain on track to double over the next decade. But if you thought DOGE was really about cutting costs, you were never in on the joke.”
View of the Chattahoochee River from Don While Memorial Park, Sandy Springs, Ga
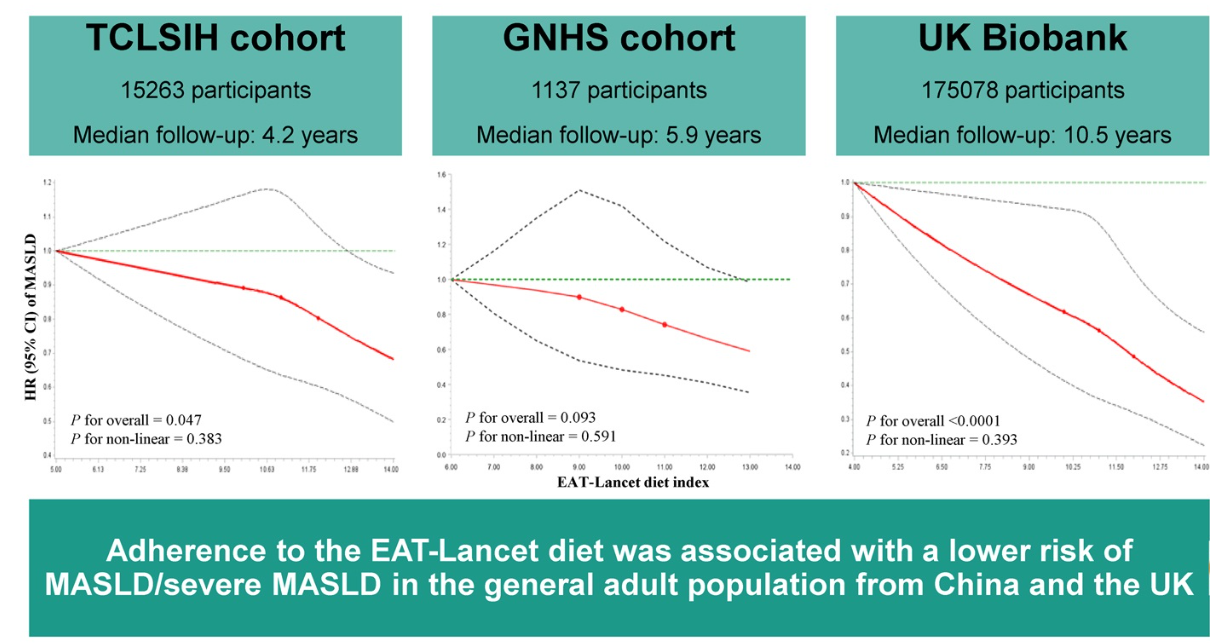
From the commentary: “In 2019, the EAT-Lancet Commission on Food, Plant, and Health proposed a planetary health diet, known as the EAT-Lancet reference diet, that promotes human health and sustainable food production globally…and recommends fruits, vegetables, whole grains, plant-based proteins (eg. legumes, nuts) and unsaturated plant oils, with limited or moderate amounts of animal-based proteins such as meat and dairy….[it] has been associated with multiple health benefits, including reducing the risks of type 2 diabetes, cardiovascular disease, certain cancers, and all-cause mortality.”
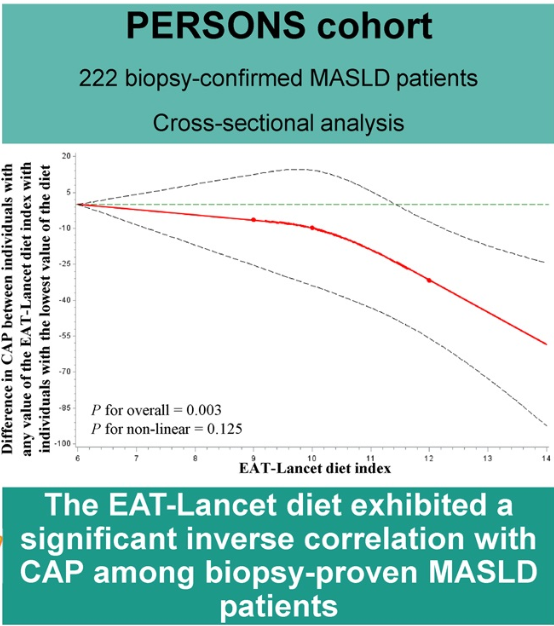
Methods: This prospective multicohort study comprised more than 191,000 adults from several cohorts. In addition, 228 Chinese adults from the Prospective Epidemic Research Specifically of Non-alcoholic Steatohepatitis (PERSONS) with biopsy-proven MASLD were included.
Key findings:
Participants in the highest tertiles of the EAT-Lancet diet index had a lower risk of MASLD compared with those in the lowest tertiles with HR ranging in different cohorts from 0.73 to 0.87
Liver-controlled attenuation parameter decreased with increasing the diet index in individuals with biopsy-proven MASLD (β = −5.895
My take (borrowed from the authors): Adherence to the EAT-Lancet reference diet was inversely associated with the risk of MASLD as well as its severity.
This case report of four patients provides a good review of metastatic Crohn’s disease (MCD). MCD indicates that there is noncontiguous dermatological spread of CD involving the genitalia and perineum.
Key points:
“Less than 100 cases of pediatric MCD have been reported in the literature to date. These lesions are characterized by swelling, plaques, nodules, fissures, ulcerations, or crusts. In children, MCD typically presents as genital swelling with or without erythema in approximately 85% of cases.”
“Prior studies have shown that MCD co-occurs with CD in 50.8% of children, while others may develop GI symptoms after MCD diagnosis (15.3%) or even lack signs of CD (11.9%).”
“Scrotal histopathology revealed granulomatous inflammation, and genetic testing identified pathogenic variants in NOD2, COL7A1, and Chek2, as well as additional variants of uncertain significance.”
The optimal treatment is not clear. “Prior case reports and case series have shown positive responses to TNF-α inhibitors, but relapses may be common. Similarly, only partial improvement was noted in our patients treated with infliximab and adalimumab.”
Discussion: “Many patients do not demonstrate GI symptoms and may experience significant delays in diagnosis.”
My take: This article provides a good review of metastatic Crohn’s disease which is a rare problem. I have had two patients with this disorder. This problem fits the adage of “the more you see, the more you know; and, the more you know, the more you see.”
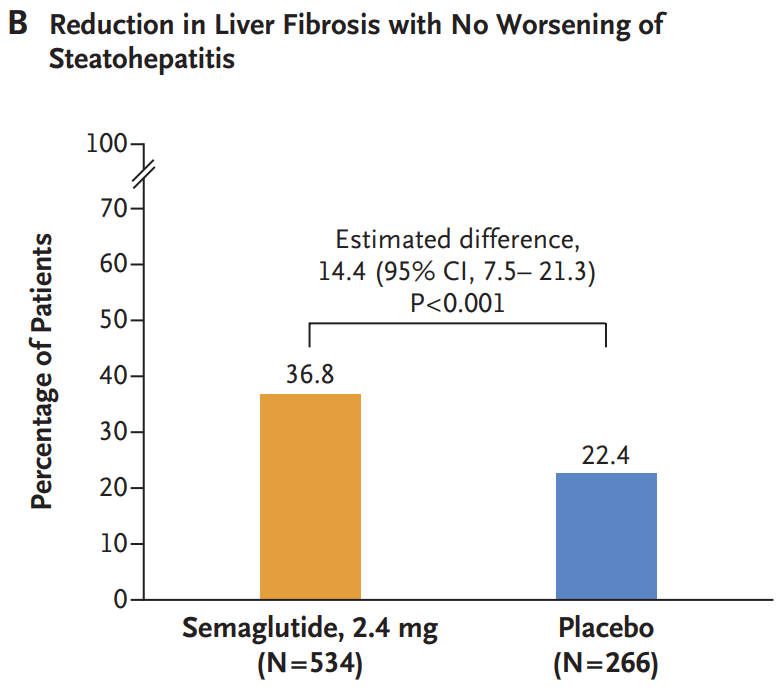
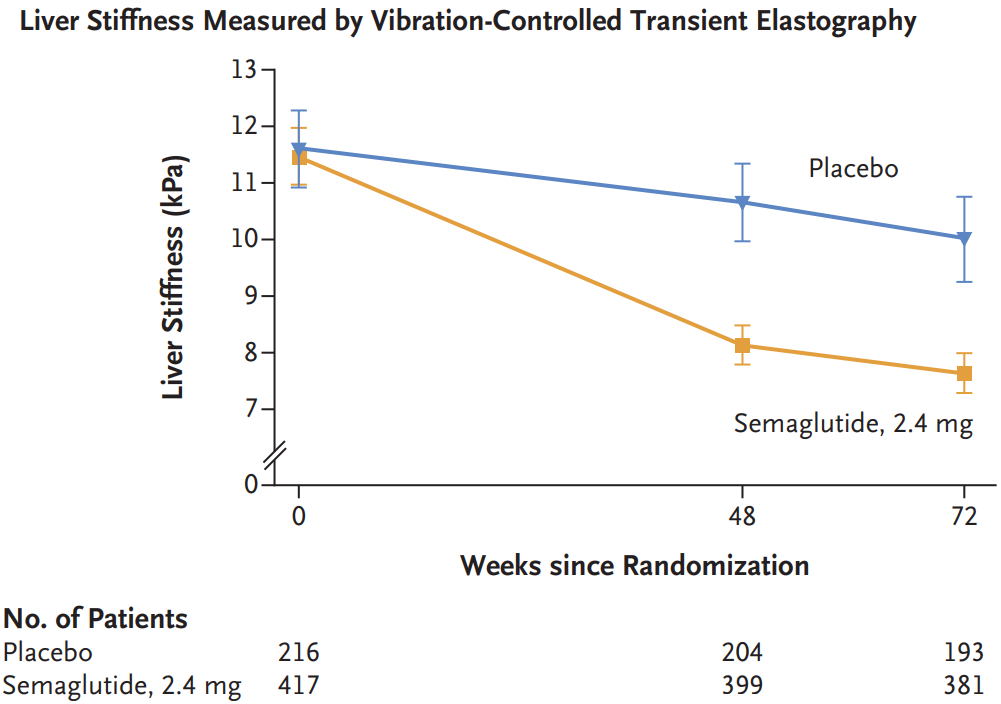
Methods: In this phase 3, multicenter, randomized, double-blind, placebo-controlled trial, the authors assigned 1197 patients with biopsy-defined MASH and fibrosis stage 2 or 3 in a 2:1 ratio to receive once-weekly subcutaneous semaglutide at a dose of 2.4 mg or placebo for 240 weeks
Key findings:
Resolution of steatohepatitis without worsening of fibrosis occurred in 62.9% of the 534 patients in the semaglutide group and in 34.3% of the 266 patients in the placebo group (P<0.001)
A reduction in liver fibrosis without worsening of steatohepatitis was reported in 36.8% of the patients in the semaglutide group and in 22.4% of those in the placebo group (P<0.001).
The mean change in body weight was −10.5% with semaglutide and −2.0% with placebo (P<0.001)
Gastrointestinal adverse events were more common in the semaglutide group. The incidence of acute pancreatitis was similar in the two groups: Nausea 290/800 (36.2%) vs. 52/395 (13.2%), Diarrhea 215/800 (26.9%) vs. 48/395 (12.2%), Constipation 178/800 (22.2%) vs. 33/395 (8.4%) and Vomiting 149/800 (18.6%) vs. 22/395 (5.6%)
Semaglutide improved multiple cardiometabolic features, including glycemic control and insulin resistance. “These findings are important because metabolic dysfunction is an upstream event driving hepatic lipotoxicity and, subsequently, steatohepatitis and fibrogenesis. Thus, semaglutide treatment addressed the primary pathogenic driver of MASH”
Side effects leading to people dropping out of the trial were 2.6% for the semaglutide group and 3.3% for the placebo group
Discussion notes that “although semaglutide can be safely used in patients with cirrhosis, its efficacy in this population has not been established.”
My take: Semaglutide appears to be effective in patients with MASH.with stage 2 or 3 fibrosis.
Background: “Caution regarding live vaccine administration emerged following reports of 5 fatal outcomes following the administration of the Bacille Calmette-Guérin vaccine in biologic-exposed infants.9 This has resulted in gastroenterology guidelines recommending that biologic-exposed infants should avoid live vaccines within the first 6 to 12 months of life or until drug concentrations are no longer detectable in the infant’s blood to reduce potential risks.2,10 [J Crohns Colitis. 2023; 17:1-27, Gastroenterology. 2021; 161:669-680.e0]. Contrary to this, inadvertent administration of the live oral rotavirus vaccine in biologic-exposed individuals has not been associated with significant adverse effects.7,11 Withholding the rotavirus vaccine has implications, given that rotavirus infection in infants is a leading cause of severe, dehydrating diarrhea in children under the age of 5 years globally.12,13“
This prospective cohort study enrolled 57 biologic-exposed infants, including infliximab (n = 21), adalimumab (n = 19), vedolizumab (n = 10), and ustekinumab (n = 7), in the third trimester.
Key findings:
Immunologic assessments validated for age were normal in all infants despite median infliximab concentrations of 6.1 ug/mL, adalimumab concentrations of 1.7 ug/mL, ustekinumab concentrations of 0.6 ug/mL, and undetectable for vedolizumab at median of 10.7 weeks of age
The live oral rotavirus vaccine series was provided to 50 infants with the first dose given at a median of 13 weeks of age. No adverse effects following immunization were reported
Discussion:
“Administration of the live rotavirus vaccine appeared low-risk in biologic-exposed infants born to mothers with IBD”
“Routine drug concentration testing in the infant should not be utilized to determine the safety of live rotavirus vaccination”
“Physicians should advise patients to ‘be more concerned about active disease rather than active medications’ and to continue effective therapy through pregnancy and lactation”
My take: Given the difficulty in excluding rare adverse outcomes, it is unlikely that formal vaccine recommendations will change in infants exposed to biologics; however, inadvertent administration of a live oral rotavirus vaccine poses a very lowl risk based on current studies.
Floating flowers -seen in several places in Thailand
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Methods: Here we characterize the trajectory by which the gut microbiome recovers its taxonomic and functional profile after antibiotic treatment in mice on regular chow (RC) or Western Diet (WD).
Key findings: “Only mice on RC undergo a rapid successional process of recovery. Metabolic modelling indicates that a RC diet promotes the development of syntrophic cross-feeding interactions, whereas in mice on WD, a dominant taxon monopolizes readily available resources without releasing syntrophic byproducts. Intervention experiments reveal that an appropriate dietary resource environment is both necessary and sufficient for rapid and robust microbiome recovery, whereas microbial transplant is neither.”
Conclusion (from authors): “Our data challenge widespread enthusiasm for faecal microbiota transplant (FMT) as a strategy to address dysbiosis, and demonstrate that specific dietary interventions are, at a minimum, an essential prerequisite for effective FMT, and may afford a safer, more natural and less invasive alternative.”
My take: This study suggests that the best way to get a “healthy” microbiome is to eat a healthy diet rather than to try to alter with FMT. This finding likely would be the same for probiotics as well.
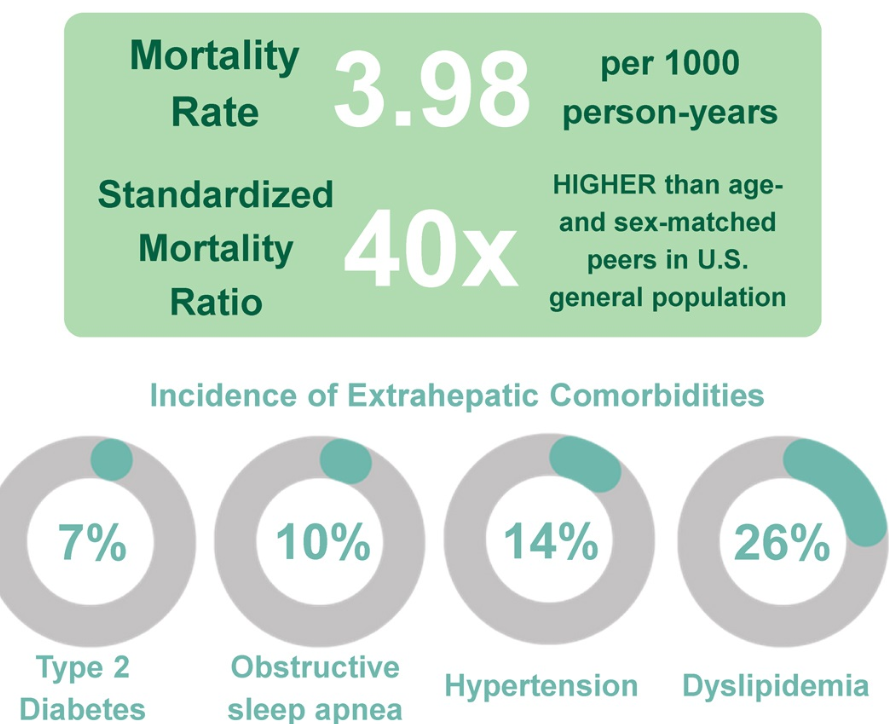
The findings, published April 22, 2025 in Hepatology, the scientific journal of the American Association for the Study of Liver Diseases, come from the Longitudinal InVestigation Evaluating Results of Steatosis (LIVERS) study, which followed 1,096 children over an average of 8.5 years. Nearly half of all deaths in the cohort were liver-related, and the overall mortality rate was 40 times higher than that of similar peers in the general U.S. population...
The retrospective cohort study used medical records and National Death Index data to follow children ages 2 to 18 who were diagnosed with MASLD between 2000 and 2017. Over an average of 8.5 years of follow-up, 3.4% of children had died…
In addition to the risk of early death, many children in the study developed serious health problems while still in their teens or twenties. These included high blood pressure (14%), obstructive sleep apnea (9.5%) and type 2 diabetes (7.3%). Problems with blood fats, such as high triglycerides or low HDL, were even more common — making dyslipidemia, the presence of abnormal levels of fats (lipids) in the blood, the most frequent complication overall.
My take: Since this was a retrospective single center study, the severity of the findings may be different with a more-representative national cohort. Nevertheless, this study shows that MASLD has serious consequences including premature death and numerous comorbidities.
Researchers recruited 10 couples, each with one partner who has celiac disease, for a two-part study. In each session, the non-celiac partner ate 10 saltine crackers, and then the couple kissed for 10 seconds. In one session, the partners waited five minutes before the kiss, and in the other, they drank 4 ounces of water before kissing…
Although gluten was still found in saliva after kissing a partner who had consumed gluten and then had a glass of water, in all cases the amount was less than 20 parts per million, the level allowed in gluten-free products, which is considered safe.
“Patients with celiac disease can be more relaxed, knowing that the risk of gluten cross-contact through kissing a partner who has consumed gluten can be brought down to safe levels if food is followed by a small glass of water.”
From NBC article:
In the first scenario — waiting five minutes before kissing — two of the celiac participants had more than 20 parts per million of gluten in their saliva sample.
In the scenario in which non-celiac partners drank 4 ounces of water before the kiss, everyone’s saliva tests contained fewer than 20 ppm of gluten.
My take: Sounds like a fun study. Best to drink water before kissing your partner who has celiac disease.
Reference: Anne Lee. DDW Abstract Mo1242, 5/5/25: “Assessing gluten transfer via kissing; a prospective study of celiac-discordant couples”
This was a cross-sectional study of newly diagnosed pediatric patients (n=869) with IBD at 22 United States sites from 2019 to 2022. 57% were diagnosed with CD, 34% with UC, and 4% with IBD-U.
Key findings:
Overall, the mean time from symptom onset to diagnosis was 265.9 days
Factors associated with longer diagnosis time included CD vs UC (odds ratio [OR], 2.6), and longer travel time to clinic (>1 hour [OR, 1.7], >2 hours [OR, 1.8] each vs <30 minutes)
There was no association with race, ethnicity, birth country, gender, parent education, household income, insurance type, health literacy, and health system distrust
The finding that there is a longer diagnostic delay with CD than UC is consistent with prior studies. The longer travel time has not been widely recognized as a factor associated with delayed diagnosis, though it has been associated with other negative outcomes like higher mortality with chronic liver disease.
Regarding the lack of a negative impact from factors like race/ethnicity and income, my suspicion is that this is probably related to several factors:
Overall, the pediatric age group has a very high rate of being insured as most children without commercial insurance currently qualify for Medicaid. This helps improve access to needed/timely health care