
NY Times 8/17/23, Nicholas Kristof: How Do We Fix the Scandal That Is American Health Care?
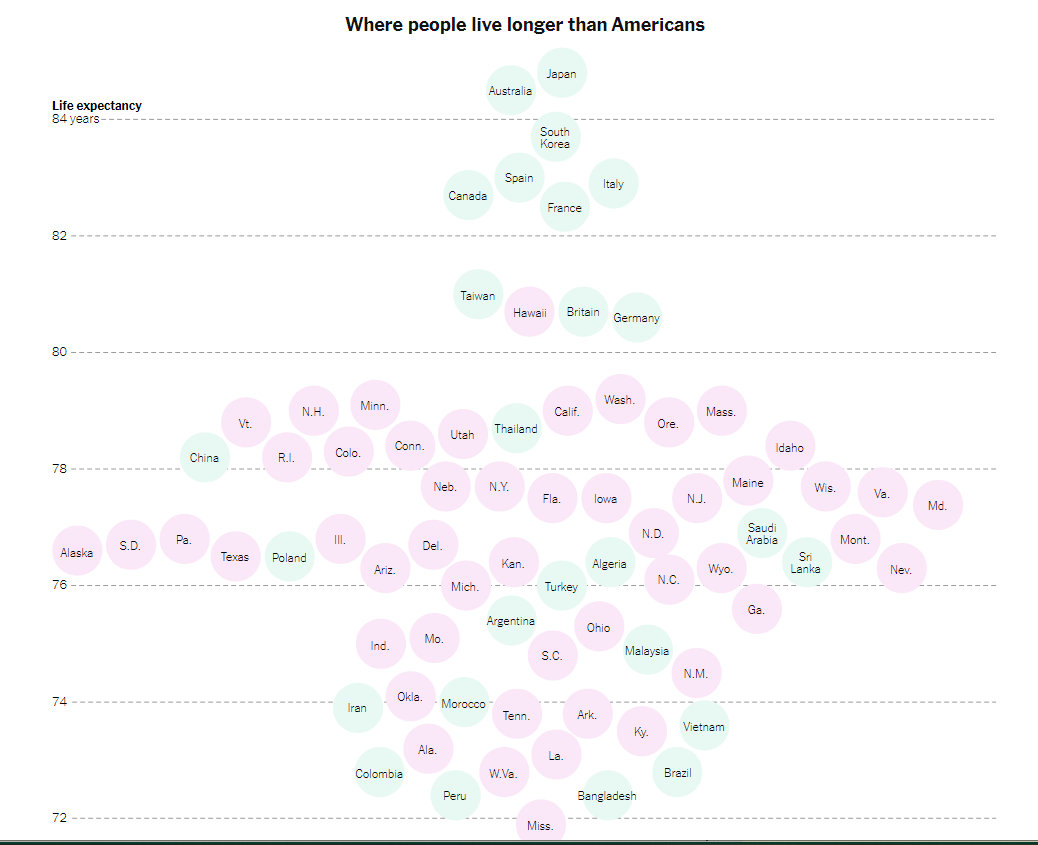
“It’s not just that life expectancy in Mississippi (71.9) now appears to be a hair shorter than in Bangladesh (72.4). Nor that an infant is some 70 percent more likely to die in the United States than in other wealthy countries….
All that is tragic and infuriating, but to me the most heart-rending symbol of America’s failure in health care is the avoidable amputations that result from poorly managed diabetes…A toe, foot or leg is cut off by a doctor about 150,000 times a year in America, making the United States a world leader of these amputations.
America’s dismal health care outcomes are a disgrace. They shame us. Partly because of diabetes and other preventable conditions, Americans suffer unnecessarily and often die young. It is unconscionable that newborns in India, Rwanda and Venezuela have a longer life expectancy than Native American newborns (65) in the United States. And Native American males have a life expectancy of just 61.5 years — shorter than the overall life expectancy in Haiti.“
The article recommends
- Expanding Access to Health Care
- Work on improving health behaviors: “smoking, eating habits and exercise — affect life expectancy even more than access to health care”…
- Work on poverty and education: “America’s health dysfunction is rooted in a broader national dysfunction, including deep intergenerational poverty and despair. The medical system can efficiently amputate a foot, but an improvement in self-care of diabetes sometimes requires an injection of hope and improvements in education, job training, earnings and opportunity.”
Related blog posts:
- “More Than Half a Million Extra Deaths” Every Year In U.S.
- Life Expectancy Dropping in U.S.
- Zip Code or Genetic Code -which is more important for longevity?
- No Exaggeration: Too Many Children Are Dying in the U.S.
- Firearms: #1 Cause of Pediatric Deaths & Households with Guns =More Deaths
- Opioid Epidemic -Devastating Impact on Children (images and Link)
- Today’s Children in Crisis: YOYO
- “Crossing Lines” and Why Firearm Deaths are The Leading Cause of Death in Children
- “A Smarter Way to Reduce Gun Deaths” Plus Two
- Suicide Rate Up 33% in Last 20 Years & Can We Stop It?



















{kind=link}