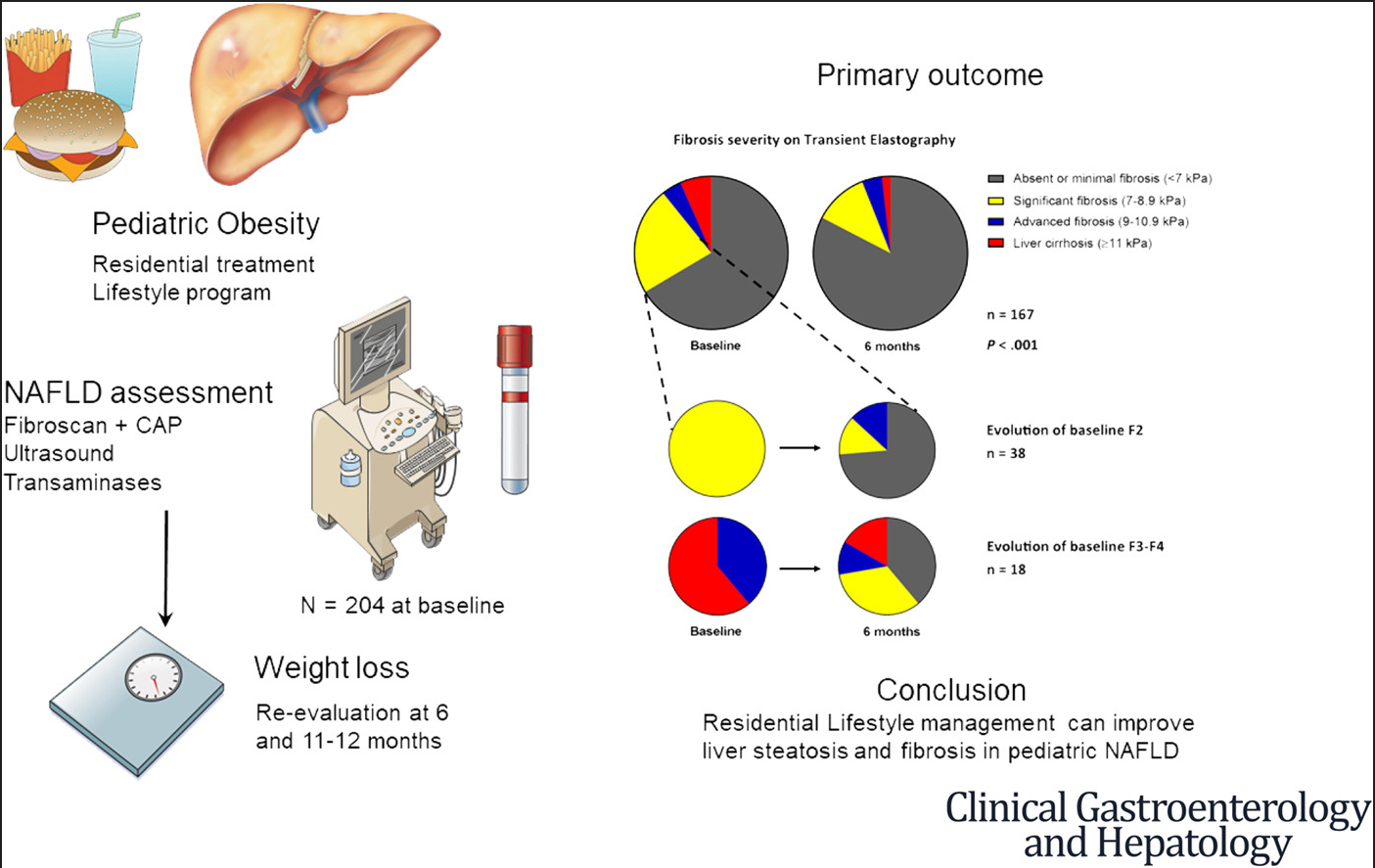
In this prospective study, pediatric patients with NAFLD received intensive lifestyle therapy which encompassed caloric restriction, physical activity, education on a healthy lifestyle, and psychosocial support. Key findings:
After 6 months, the median body weight loss was 16.0% in the 167 patients evaluated. Fibrosis improved in 75.0% (P < .001).
Fasting serum alanine aminotransferase and homeostasis model assessment of insulin resistance decreased significantly over the 1-year period (P < .001).
Related article: MH Malespin et al. Clin Gastroenterol Hepatol 2022; 20: 2393-2395. In this study, adults who were enrolled in TARGET-NASH (n=2019) were reviewed. Only 32% of overweight/obese adults with NAFLD receiving usual care in the U.S. achieved weight loss of 5% or more. In addition, only 25% who lost 5% or more of their weight maintained weight loss at follow-up at 5 years.
My take: Together these studies show that weight loss can reverse liver damage (steatosis and fibrosis) in NAFLD; however, maintaining weight loss with lifestyle treatment is quite difficult. As such, it is anticipated that newer pharmacologic agents (eg. semaglutide) will be available (after appropriate trials), especially for more severe NAFLD.
This retrospective review examined health care utilization within 3 months before and after patients received a constipation action plan (CAP which was implemented in 2019). There were 336 patients who received a CAP and 2812 patients who did not.
Key findings:
There were fewer patient telephone calls for patients who received the CAP (P = 0.0006). The difference in patient electronic messages was not statistically significant (P = 0.09).
There were no differences in UC/emergency department visits or hospitalizations.
Medications for CAP included the following:
Polyethylene glycol 3350, Senna, Milk of Magnesia, Magnesium Citrate, Lactulose, Bisacodyl (tablets, suppository, enema), Normal saline enema, Glycerin suppository, and Sodium phosphate enema
My take: A CAP likely helps educate and empower families on how to manage their child’s symptoms. In this study, it resulted in fewer phone calls (& trend of less electronic messages). Better education is likely to help with patient outcomes even if this is difficult to prove in a retrospective study. This action plan appears easier to understand than a previous CAP, and uses the Red Zone as the cleanout section. Related blog post:Pictographic Constipation Action Plan (2021)
This is a sample of the institution’s constipation action plan (similar to Figure 1) shared by the author.
Methods: In this 5-year retrospective study, the authors identified 22 patients with NRCD; they were following a gluten-free diet for at least 12 months but had persistent symptoms and enteropathy (Marsh 3). Treatments for NRCD were either a GCED (n=13), budesonide (n=9) or both (n=4). Four patients were lost to follow-up and did not receive either treatment.
Key findings:
Thirteen were treated with the GCED for 3 months with 46% achieving both histological and symptomatic resolution
Nine patients were treated with budesonide (6–9 mg daily), with 89% achieving both symptomatic and histologic resolution after a median 3-month treatment course
67% of patients who responded to the GCED and 100% of patients who responded to budesonide remained in remission for at least 6 months following treatment transition back to exclusive GFD
My take: This important article shows that many patients thought to be receiving a GFD can respond to a more stringent approach. In addition, it offers an alternative strategy with budesonide which had a high response rate.
In patients believed to have celiac disease who have persistent or recurrent symptoms or signs, the initial diagnosis of celiac disease should be confirmed by review of prior diagnostic testing, including serologies, endoscopies, and histologic findings.
Best Practice Advice 2
In patients with confirmed celiac disease with persistent or recurrent symptoms or signs (nonresponsive celiac disease), ongoing gluten ingestion should be excluded as a cause of these symptoms with serologic testing, dietitian review, and detection of immunogenic peptides in stool or urine. Esophagogastroduodenoscopy with small bowel biopsies should be performed to look for villous atrophy. If villous atrophy persists or the initial diagnosis of celiac disease was not confirmed, consider other causes of villous atrophy, including common variable immunodeficiency, autoimmune enteropathy, tropical sprue, and medication-induced enteropathy.
Best Practice Advice 3
For patients with nonresponsive celiac disease, after exclusion of gluten ingestion, perform a systematic evaluation for other potential causes of symptoms, including functional bowel disorders, microscopic colitis, pancreatic insufficiency, inflammatory bowel disease, lactose or fructose intolerance, and small intestinal bacterial overgrowth.
Best Practice Advice 4
Use flow cytometry, immunohistochemistry, and T-cell receptor rearrangement studies to distinguish between subtypes of refractory celiac disease and to exclude enteropathy-associated T-cell lymphoma. Type 1 refractory celiac disease is characterized by a normal intraepithelial lymphocyte population and type 2 is defined by the presence of an aberrant, clonal intraepithelial lymphocyte population. Consultation with an expert hematopathologist is necessary to interpret these studies.
Best Practice Advice 5
Perform small bowel imaging with capsule endoscopy and computed tomography or magnetic resonance enterography to exclude enteropathy-associated T-cell lymphoma and ulcerative jejunoileitis at initial diagnosis of type 2 refractory celiac disease.
Best Practice Advice 6
Complete a detailed nutritional assessment with investigation of micronutrient and macronutrient deficiencies in patients diagnosed with refractory celiac disease. Check albumin as an independent prognostic factor.
Best Practice Advice 7
Correct deficiencies in macro- and micronutrients using oral supplements and/or enteral support. Consider parenteral nutrition for patients with severe malnutrition due to malabsorption.
Best Practice Advice 8
Corticosteroids, most commonly open-capsule budesonide or, if unavailable, prednisone, are the medication of choice and should be used as first-line therapy in either type 1 or type 2 refractory celiac disease.
Best Practice Advice 9
Patients with refractory celiac disease require regular follow-up by a multidisciplinary team, including gastroenterologists and dietitians, to assess clinical and histologic response to therapy. Identify local experts with expertise in celiac disease to assist with management.
Best Practice Advice 10
Patients with refractory celiac disease without response to steroids may benefit from referral to a center with expertise for management or evaluation for inclusion in clinical trials.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“Science suggests that chores make kids happy and that you should start assigning little jobs early, even when they are toddlers.”
“Seemingly insignificant chores like setting the table or folding laundry are valuable building blocks toward a child’s independence.”
NY Times (11/1/22): How Brains Send a Signal That It’s Time to Vomit (in mice) Reference article: Z Xie et al. Cell: The gut-to-brain axis for toxin-induced defensive responses “They traced the effect to certain neurons in the brain that released neurotransmitters when the drug [eg. chemotherapy] or the toxin [eg. bacterial] reached the gut. Following those messages back, they discovered cells in the small intestine that reacted to the presence of these noxious substances. A central player in the pathway to nausea and retching was an immune system molecule called interleukin 33, or IL33. Keeping mice from making IL33 significantly reduced their symptoms.”
Three most common causes of infectious esophagitis in children: Candida, HSV and CMV. Asperigillus (& other fungi) as well as bacterial esophagitis are rarely seen. Rare viral infections include human papilloma, varicella zoster and EBV
For Candida, this is typically a benign commensal organism but can become pathogenic due to changes in immunity (immunocompromised including corticosteroids), altered motility and sometimes after antibiotics (with or without PPI therapy). EoE can present with similar-appearing mucosa; thus, biopsy and/or brushing is needed.
With HSV, pediatric case series have reported higher rates in immunocompetent children
Typical treatments: fluconazole for Candida, and Acyclovir for HSV. For CMV, potential treatments include ganciclovir, valganciclovir, foscarnet or cidofovir.
My take: This is a short, good review of the infections that can cause esophagitis in children.
Key findings from this retrospective review (2011-2019):
Of 1801 cases of histologic colitis, 11 patients had CMV found by histology (mean age 15.4, 72.7% female), with an incidence of 0.6%
Nine out of these 11 (81.8%) patients were immunocompromised and 4 (36.4%) had inflammatory bowel disease (IBD) as an underlying diagnosis of whom 2 had new-onset ulcerative colitis
5 of 6 post-transplant patients with CMV colitis had preexisting CMV viremia
An independent analysis of 54 consecutive IBD-associated colectomy cases at TCH showed no histologic evidence of CMV
The study finding that half of the cases of CMV in the IBD population were identified prior to treatment indicates that the underlying IBD may be a more important susceptibility factor than the immunosuppressive medications.
My take: This study indicates that CMV colitis remains important in the post-transplant population but is rarely consequential in the pediatric IBD population.
IBD Updates -January 2017 With regard to CMV and IBD, this study showed “that in most cases the virus is nonpathogenic and thus antiviral is usually ineffective”
Little O’Malley Peak Trail, near Anchorage AK. Denali is visible in background, even though it is ~180 miles away.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“The study included data from 463 observed vedolizumab concentrations (59 peaks and 404 troughs) from 74 patients with IBD (52 with Crohn’s disease and 22 with ulcerative colitis or unclassified IBD, median age 16 years)…This study was part of the multicentre REFINE study, which aimed to investigate paediatric PK factors among different biological therapies. Both induction and maintenance doses were between 6 and 10 mg/kg for patients less than 30 kg and 300 mg for patients above 30 kg.”
Key findings:
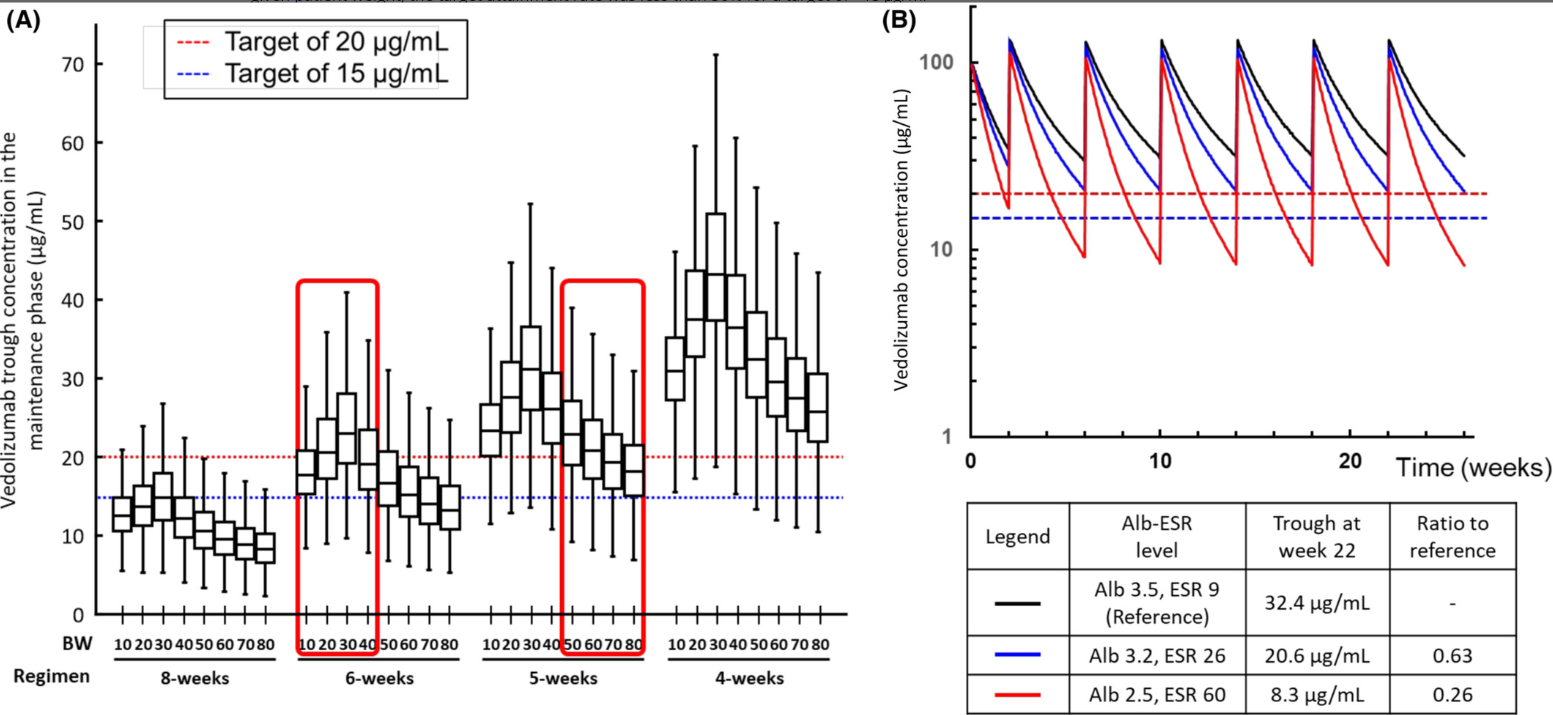
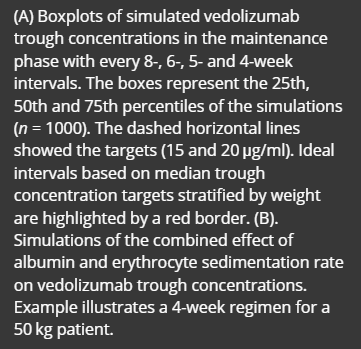
“Using the new model in a simulation analysis of standard vedolizumab infusions (0, 2 and 6 weeks followed by every 8 weeks), we demonstrate that the expected cTrough at week 22 (infusion-5) in the majority of patients would result in drug exposure below current cTrough targets..The dosing simulations in our current study found that receiving standard dosing would lead to <20% of patients achieving a cTrough of 20 μg/ml at infusion-5.”
“The severity of hypoalbuminemia resulted in higher drug CL (lower cTrough) than the inflammatory burden (elevated ESR).”
Infusion-3 cTrough of at least 37 μg/ml and infusion-4 cTrough of at least 20 μg/ml best predicted SFCR (steroid-free clinical remission) at infusion-4. In contrast, we showed inadequate drug exposure during induction (AUCweek 14 of <134,580 μg h/ml) was associated with clinical non-response
My take: This study shows that therapeutic drug monitoring (TDM) is likely to be beneficial in improving outcomes in pediatric patients receiving vedolizumab. Low albumin in particular is associated with increased drug clearance. From this study, it looks like most pediatric patients will need dosing every 4 to 6 weeks to achieve good levels. The authors in their discussion reinforce the utility of TDM to “guide anti-TNF dose optimisations has been shown to improve durability and reduce both immunogenicity and loss of response.”
51 Strik AS, Löwenberg M, Mould DR, Berends SE, Ponsioen CI, van den Brande JMH, et al. Efficacy of dashboard driven dosing of infliximab in inflammatory bowel disease patients: a randomized controlled trial. Scand J Gastroenterol 2021; 56: 145– 154.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: NSAIDs are well-known to cause gastrointestinal injury. While single center studies have suggested that NSAIDs are associated with increased IBD flares, a systemic review of 18 studies found no consistent association between NSAIDs and IBD exacerbation.
This study included 15,705 (44.8%) and 19,326 (55.2%) IBD patients with and without an NSAID exposure.
Key findings:
Findings from a Cox proportional hazards model suggest an association between NSAIDs and IBD exacerbation (HR 1.24; 95%CI 1.16-1.33)
However, the likelihood of an IBD exacerbation in the NSAID exposed arm preceding NSAID exposure was similar (HR 1.30; 95%CI 1.21-1.39).
Those who received NSAIDs were already at increased risk of experiencing a disease flare. And the prior event rate ratio for IBD exacerbation, as determined by dividing the adjusted HR after NSAID exposure by the adjusted HR for pre-NSAID exposure, was 0.95 (95% CI, 0.89 – 1.01).
“A self-controlled case series analysis of 3,968 patients who had both an NSAID exposure and IBD exacerbation demonstrated similar exacerbation rates in the 1-year preceding exposure, 2-6 weeks post-exposure, and 6-weeks to 6-months post-exposure, but higher incidence 0-2 weeks post-exposure, suggesting potential confounding by reverse causality.” The self-controlled part of the study allowed patients to serve as their own controls which allowed adjustment for many factors that are difficult to control with retrospective studies.
75% of patients with IBD who were prescribed an NSAID did not have an IBD exacerbation during a mean of 5.9 years of follow-up
NSAIDs were commonly used: 36.5% of patients with IBD had received at least one NSAID prescription
NSAIDs use was prescribed more frequently in patients with immune targeted therapy (likely a marker for moderate to severe disease)
Discussion points:
The estimated prior event ratio of 0.95 suggests that the risk of IBD flares in NSAID-exposed patients preceded the use of NSAIDs. The risk of IBD exacerbation did not increase in the 2 weeks to 6 months after NSAID exposure.
The overall association of increased IBD flare is likely related to reverse causation. Patients may take NSAIDs due to arthropathy or other symptoms that may be an early manifestation of a flare.
My take: This study challenges the prevailing view that NSAID use worsen inflammatory bowel disease; it is more likely that IBD exacerbations are due to underlying risk from more severe disease and residual confounding/reverse causality. The study provides reassurance that short-duration use is likely to be well-tolerated in most patients with IBD.
No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
Link (12-page) Le Bonheur Dysphagia -Thickeners The algorithms suggest starting with oatmeal and then rice cereal for thickening in infants. Recipes are available for how much cereal is needed for each formula based on desired consistency.
This guide reviews the common thickeners including SimplyThick, Nestle ThickenUp Clear, Hormel: Thick & Easy Clear, Gelmix (see below), Purathick, DysphagiAide, Thick-It, Gerber Rice Cereal, Beechnut Oatmeal Cereal