This was an open-label, retrospective study with 64 patients with collagenous gastritis (CG) (50 adults, 14 children). Budesonide was administered in 2 formulations: open-capsule budesonide or compounded immediate-release budesonide capsule. Key finding: Of the patients treated with topically targeted budesonide (TTB), 89% had a clinical response (42% complete, 46% partial), and 88% had a histologic response (53% complete, 33% partial).
The authors have devised a SQUIRT score for short bowel syndrome. The higher score indicates better enteral tolerance with a highest score of 13 and a lowest score is 3. It is a composite score based on composition, frequency and volume/blowouts. The authors define a blow-out to be a stool loose enough and large enough for the child to require a change of clothes.
How to Score:
Consistency (choose best stool of the day) Playdough, Formed 5 Peanut Butter, Pasty 4 Pudding, Seedy 3 Pea Soup, Loose 2 Water 1
Occurrences (over 24 hours) 1 to 3 4 4 to 6 3 7 to 9 2 Greater Than 10 1 Ostomy Present 0
Volume With Ostomy Without Ostomy (mL/kg) (# of blowouts)
< 10 mL/kg 8 0 =4
10 -14 mL/kg 7 15-19 mL/kg 6 1 =3
20-24 mL/kg 5 2 =2 25-29 mL/kg 4
30-34 mL/kg 3
35 mL/kg 2
>35 mL/kg 1 >3 =1
The authors state that this scoring system has been used in their institution. “This tool can provide objective information to guide clinical decision making. Even patients with ostomies, for whom we can measure stool volume, benefit from SQUIRT scores because including the variable of stool consistency provides a more nuanced assessment than relying on volume.”
My take:This type of scoring system would be useful, primarily in patients in which the volume of stool is difficult to measure. It would benefit from trials to validate its utility.
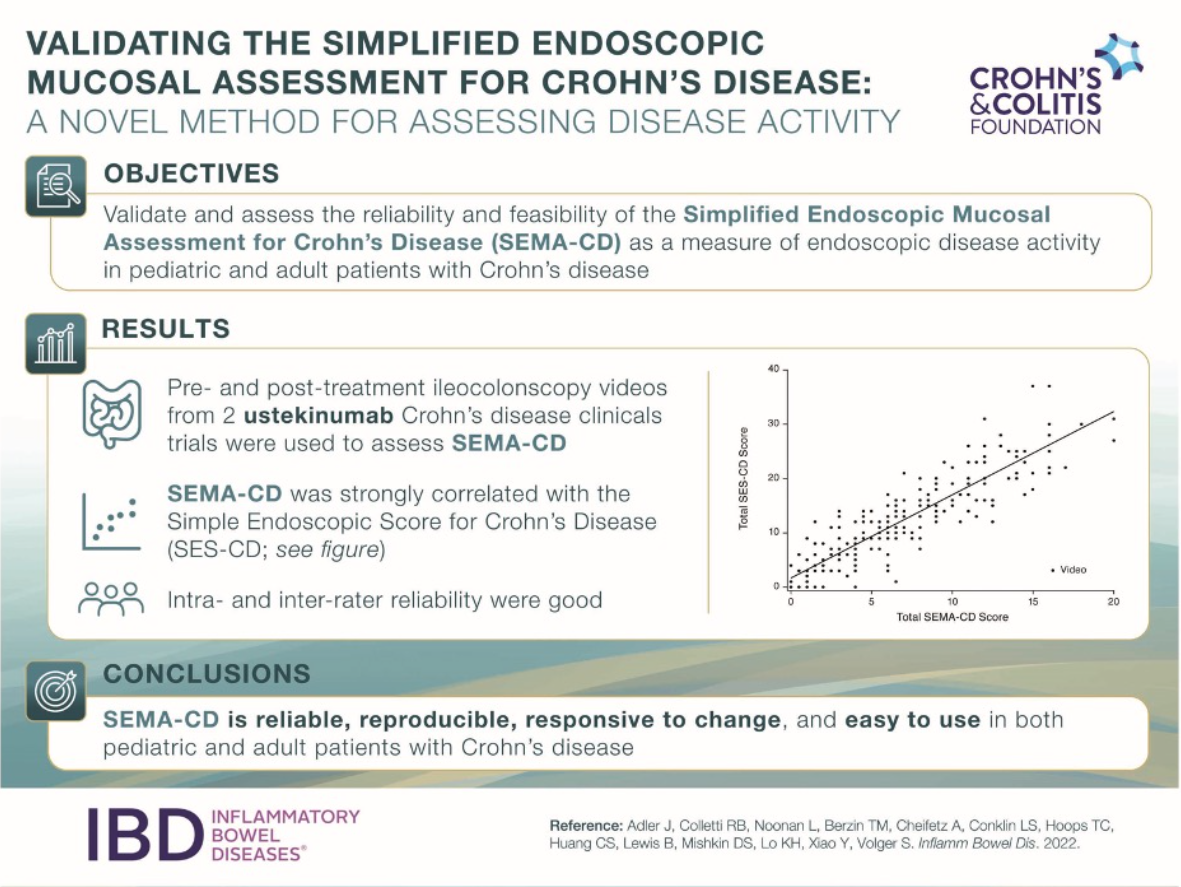
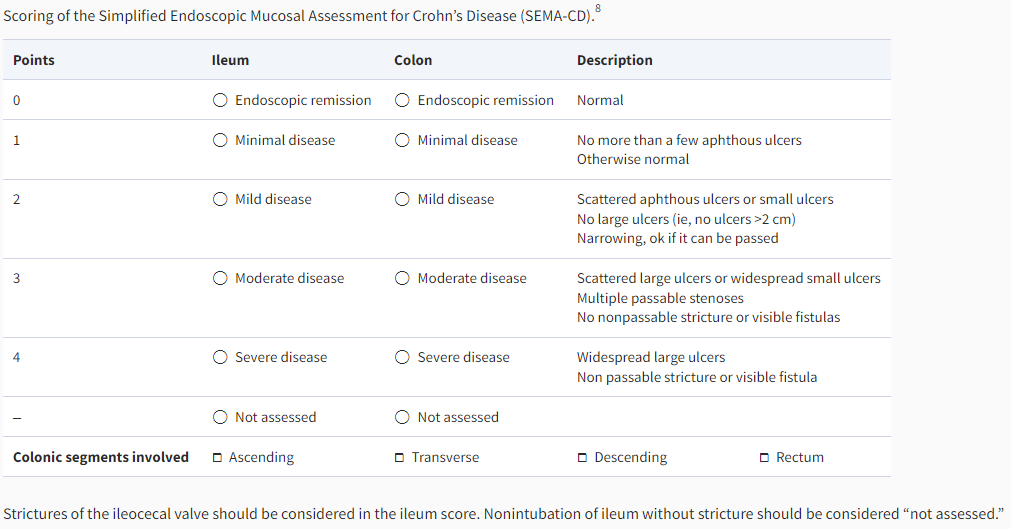
“The SEMA-CD is scored by assigning a numerical value ranging from 0 (endoscopic remission) to 4 (severe disease) for each bowel region (ileum and colon). The overall colon is scored as a whole based on the most severe colonic segment. The number of colonic segments with any degree of active disease is recorded, regardless of the severity of individual segments. The overall colon score is then multiplied by the number of involved colonic segments, and the result is added to the ileum score.”
“The (FDA) has approved 2 vonoprazan-based medications for the treatment of Helicobacter pylori (H. pylori) infection.
Phathom Pharmaceuticals announced the approvals of both the Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin) based on positive safety and efficacy data from the phase 3 PHALCON-HP trial.”
Key findings from this randomized, controlled trial with treatment-naive 1046 adults:
In all patients, vonoprazan triple and dual therapy were superior to lansoprazole triple therapy (80.8% and 77.2%, respectively, vs 68.5% (both superior)
In patients with clarithromycin resistance, vonoprazan triple therapy was effective in 65.8%, dual therapy in 69.6%, vs lansoprazole triple therapy 31.9% (both superior)
Vonoprazan increases intragastric pH rapidly “and maintains it to a greater degree than PPI; this has been associated with higher H pylori eradication rates” (in prior studies as well)
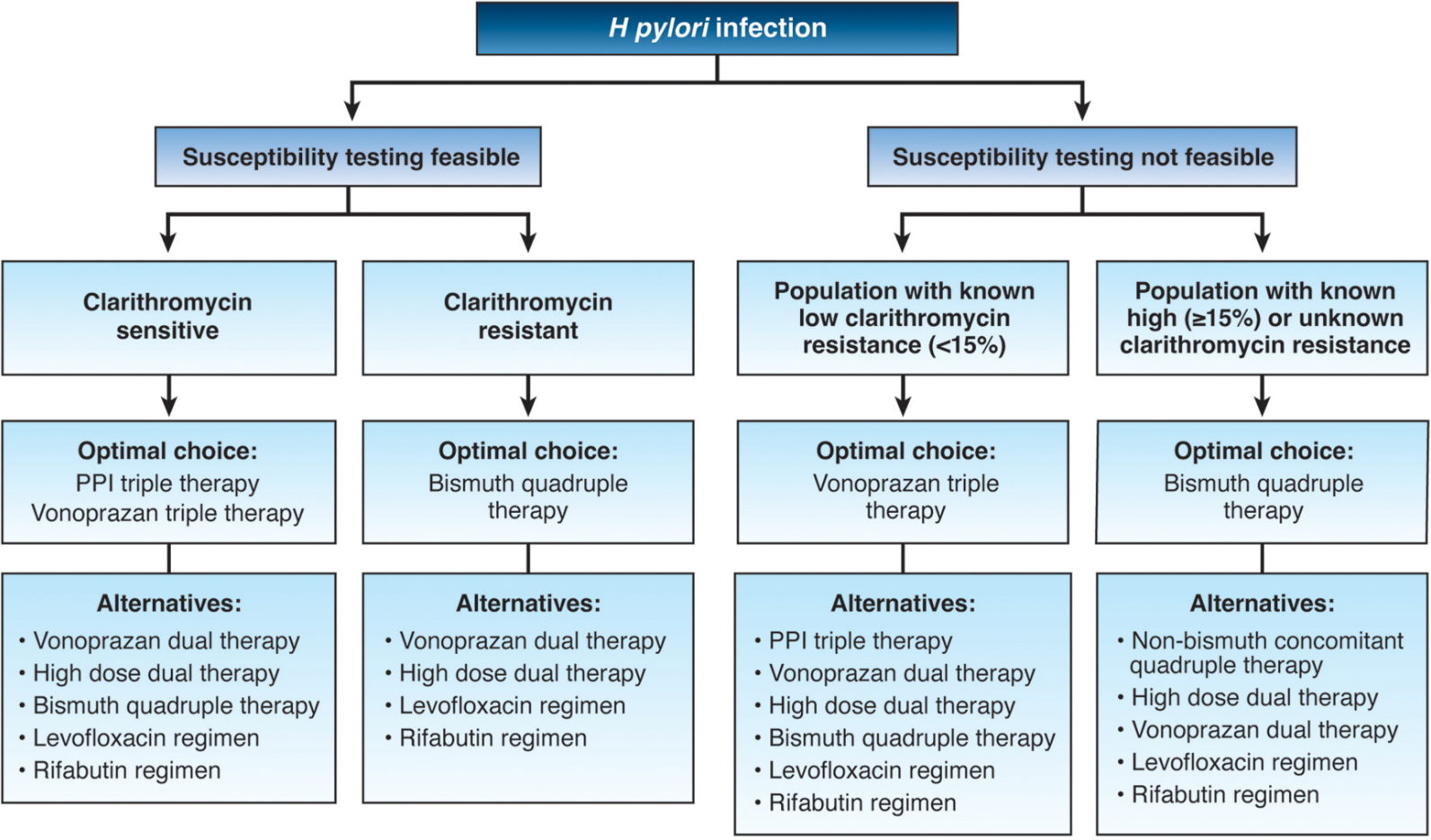
Based on this new information, the author proposes the treatment algorithm below and notes that “the role of increased acid suppression by PPI substitution with vonoprazan should be examined in other H pylori regimens.” The author favors bismuth quadruple therapy in those with clarithromycin resistance as non-bismuth quadruple therapy utilizes an unnecessary antibiotic (clarithromycin).
Other points:
Metronidazole resistance is fairly common, but bismuth quadruple therapy can overcome much of the metronidazole resistance
Levofloxacin resistance is quite high in certain regions and should only be used with caution, given recent warnings from the US Food and Drug Administration of aortic rupture in susceptible individuals
Rifabutin can cause some bone marrow suppression
My take: With the more widespread availability of susceptiblity testing (beyond clarithromycin), I anticipate more targeted treatments. At the same time, vonoprazan-based treatments are likely to be important in increasing eradication rates.
Related blog posts:
How To Achieve Helicobacter Pylori Cure Rates of >95% This post lists some of the codes from several commercial companies that perform susceptibility testing. The Quest code has been updated. Our Quest representative indicated code: 36994 (H. pylori culture with reflex to susceptibility). Preferred Specimen: 3 mm Gastric/Antral or Duodenal biopsy collected in Brucella broth or Trypticase Soy Broth (TSB) with 10-20% glycerol
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In 2018, Belcher pharmaceuticals managed to get the FDA to designate Ethanol as an orphan drug with a subsequent increase in cost to ~$10,000 for a 10-vial pack (10-day supply) (Related post: FDA ‘Safety Initiative’ Now Means an Ounce of Ethanol Costs $30,000). As such, many (?most) children with intestinal failure (IF) no longer have access to this therapy which prevents life-threatening infections to their central lines.
A recent retrospective study (R Josyabhata et al. JPGN 2022; 75: 304-307. Sodium Bicarbonate Locks May Be a Safe and Effective Alternative in Pediatric Intestinal Failure: A Pilot Study) examined the use of sodium bicarbonate lock therapy (SBLT) as an alternative to ethanol in four children. This study was prompted by a clinical trial in hemodialysis patients which demonstrated a reduction in catheter-related bloodstream infections (CRBSI). None of the four patients had a CRBSI.
My take: A much larger multi-center study will be needed to determine if SBLT is worthwhile.
K Culbreath et al. JPGN 2022; 75: 345-350. Antibiotic Therapy for Culture-Proven Bacterial Overgrowth in Children With Intestinal Failure Results in Improved Symptoms and Growth This article describes outcomes of 104 children with intestinal failure who underwent endoscopy and had duodenal cultures sent to identify bacterial overgrowth/susceptibility/targeted antibiotics. This information was associated with fewer symptoms and better growth. The methods section provides detailed information on collection and handling of specimens (which could be helpful for those trying to implement this strategy). However, there is not a standardized protocol for duodenal cultures to detect bacterial overgrowth.
This is a terrific review of POEM; it explains the procedure technique (with pictures), outcomes, indications and adverse events. The paper indicates that more than 300 children (as young as 11 months) have had POEM in published studies with good outcomes.
Interestingly, the authors state that 20-40 procedures “should be performed for competency and that 60 are required to achieve mastery.” Also, long-term data are lacking.
My take: POEM has good data supporting its use, especially in adults. Still, it will be quite difficult for pediatric gastroenterologists to acquire sufficient expertise to do this procedure.
“Exit Glacier” in Kenai Fjords National Park. This picture shows how much the glacier has retreated since 2005 due to global warming (the ice used to extend to this sign).
Design: A prospective observational single-center study in 41 children with EoE treated with the 1-food elimination diet (1FED). Upper endoscopy with biopsies was performed after 8 to 12 weeks of treatment. The primary end point was histologic remission, defined as fewer than 15 eosinophils per high-power field.
Key findings:
Histologic remission occurred in 21 (51%) children, with a decrease in peak eosinophils per high-power field from a median of 50
Endoscopic abnormalities improved in 24 (59%) patients, while symptoms improved in 25 (61%). Improved symptoms included chest pain, dysphagia, and pocketing/spitting out food
Interestingly, in terms of all symptom resolution, this was higher in the group of nonresponders 8 (40%) than in the responders 4 (19%)
Younger patients (mean 7 yrs vs 12 yrs) and patients with IgE-mediated food allergies tended to be more likely to fail dairy elimination in this study
One key caveat is that most patients continued PPI during study; thus it is unknown if stopping a PPI before starting dairy elimination would have changed treatment response. 90% of patients were receiving PPIs at enrollment
My take: This study should prompt more widespread use of dairy elimination as a first line treatment prior to consideration of medications for long-term treatment. This study also reinforces the concept that symptom improvement remains an inadequate indicator of response. Perhaps, Chick-Fil-A marketing needs to be used for our EoE patients to shun cows (cow’s milk in this case).
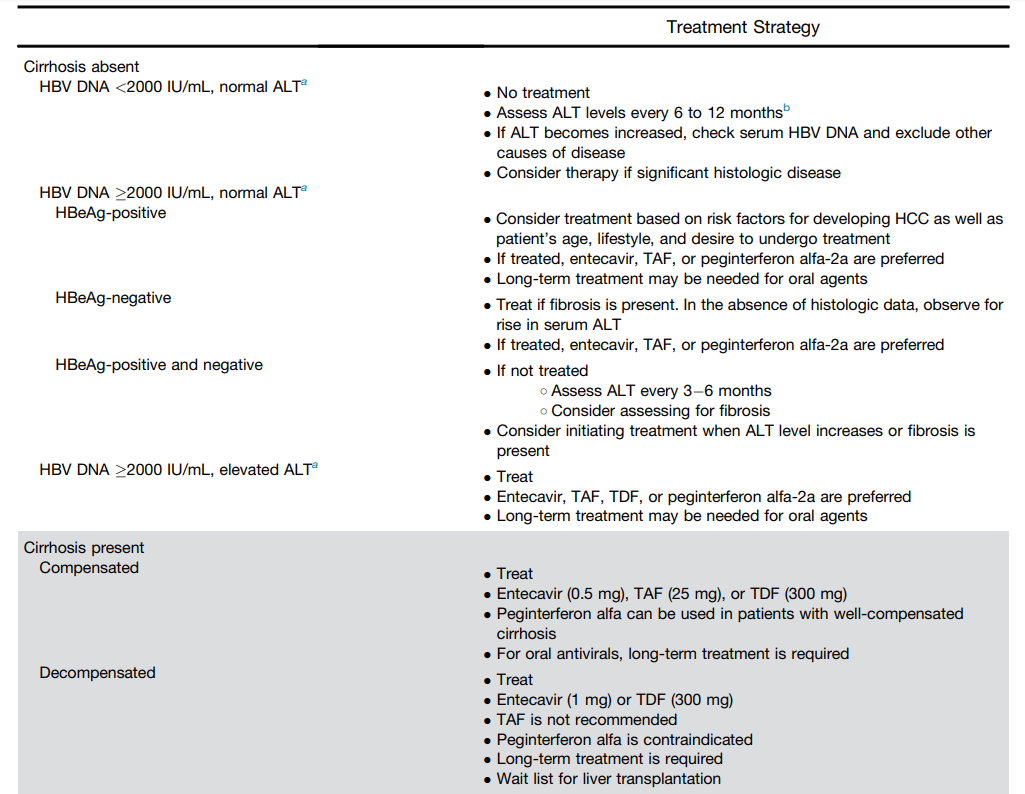
This article provides an updated treatment algorithm with many changes since 2015.
Key points:
New terminology. The authors provide updated terminology. The term ‘immune tolerant’ is losing favor. “There is also evidence that during the immune tolerant phase virologic events occur, such as integration of viral DNA into the host genome, which may help set the stage for the subsequent development of HCC.” As such, the new terminology focuses on “describing the 2 main characteristics of chronicity, infection alone and infection with evidence of ongoing hepatic inflammation (ie, hepatitis).” (See below)
TAF preferred over TDF. “The 4 first-line therapies available for managing CHB infection in the United States are peginterferon alfa-2a, entecavir (ETV), tenofovir disoproxil fumarate (TDF), and tenofovir alafenamide (TAF)….It is the opinion of most—but not all—members of the panel that when antiviral therapy is contemplated, TAF is preferred over TDF because of the lower risks of renal or bone side effects and higher likelihood of ALT normalization through 48 weeks.” For decompensated cirrhosis, TAF and peginterferon are NOT recommended.
Long term treatment is the rule (not the exception). “HBeAg-positive patients with evidence of less extensive fibrosis (<F3) should be treated long-term, even after HBeAg seroconversion and virologic suppression because of the risks of virologic relapse55 and ALT flares, except when treatment is initiated solely for the purpose of prevention of vertical transmission…For HBeAg-negative patients without HBsAg seroconversion, the panel does not recommend stopping treatment.”
Monitoring. “Primary nonresponse to ETV, TDF, or TAF is rare; therefore, any patients who are not responsive to these agents after 12 to 24 weeks should be evaluated for compliance.”
Table 1 (see below) summarizes treatment recommendations. In almost all patients with HBV, if there is elevated ALT, treatment is recommended.
Terminology:
Table for Treatment Recommendations:
In the article, more information is available, including recommendations for treatment in the setting of HIV coinfection
My take: Forget about “immunotolerant” HBV. Until better treatments emerge, patients with HBV and elevated liver enzymes are likely to need long-treatment if using TAF, TDF or entecavir.
“In an effort to reduce the risk of children and teens experiencing serious, even life-threatening injuries from swallowing dangerous, small high-powered magnets, the U.S. Consumer Product Safety Commission (CPSC) voted to approve a new federal safety standard for magnets on September 7, 2022.”
“The new mandatory federal standard requires loose or separable magnets in certain magnet products to be either too large to swallow, or weak enough to reduce the risk of internal injuries when swallowed; specifically, if the magnets fit in a small parts cylinder, then they must have a flux index of less than 50 kG2 mm2.”
“CPSC estimates 26,600 magnet ingestions were treated in hospital ERs from 2010 through 2021, and cases have been rising annually since 2018. CPSC is aware of seven deaths involving the ingestion of hazardous magnets (including two outside of the United States), the majority of these incidents likely involved magnet sets.”
“CPSC urges anyone who may own these magnets and magnet sets to discard them to protect children who may come into contact with them and unintentionally ingest them. “