Adalimumab trough levels (TLs) at both weeks 4 and 8 were significantly higher in remitters vs nonremitters at week 24 (P < 0.001 and P = 0.002, respectively)
The best ADA TL cutoffs at weeks 4 and 8 for predicting clinical/biomarker remission at week 24 were 22.5 µg/mL (80% sensitivity, 90% specificity) and 12.5 µg/mL (94% sensitivity, 60% specificity) respectively
My take (borrowed from authors): Greater early ADA exposure is associated with superior clinical/biomarker outcomes at week 24. ADA pediatric dosing is looking a lot like infliximab dosing in which nearly 75% would be underdosed if using on-label dosing.
Using a selected sample from a database with >62 million patients, this retrospective cohort study determined the rates of colorectal cancer among patients with IBD. Key finding:
Among the IBD cohort, patients treated with anti-TNF agents were less likely to develop CRC; patients with Crohn’s disease: odds ratio, 0.69; 95% confidence interval, 0.66-0.73; P < 0.0001 vs patients with ulcerative colitis: odds ratio, 0.78; 95% confidence interval, 0.73-0.83; P < 0.0001.
My take: This study found an association between anti-TNF therapy and a reduced risk of CRC in patients with IBD.
Using the National Health Interview survey (2015), the authors identified individuals with self-reported IBD and assessed national estimates of financial toxicity. Key findings:
23% reported financial hardships due to medical bills, 16% of patients reported cost-related medication nonadherence, and 31% reported cost-reducing behaviors
Approximately 62% of patients reported personal and/or health-related financial distress, and 10% of patients deemed health care unaffordable
Inflammatory bowel disease was associated with 1.6 to 2.6 times higher odds of financial toxicity across domains compared with patients without IBD
My take: In addition to the physical and emotional toll of having IBD, there is also significant financial hardships for many.
Methods: Data from 6 ustekinumab phase 2/3 CD and UC studies were pooled, and safety was evaluated through 1 year; this included 2574 patients (1733 patient-years of follow-up)
Key Safety findings –Events per 100 patient years -placebo vs ustekinumab respectively:
Major cardiovascular events were rare with 2 in placebo group 0.34 and 2 in the ustekinumab group 0.12
Morekey findings:
No cases of progressive multifocal leukoencephalopathy or reversible posterior leukoencephalopathy
Antibodies to ustekinumab were identified in 3.6% of patients
My take: This study showed similar safety between ustekinumab and placebo, but is limited by short followup. The authors note that 5-year data from ustekinumab’s use with psoriasis has found no safety signals for malignancy.
This cross-sectional study with 229 patients examined the relationship between inflammatory bowel disease (IBD) activity and resilience based on the Connor-Davidson Resilience Scale questionnaire (high resilience score ≥ 35).
Key findings:
High resilience was noted in 27% of patients with UC and 21.5% of patients with CD.
Among patients with UC, those with high resilience had a mean Mayo score of 1.54, and those with low resilience had a mean Mayo score of 4.31, P < 0.001.
Among patients with CD, those with high resilience had a mean HBI of 2.31, and those with low resilience had a mean HBI of 3.95, P = 0.035.
In multivariable analysis, high resilience was independently associated with lower disease activity in both UC (P < 0.001) and CD (P = 0.037) and with higher QoL (P = 0.016).
High resilience was also associated with fewer surgeries (P = 0.001) among patients with CD.
Reading this study, made me think of Galen’s assertion about a different treatment, circa 100 AD: “All who drink of this remedy recover in a short time except those whom it does not help, who all die. It is obvious, therefore, that it fails only in incurable cases.” In the case of this study, the remedy is resiliency.
This study is intriguing and adds to the literature that mental health and IBD may be a two-way street: mental health may affect IBD and IBD activity may affect mental health. However, it is difficult to prove causation in a cross-sectional study. Reverse causation is possible; that is higher disease burden may result in lower resilience.
Also, it is not clear to me that resilience is a particularly modifiable factor. Some may interpret this study in a ‘blame the victim’ mode. I think a lot of individuals would think they are resilient but most do not know until they face a difficult situation. Perhaps, Mike Tyson’s assertion is more apt: “Everyone has a plan until they get punched in the mouth.”
My take: This study does not prove that resilience helps prevent IBD activity, though being resilient is nice if you have it.
Plus one: JR Rosh et al. J Crohns Colitis. 2021 May 26; jjab089. doi: 10.1093/ecco-jcc/jjab089. (EPUB). Ustekinumab in Pediatric Patients with Moderately to Severely Active Crohn’s Disease Pharmacokinetics, Safety, and Efficacy Results from UniStar, a Phase 1 Study This was a “multicentre, 16-week, double-blind induction dose-ranging study (NCT02968108), patients aged 2-<18 years; patients were randomized (1:1) to one of 2 weight range-based intravenous induction doses: 130mg vs 390mg in patients ≥40kg and 3mg/kg vs 9mg/kg in patients <40kg. At week 8, all patients received a single subcutaneous ustekinumab maintenance dose of 90mg in patients ≥40kg or 2mg/kg in patients <40kg..” (Kudos to my partner, Stanley Cohen, one of the authors)
Key finding: Pharmacokinetics were similar to those in adults with Crohn’s disease. However, serum ustekinumab concentrations were lower among those with body weight <40kg…These results suggest a different dosing regimen may be required for patients <40kg
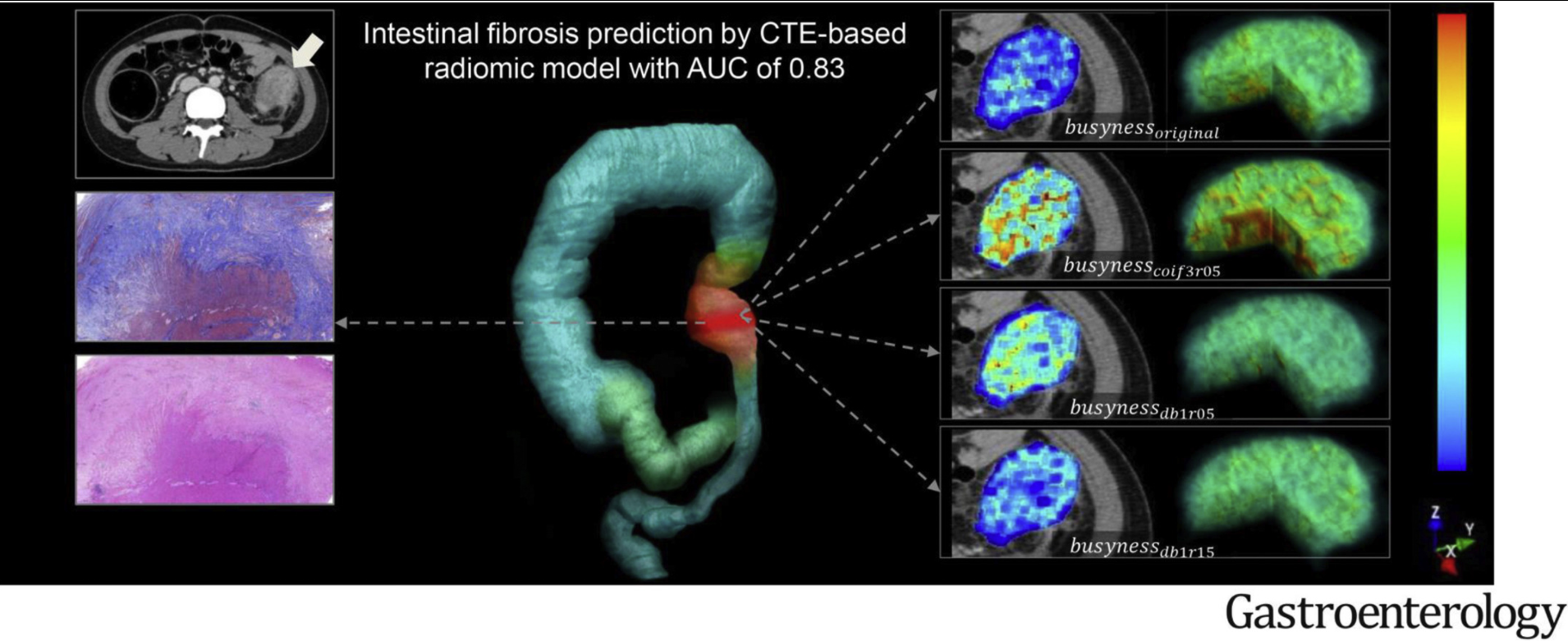
Methods: This article describes the development a computed-tomography enterography (CTE)–based radiomic model (RM). This retrospective multicenter study included 167 CD patients who underwent preoperative CTE and bowel resection. 1454 radiomic features were extracted from venous-phase CTE and a machine learning–based RM was developed based on the reproducible features using logistic regression. The RM was validated in an independent external test cohort recruited from 3 centers.
Key findings:
In the training cohort, the area under the ROC curve (AUC) of RM for distinguishing moderate–severe from none–mild intestinal fibrosis was 0.888.
In the test cohort, the RM had an AUC of 0.816.
RM was more accurate than visual interpretations by either radiologist (radiologist 1, AUC = 0.554; radiologist 2, AUC = 0.598; both, P < .001) in the test cohort
My take: This CT approach with RM allowed for accurate characterization of intestinal fibrosis in CD. The images look pretty cool too.
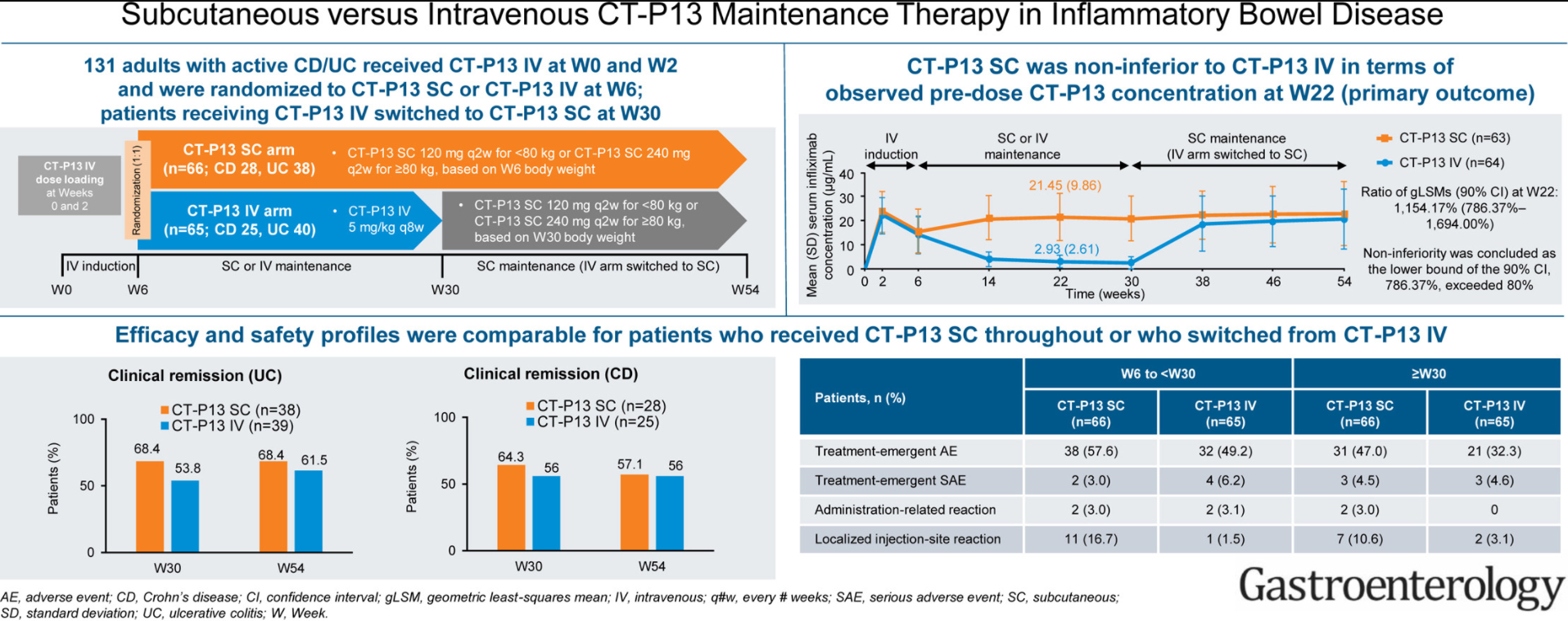
Methods: Overall in this phase 1 randomized, open-label study in patients with either ulcerative colitis or Crohn’s disease, 66 and 65 patients were randomized to CT-P13 SC (every 2 weeks) and CT-P13 IV, respectively
Key findings: The pharmacokinetic noninferiority of CT-P13 SC to CT-P13 IV, and the comparable efficacy, safety, and immunogenicity profiles
These findings are in agreement with similar studies performed in patients with Rheumatoid Arthritis.
My take: If confirmed with additional studies, it is likely that SC infliximab treatment will be a useful alternative to intravenous infliximab. This is similar to data presented with vedolizumab which is currently administered intravenously.
This in-depth report reviews pyoderma gangrenosum including the differential diagnosis, the pathophysiology/genetics, presentation/diagnosis and treatment approaches. Anti-TNF therapy: “Currently available published data support using an anti-TNF-α biologic agent as first-line therapy for severe PG therapy in pediatric IBD, as well as for those cases that have not responded to local therapies.”
This reported case series with 5 patients with severe ulcerative colitis (UC) who received a combination of tofacitinib and infliximab for at least 90 days were retrospectively reviewed. Tofacitinib dosing was de-escalated to 5 mg twice daily after 8 weeks. Thiopurine therapy was stopped with tofacitinib initiation.
Key findings:
Median duration of combination therapy was 9 months (range, 4–12 months). At 90 days, all patients had a reduction in Mayo score of ≥3. Four patients improved clinically and biochemically (Table 1), with 3 patients achieving steroid-free remission.
The only adverse event reported was one patient developing varicella zoster.
The authors letter title regarding tofacitinib being “safe and effective” is clearly overstated. The reply notes that in limited experience the group from the University of Michigan had a 50-year-old man develop severe pulmonary and CNS disease due to acquisition of legionnaires disease while on combination tofacitinib and infliximab.
My take: (borrowed from reply) “Efficacy and safety data obtained through rigorous randomized trials are needed…it is possible that long-term use of combination tofacitinib and infliximab will lead to an unacceptable risk of infection.”
Another study of tofacitinib: GR Lichtenstein et al. Inflamm Bowel Dis 2021; 27: 816-825. Tofacitinib, an Oral Janus Kinase Inhibitor: Analysis of Malignancy (Excluding Nonmelanoma Skin Cancer) Events Across the Ulcerative Colitis Clinical Program Key finding: With an exposure of 2576.4 patient years & 124 overall cohort tofacitinib-treated patients, 20 developed a malignancy
In this retrospective study with 129 patients (mean age 25 yrs, mean disease duration 14.5 yrs) whose CD was in clinical/endoscopic remission, the authors examined factors associated with clinical relapse within 2 years; this included dose escalation, change in therapy, need for systemic steroids, or CD-related hospitalization or surgery.
Key findings:
Within 2 y of endoscopic evaluation, 42 patients (32.6%) had a clinical relapse.
There were no significant differences in proportions of patients with active ileal CD (23.8%), quiescent CD (28.6%), or normal histology (37%) between those who relapsed and those remaining in remission (P = .43). In addition, there was no no association between histologic features of active disease in ileal histology biopsies and symptom scores (Harvey Bradshaw index and simple inflammatory bowel disease questionnaire scores)
There were no significant differences in proportions of relapses among patients with active colonic disease (38.1%), quiescent disease (35.0%), or normal histology (27.9%, P = .73).
My take: In terms of outcomes, clinical and endoscopic remission are important but whether histologic remission is needed is unclear (at this time).
Related blog posts:
Histologic Healing and IBD Outcomes –several studies showed that histologic healing in ileal Crohn’s disease and in ulcerative colitis are associated with better outcomes
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Data pooled from 27 studies showed the prevalence of NAFLD among IBD patients was 32% (substantial heterogeneity); this is “statistically significantly higher than the prevalence of NAFLD in the general population (25.2%; P < 0.001)”
A total of 93 studies were identified, comprising 16,064 IBD patients with co-occurring IMIDs and 3,451,414 IBD patients without IMIDs. IMIDs included the following:
Unspecified autoimmune disease
Diabetes type 1
Asthma
Grave disease
Spondyloarthropathy
Ankylosing spondylitis
Iridocyclitis
Uveitis
Rheumatoid arthritis
Polymyalgia rheumatica
Psoriasis/psoriatic arthritis
Primary Sclerosing Cholangitis
Celiac disease
Pyoderma gangrenosum
Pernicious anemia
Autoimmune hepatitis
Sarcoidosis
Giant cell arteritis
Primary biliary cholangitis
Hashimoto thyroiditis
Episcleritis
Sjogren syndrome
Key findings: Patients with IBD and co-occurring IMIDs were at increased risk of having extensive colitis or pancolitis (risk ratio, 1.38; 95% Cl, 1.25–1.52; P < 0.01, I2 = 86%) and receiving IBD-related surgeries (risk ratio, 1.17; 95% Cl, 1.01–1.36; P = 0.03; I2 = 85%) compared with patients without IMIDs