Two phase 3 placebo-controlled trials with the immune modulator risankizumab demonstrated control of Crohn’s disease whether or not patients had previously received a biologic agent.
Rates of clinical remission at 12 weeks with the interleukin (IL)-23 inhibitor risankizumab (Skyrizi, AbbVie), were about 48% in patients without prior exposure to biologic therapy and more than 40% in those with prior exposure…
The two trials, ADVANCE and MOTIVATE were presented together at the 2021 Digestive Disease Week (abstract 775a)…
Only 12% of patients in the placebo group achieved endoscopic remission versus 40.3% of those on the 600-mg dose of risankizumab (P<0.001). [Rates of endoscopic remission were higher in the biologic-naive (50.5%)]
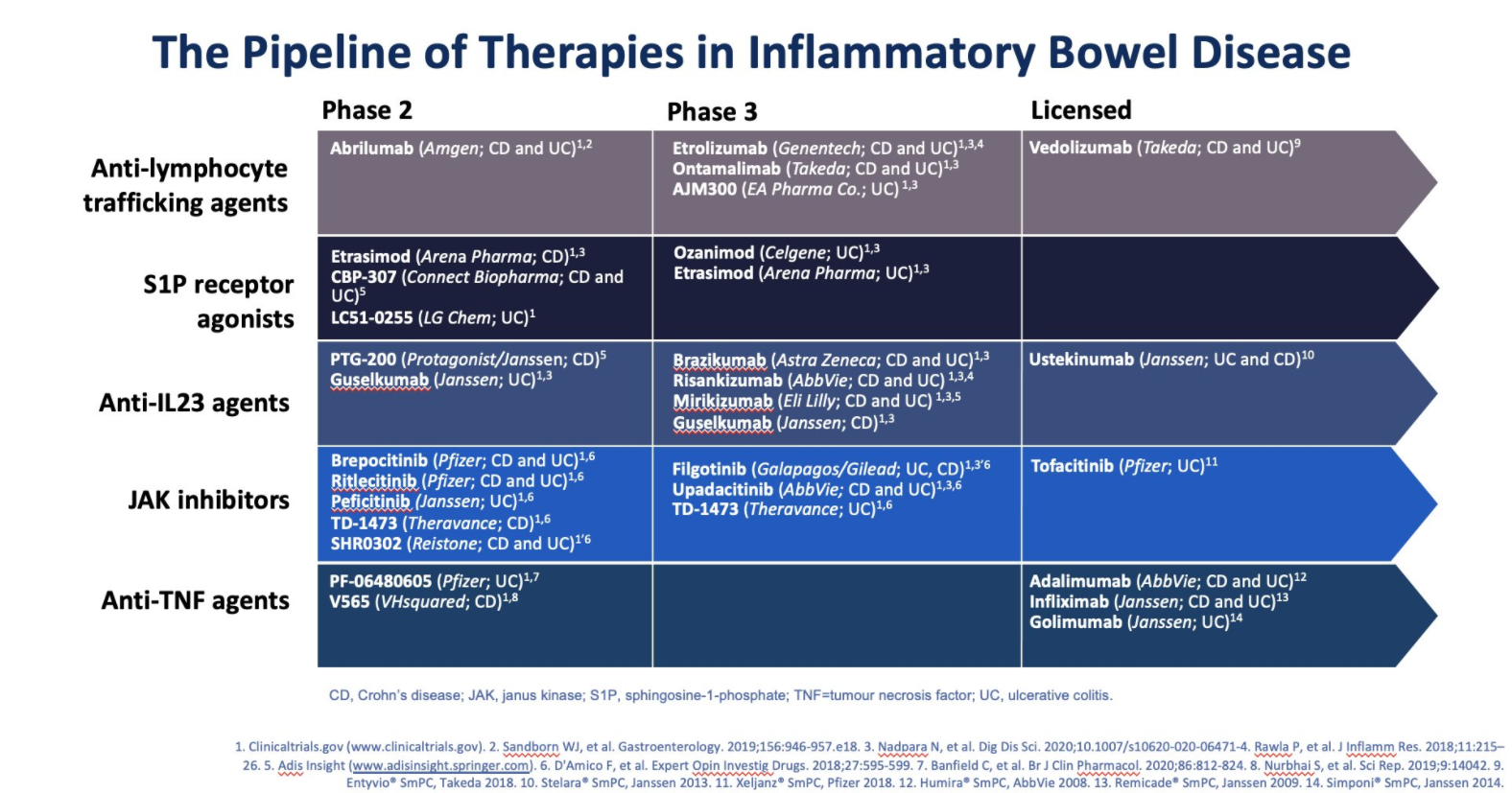
My take: In addition to ustekinumab (already approved), a number of other therapeutic agents that target IL-23 are likely to be available soon to help manage Crohn’s disease. This includes risankizumab but others with phase 3 studies include brazikumab, mirikizumab, and guselkumab..
Slide from David Rubin Twitter Feed (March 2021). Ozanimod now approved.
The first head-to-head trial comparing ustekinumab and adalimumab has found the two drugs are similarly safe and effective in patients with moderate to severe Crohn’s disease…
Dr. Scherl and her co-investigators in the SEAVUE trial randomly assigned 386 biologic-naive patients with Crohn’s disease to receive one year of treatment with either ustekinumab or adalimumab at standard on-label doses, with no dose escalation throughout the study period and no concomitant immunomodulators...
The findings, which were presented at the 2021 annual meeting of the European Crohn’s and Colitis Organisation (oral presentation OP02), showed that after one year of treatment, 65% of patients who received ustekinumab and 61% of those who received adalimumab achieved clinical remission, defined as a CDAI below 150...[And] similar additional outcomes, including clinical response at one year (72.3% for ustekinumab vs. 66.2% for adalimumab), corticosteroid-free remission at one year (60.7% vs. 57.4%, respectively), endoscopic remission at one year (28.5% vs. 30.7%)
My take: This study indicates that ustekinumab likely has similar safety and efficacy as adalimumab (though the study did not allow dose escalation or immunomodulators); thus, it could be positioned as a first-line treatment. It is administered less frequently as well.
Patrick Reeves passed along the following helpful information about the NASPGHAN toolbox:
The NASPGHAN Fellows committee, working in close partnership with the NASPGHAN Technology and Training committees, has developed an App named, “The NASPGHAN Toolbox”.
The App is equipped with ready access to: clinical calculators, guidelines and algorithms, medication guides, patient education resources, and more. You can access the Toolbox via its URL (https://toolbox.naspghan.org/) on your phone or computer.
The NASPGHAN team hopes this will enhance your day-to-day patient care of children with gastrointestinal disorders.
Some highlights:
Under scores/calculators: Paris Classification, PUCAI, PCDAI, Mayo Score, PELD, MELD
Methods: Twenty-eight patients corresponding to 29 SSTs (secretin stimulation tests) were performed on PPI, and 70 patients corresponding to 107 SSTs were performed off PPI.
Key findings:
Sensitivity, specificity, and PPV of SSTs on PPI were determined to be noninferior to SSTs off PPI (P ≤ 0.05 for all).
My take: Zollinger-Ellison is a rare consideration in pediatric gastroenterology (I have only seen one case in ~ 25 years of practice). However, if testing is needed, this article indicates that stopping PPIs is probably not needed.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Taft et al performed a retrospective study of 103 adult patients with eosinophilic esophagitis. Patients completed the following questionnaires immediately before to endoscopy:
Esophageal Hypervigilance and Anxiety Scale (EHAS)
Brief Esophageal Dysphagia Questionnaire (BEDQ)
Eosinophilic Esophagitis Symptom Activity Index (EEsAI)
Northwestern Esophageal Quality of Life Scale (NEQOL).
Endoscopic severity of EoE was graded using the EoE Endoscopic Reference Score System (EREFS). Dysphagia was the primary symptom in 73% of the patients.
Key findings:
Patient’s symptom severity (via EEsAI or BEDQ) did not correlate with histology (distal or proximal peak eosinophil count), endoscopic severity of the disease (EREFS), or the distensibility index (measured via functional lumen imaging probe)
Symptom severity was correlated with the Esophageal Hypervigilance and Anxiety Scale (EHAS)
There was no correlation between EHAS and histologic activity, endoscopic severity (EREFS), or the presence of a stricture
The associated commentary emphasizes some of the study limitations including taking surveys prior to endoscopy (increased anxiety).
My take: This study indicates that with eosinophilic esophagitis, similar to other organic diseases (eg. IBD), patient symptoms do not always correlate with disease severity, and addressing the impact of anxiety and hypervigilance is critical, especially in refractory symptoms.
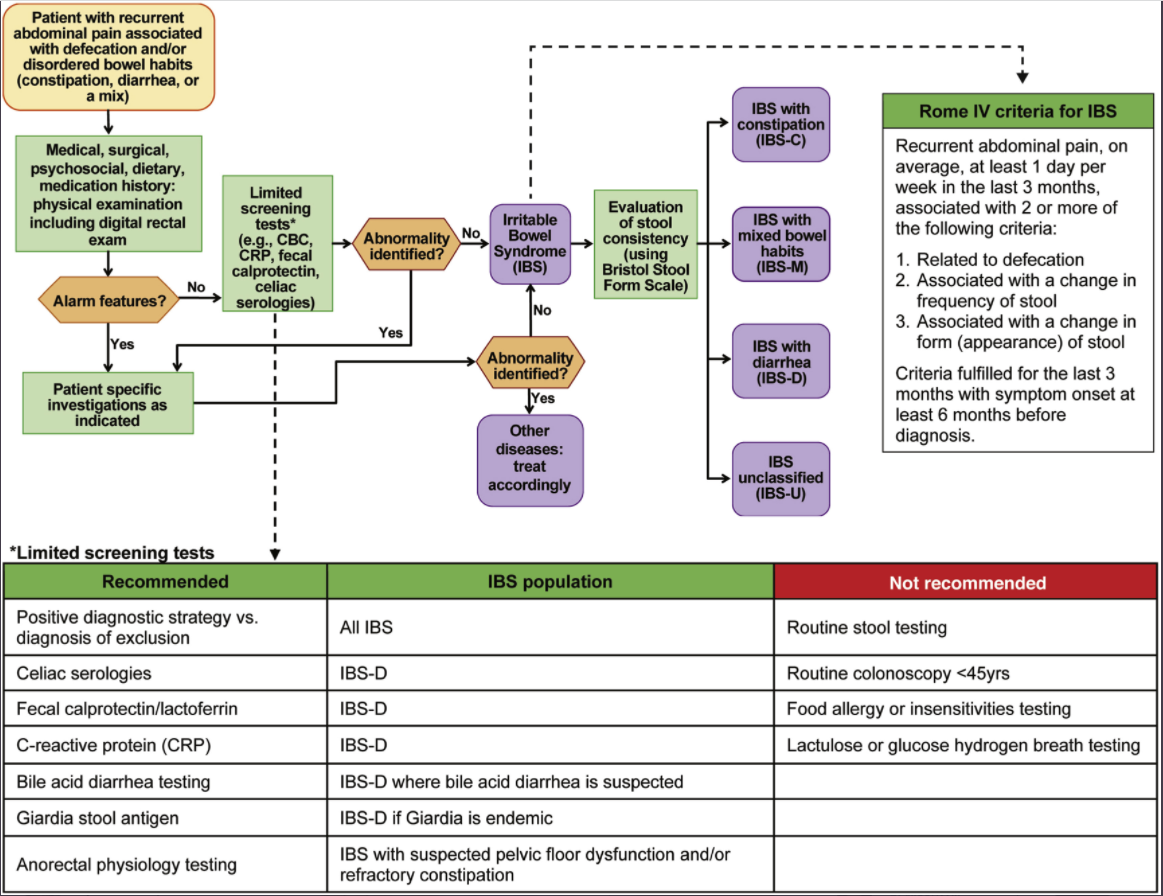
For a short article, this review provides a lot of practical advice. Challenges with IBS include the lack of objective biomarkers and “patients are often dissatisfied with a positive diagnostic approach or even after multiple negative tests.” The author recommends the following:
Confidently communicate the diagnosis of IBS
Explain visceral hypersensitivity and its associated with pain, and bloating and why central neuromodulators and behavioral therapy are often used. Explain that IBS can be associated with high-amplitude propagating contractures which can cause pain/diarrhea
Treatment focused on ‘RESET’ =Relationship with patient-provider, Education/reassurance, Symptom assessment, Exacerbating/alleviating factors, and Targeting treatment (see Table 1)
Treatment may need to target gut, brain and/or both
Dietary treatments considered 1st line approach
Treatment pharmacology options for IBS-D include antidiarrheals, antispasmotics, rifaximin, eluxadoline, alosetron (rarely, can cause ischemic colitis), bile acid sequestrants
Treatment pharmacology options for IBS-C include polyethylene glycol, lubiprostone, linaclotide, plecanatide, and tegaserod (restricted to women <65 yrs w/o cardiovascular dz)
Treatment pharmacology options for all IBS include TCAs (start with low dose and can titrate upwards; amitriptyline for IBS-C, nortriptyline or desipramine for IBS-M or IBS-C), SNRI (eg. duloxetine (may be better than TCAs in patients with IBS-C and comorbidities like fibromyalgia and depression), mirtazapine (small studies demonstrated benefit for IBS-D and functional dyspepsia), SSRIs (“consider…in patients with predominant anxiety and/or depression…advise against its use as primary treatment for IBS w/o comorbid psychological disorder”), delta ligand agent (eg. pregabalin) (consider if refractory to other treatments), and brain-gut therapies (eg. CBT, GDH)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
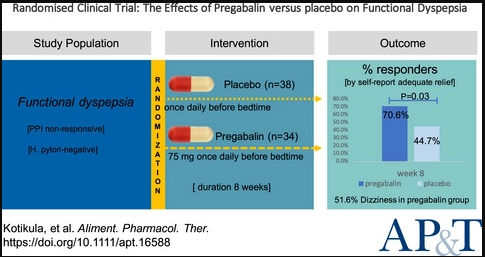
The self-reported adequate relief rates in the pregabalin and placebo groups were 70.6% and 42.1% at week 4 (P = 0.02), and 70.6% and 44.7% at week 8 (P = 0.03), respectively
Pregabalin improved the overall quality of life (P = 0.03)
The most common adverse event with pregabalin was dizziness, occurring in 51.6% of patients
My take: In this study, pregabalin led to significant alleviation of dyspeptic symptoms, especially in patients with predominant epigastric pain.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
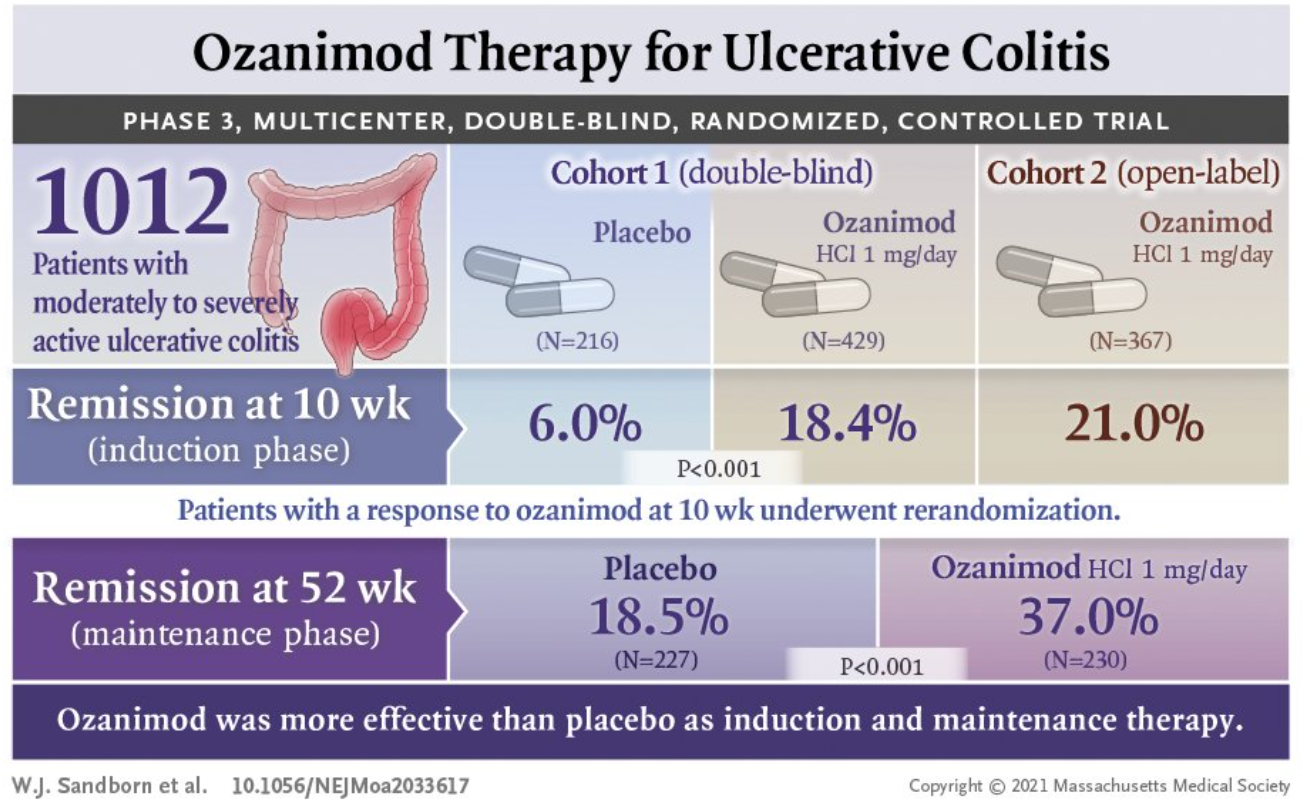
Mechanism of Action: Ozanimod is a selective sphingosine-1-phosphate receptor modulator which leads to internalization of S1P1 receptors in lymphocytes and the prevention of lymphocyte mobilization to inflammatory sites.
Design: There were two initial cohorts of adults with moderately to severely active ulcerative colitis. The first cohort (n=645) of this 52-week multicenter, randomized, double-blind, placebo-controlled trial (285 sites, 30 countries) of ozanimod as induction and maintenance therapy received either 1 mg of ozanimod hydrochloride once a day or placebo. A second cohort (n=457) received open-label ozanimod and was designed to assure that there would be adequate numbers of patients for the maintenance phase. The design allowed up to 30% of the first cohort to have received prior anti-TNF therapy and up to 50% of the second cohort to have received prior anti-TNF therapy. Ozanimod-treated patients with a clinical response during the 10-week induction were randomized again to a treatment group (n=230) or a placebo group for maintenance (n=227). Placebo-treated patients with a clinical response continued to receive placebo.
Approximately 97% of both cohorts had received prior aminosalicylate treatment and ~20% had received prior vedolizumab therapy.
As a safety measure (due to concerns of bradycardia), there was a 7-day period at the start of treatment with dose escalation, starting at 0.25 mg on days 1-4, 0.5 mg on days 5-7, then to 1 mg thereafter.
Key findings:
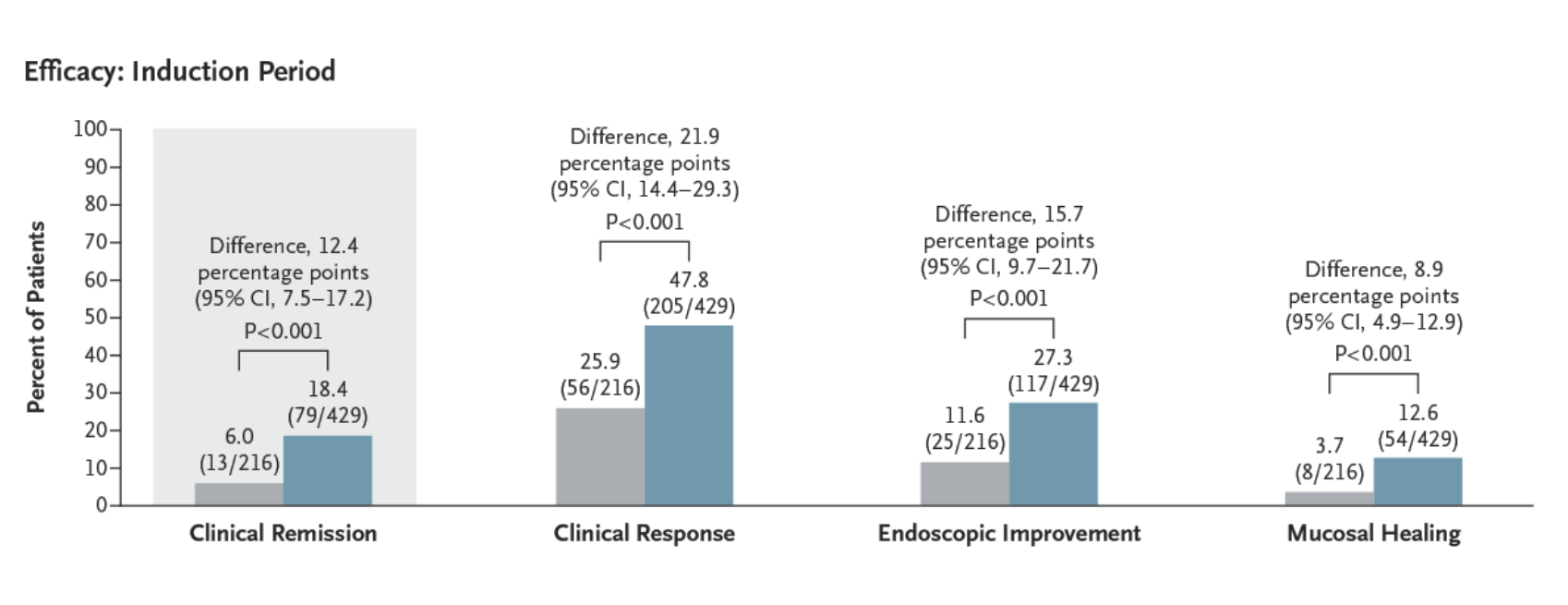
The incidence of clinical remission was significantly higher among patients who received ozanimod than among those who received placebo during both induction (18.4% vs. 6.0%, P<0.001) and maintenance (37.0% vs. 18.5% [among patients with a response at week 10], P<0.001).
The incidence of clinical response was also significantly higher with ozanimod than with placebo during induction (47.8% vs. 25.9%, P<0.001) and maintenance (60.0% vs. 41.0%, P<0.001).
Histologic remission during induction, ozanimod vs placebo: 15.% vs 5.8%.
A post hoc analysis showed decreases in the rectal-bleeding and stool-frequency subscores by week 2 (1 week after the completion of dose adjustment).
From NEJM Twitter Feed
Safety Concerns:
Serious adverse events attributed to ozanimod or placebo occurred in 4 (0.5%) and 2 (0.9%) during induction respectively and none and 1 (0.4%) respectively during maintenance.
Overall alladverse events during induction occurred in 40% of ozanimod-treated patients and 38% of placebo recipients; during maintenance, adverse events were 49% and 37% respectively.
Absolute lymphocyte count (ALC) decreased by a mean of ~54% from baseline to week 10 in ozanimod-treated patients; ALC was <200 in 1.1% (both cohorts) in induction and 17 patients during maintenance. None of the patients with ALC <200 experienced a serious or opportunistic infection.
Serious infections associated wtih ozanimod or placebo occurred in 10 (1.3%) and 1 (0.5%) during induction respectively and 2 (0.9%) and 4 (1.8%%) respectively during maintenance.
Common infections like nasopharyngitis and upper respiratory tract infections in 3-4% of ozanimod-treated patients compared to ~2% of placebo-treated patients
Cancer: during induction there was one ozanimod-treated patient who had a basal cell carcinoma and during maintenance there was one ozanimod-treated patient who had a basal cell carcinoma. In the placebo group, during maintenance there was one patient who developed adenocarcinoma of the colon and one who developed breast cancer.
Among ozanimod-treated patients, bradycardia was evident in 5 (~0.6%) during induction and none during maintenance. (Patients with significant cardiovascular history were excluded from trial)
Among ozanimod-treated patients, hypertension occurred in 13 (~1.6%) during induction and 4 (1.7%); in the placebo group, none in the induction period and three (1.3%) in the maintenance had hypertension.
Prior to entry, the trial required documented varicella zoster IgG antibody or completion of vaccination. Still, HSV occurred in 3 during induction (~0.5%) and 5 (2.2%) during maintenance (only 1 placebo patient (0.4%) had an HSV infection during maintenance.
Elevated liver tests associated wtih ozanimod or placebo occurred in 42 (5.3%) and 2 (0.9%) during induction respectively and 32 (13.9%) and 1 (5.3%%) respectively during maintenance.
Macular edema was noted in 2 ozanimod-treated patients during induction and 1 during maintenance.
My take: This study shows that ozanimod was more effective than placebo in adults with moderately to severely active ulcerative colitis. It will probably be years before we have adequate pediatric data.
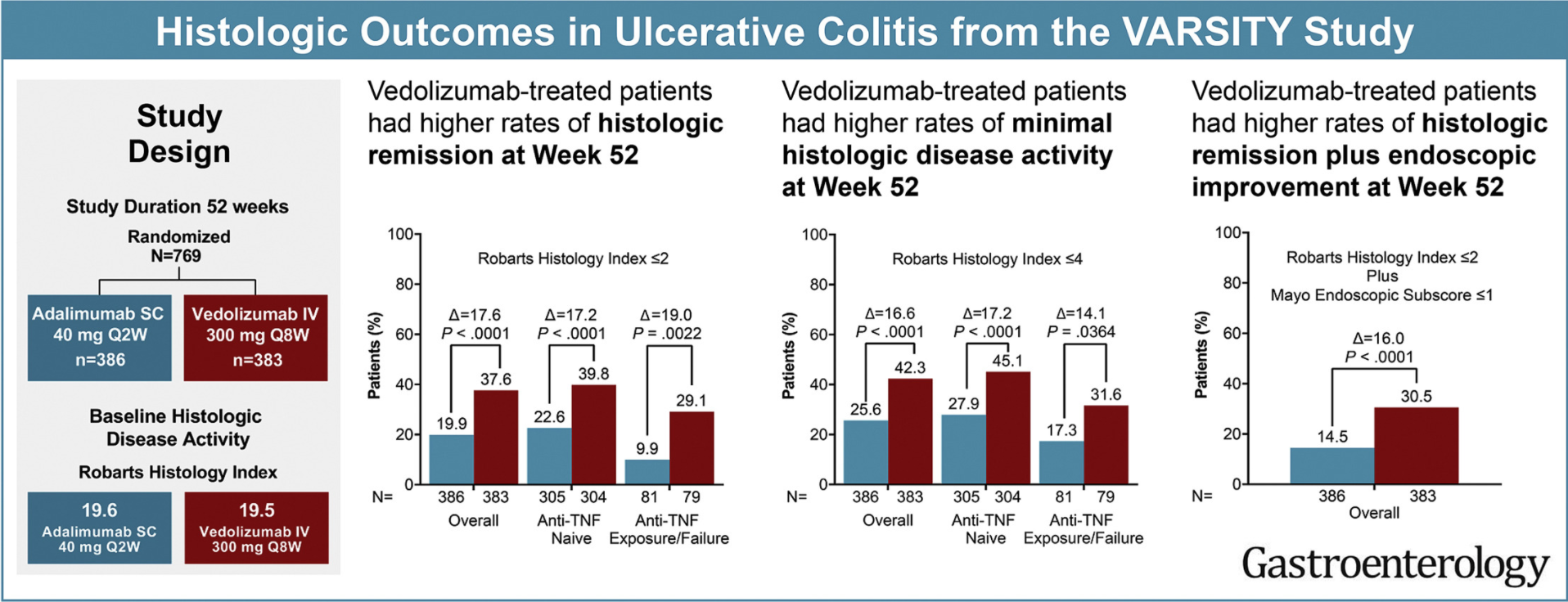
In total, 769 patients received vedolizumab (n = 383) or adalimumab (n = 386). Geboes Index and Robarts Histopathology Index (RHI) scores were used to assess prespecified histologic exploratory end points of histologic remission (Geboes <2 or RHI ≤2) and minimal histologic disease activity (Geboes ≤3.1 or RHI ≤4) at weeks 14 and 52.
Key findings:
Vedolizumab induced greater histologic remission than adalimumab:
week 14: Geboes: 16.7% vs 7.3%, RHI: 25.6% vs 16.1%
week 52: Geboes: 29.2% vs 8.3%, RHI: 37.6% vs 19.9%
Histologic outcomes were generally better in anti–TNF-naïve vs -failure patients
My take: This study shows that histologic outcomes with vedolizumab, similar to clinical outcomes, were better than with adalimumab. Some of this difference could be due to the trail design which did not allow optimization of adalimumab dosing.
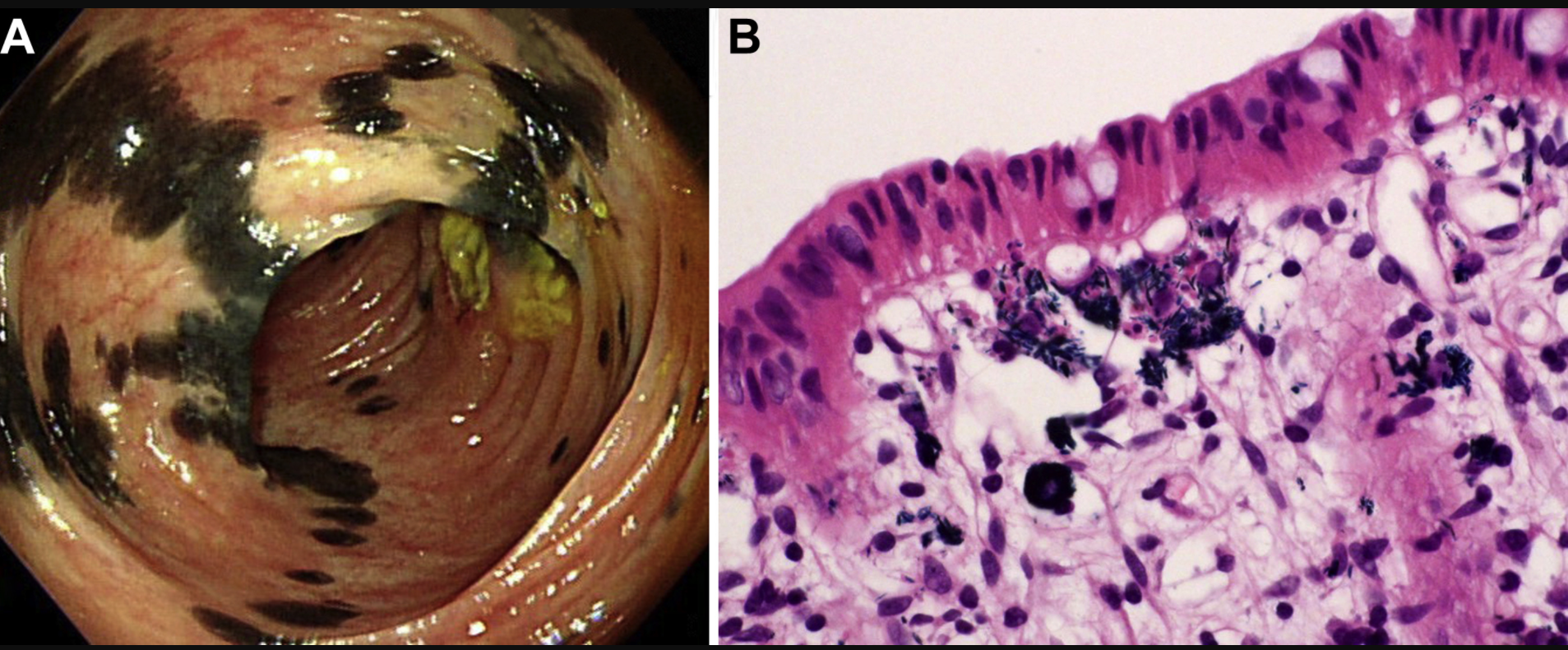
The image below is from a 57 yo woman with Crohn’s disease who was taking a supplement, indigo naturalis (Qing-Dai). “Higher magnification disclosed bluish, needle-like crystals in the cytoplasm of these histiocytes. In light of the presence of pigment-laden histiocytes, we called the lesions indigo naturalis-related pseudomelanosis. Unlike melanosis coli, which typically shows continuous homogeneous brown or black discoloration of colon mucosa (snake-skin appearance or starry sky appearance), indigo naturalis-related pseudomelanosis exhibits a haphazard distribution of black discoloration reminiscent of the skin markings of Holstein Friesian cattle…It remains to be seen whether deposition of indigo naturalis has any long-term adverse effect, although histologically the mucosa with indigo deposition was not accompanied by significant inflammatory activity.”