




My notes from Georgia Chapter of CCFA’s conference. There could be errors of omission, transcription and/or errors in context based on my understanding.
Evan Feldman, MD –Atlanta Colorectal Surgery
Surgical Management of Fibrostenotic Crohn’s Disease
Key Points:


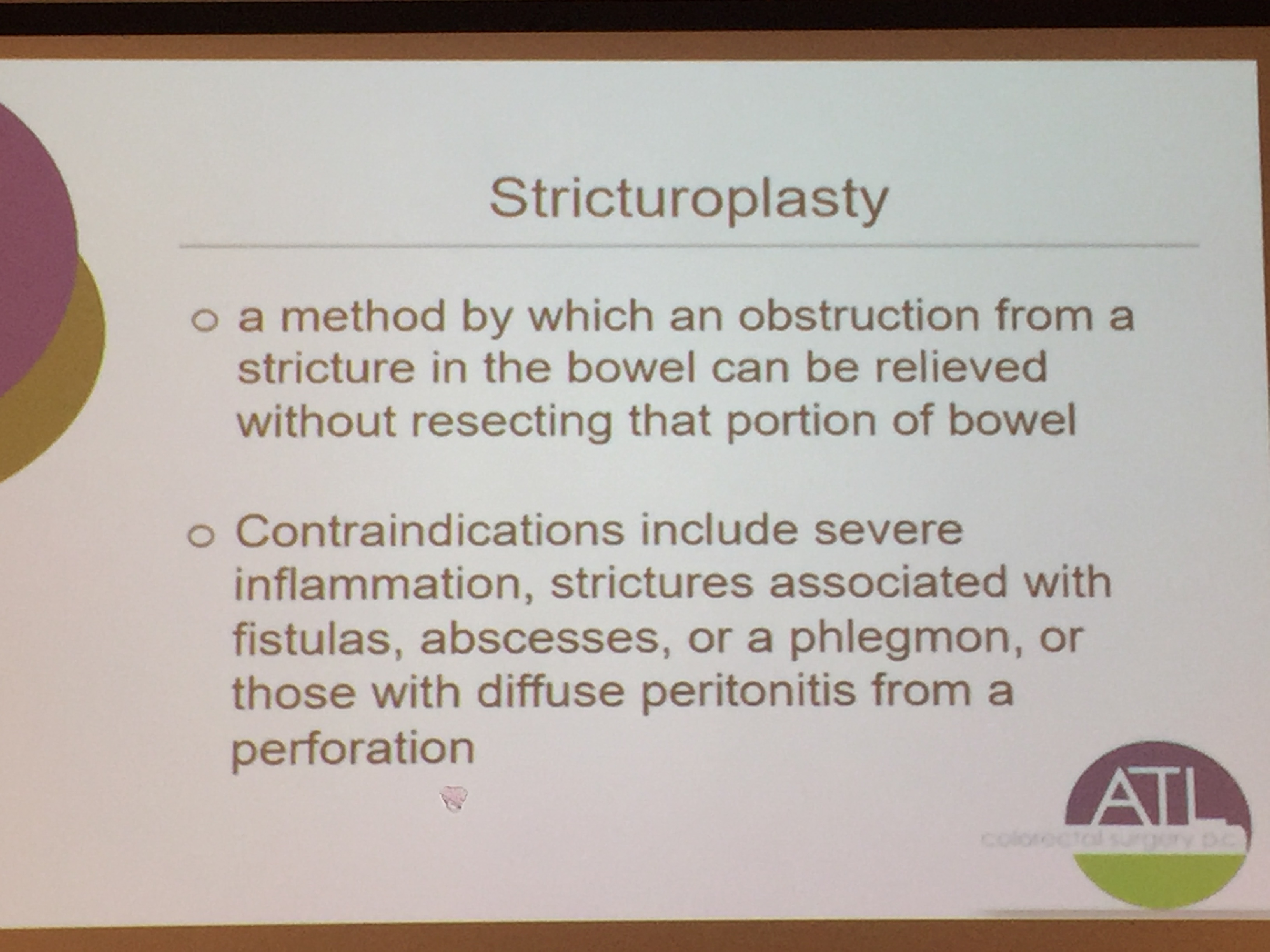



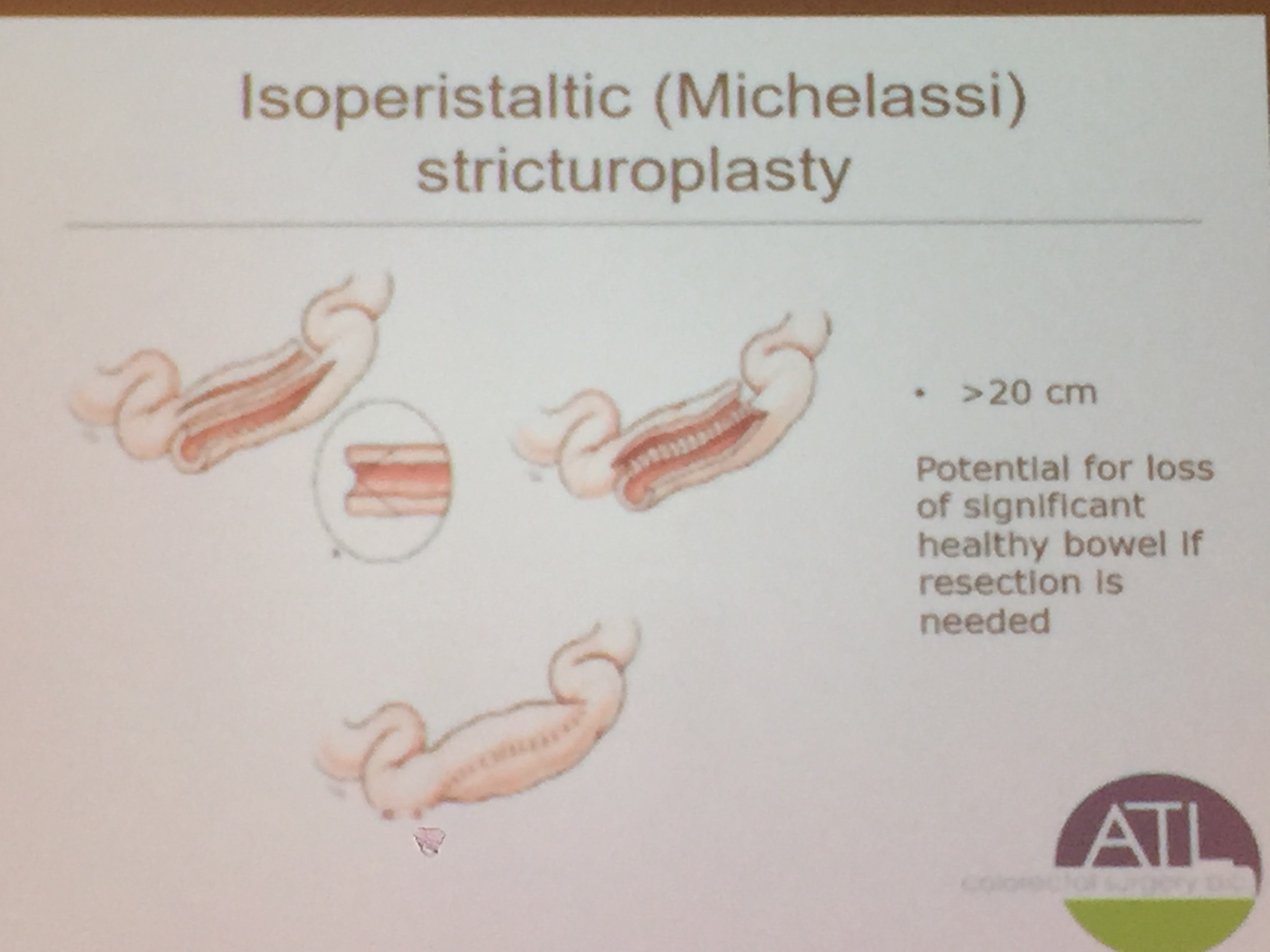
The slide above depicts a Michelassi stricturoplasty which is rarely performed, but considered for long segments of strictured bowel.
Related blog post:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
My notes from Georgia Chapter of CCFA’s conference. There could be errors of omission, transcription and/or errors in context based on my understanding.
Sandy Kim, MD –Children’s Hospital of Pittsburgh
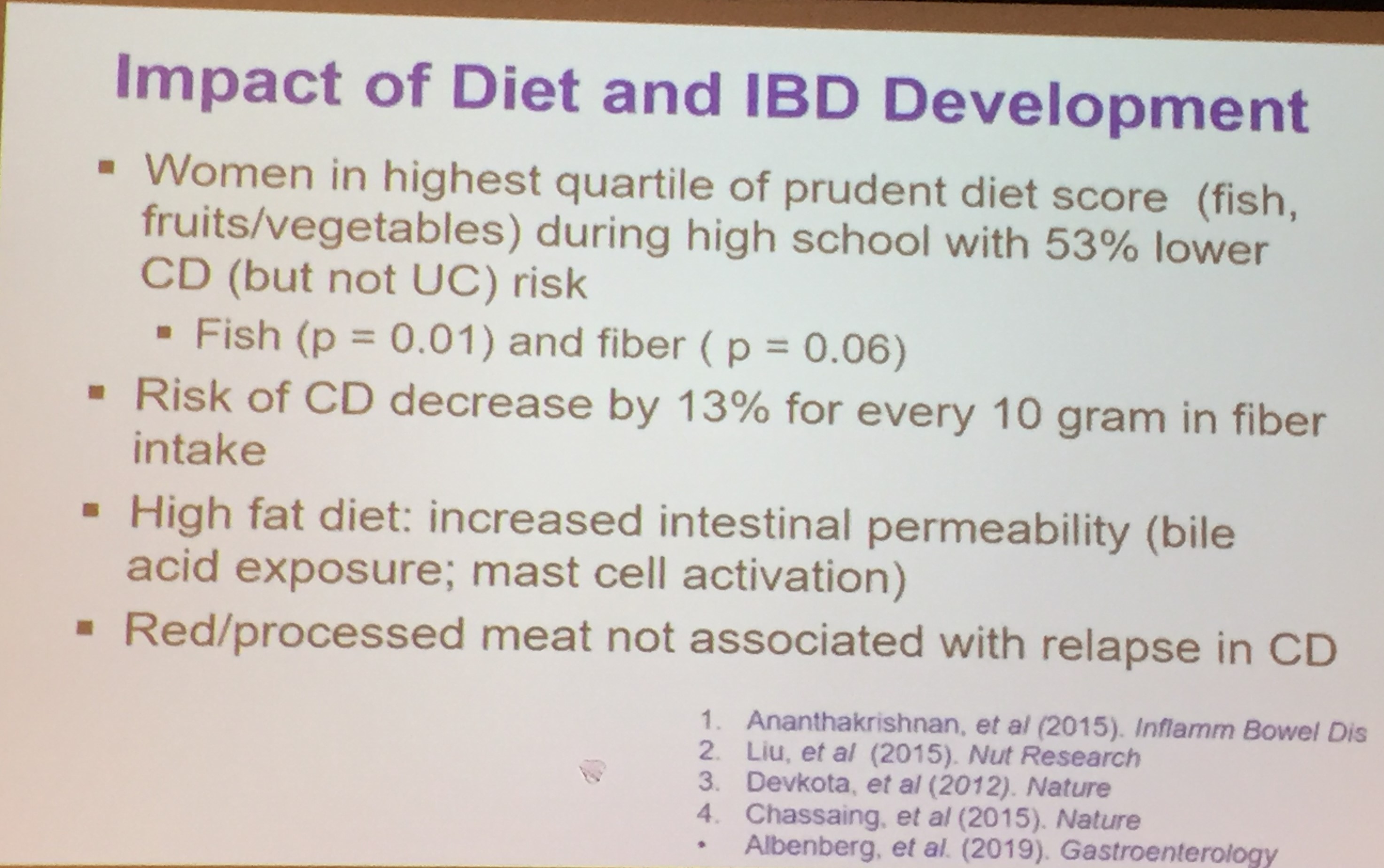
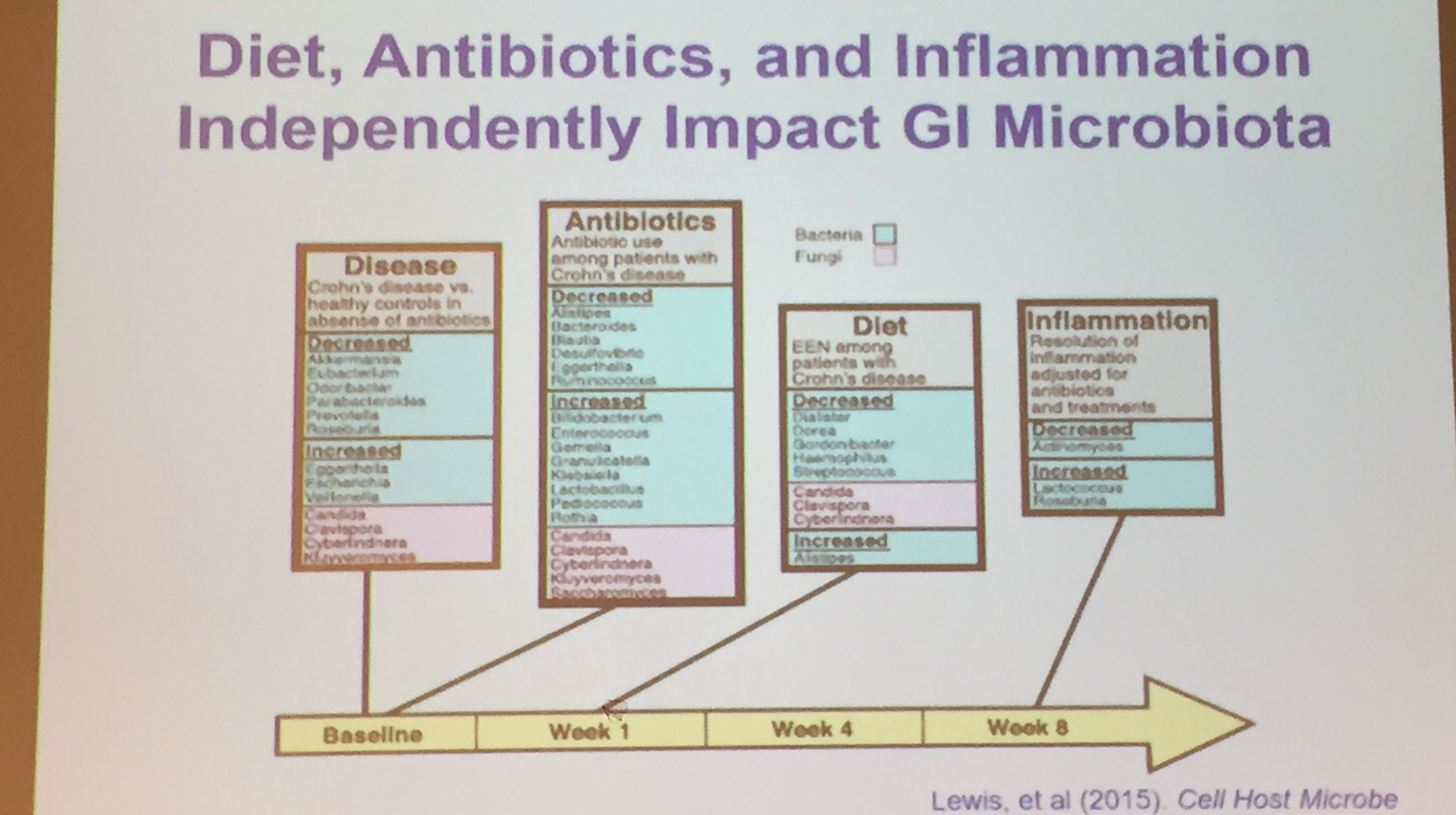
Diet in Inflammatory Bowel Disease: Food for Thought
This was a terrific lecture –though much of the topic has been reviewed recently in this blog: Dietary Therapy for Inflammatory Bowel Disease.
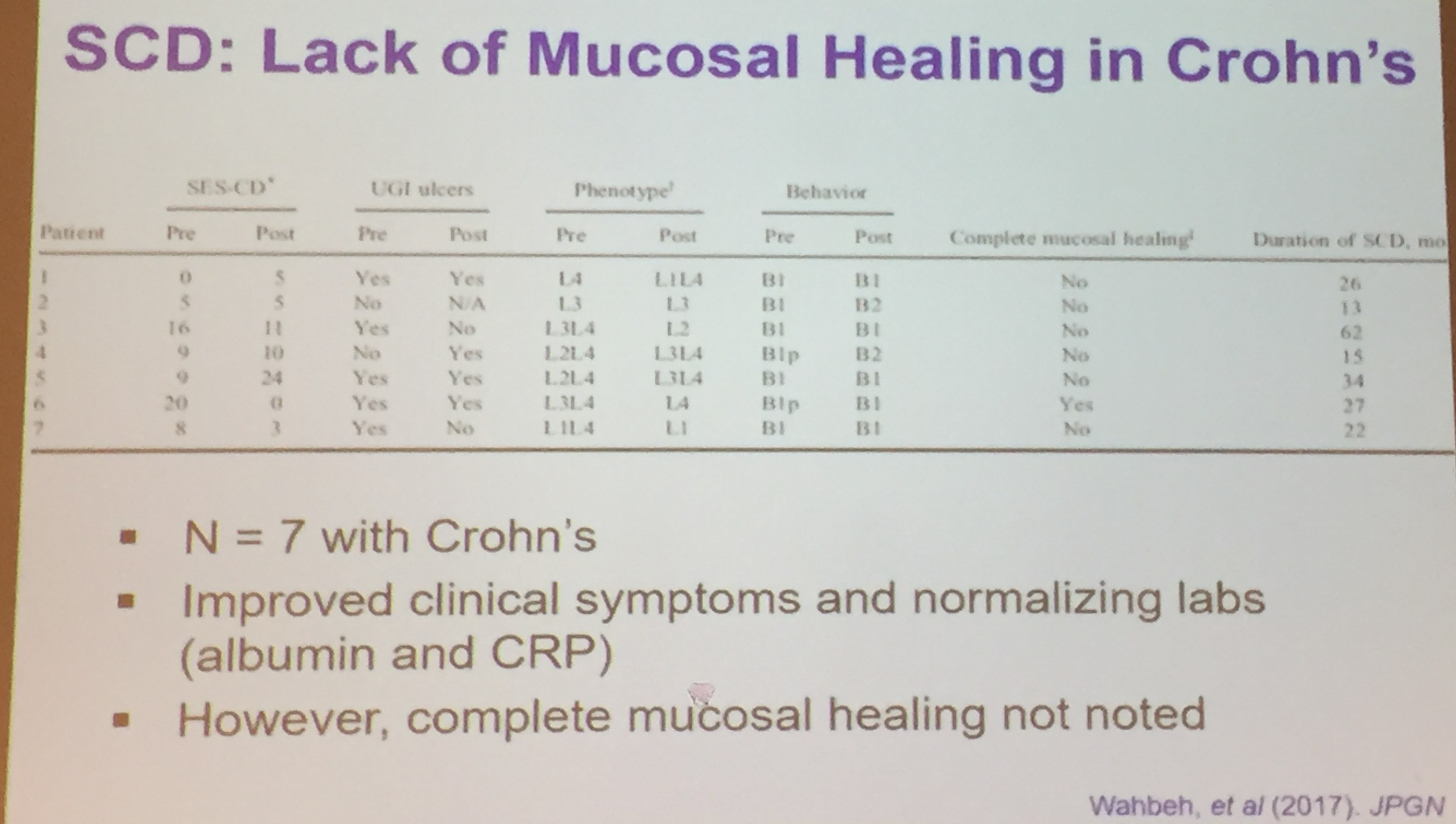
Key points:


Related blog posts:
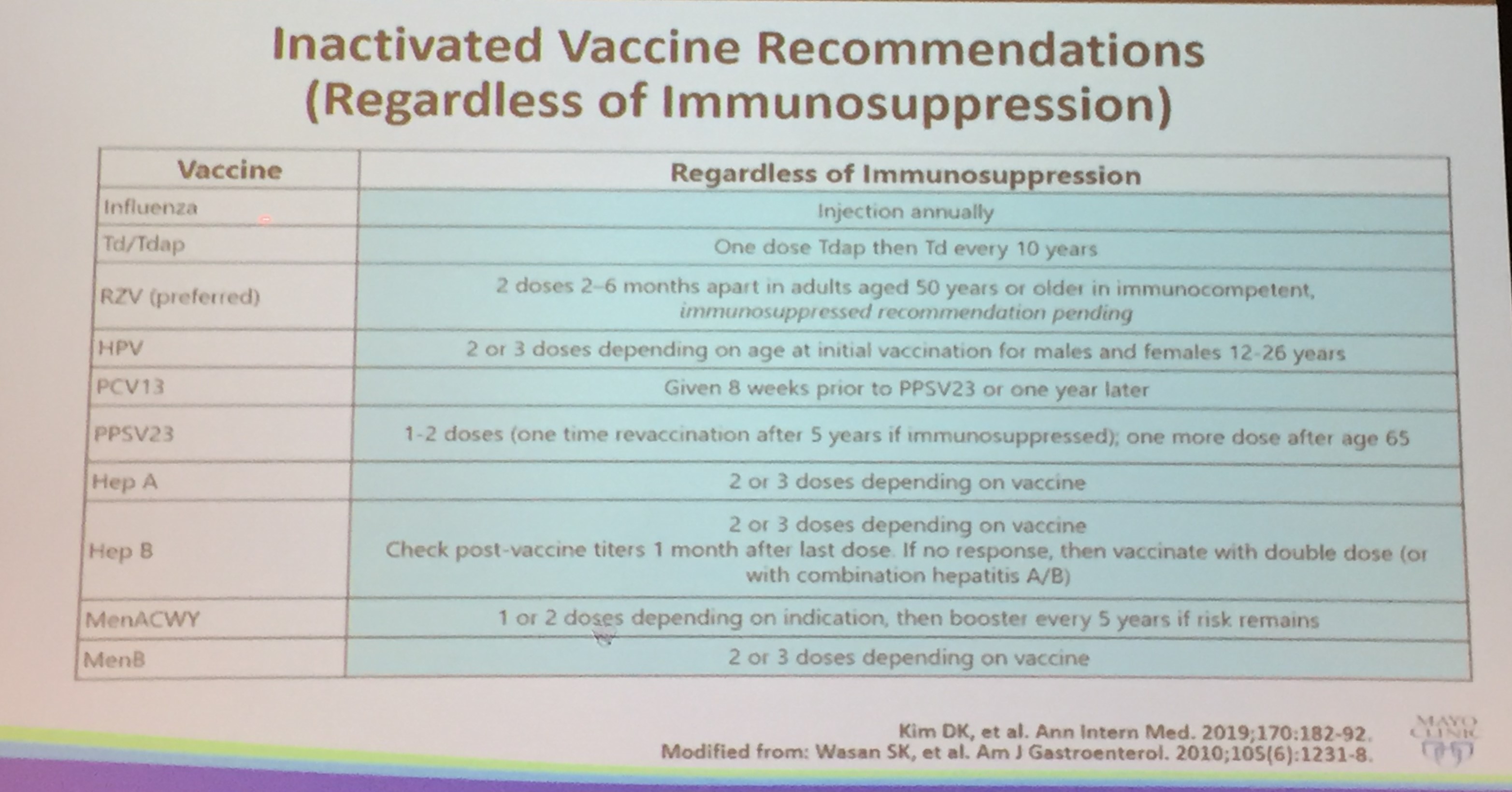
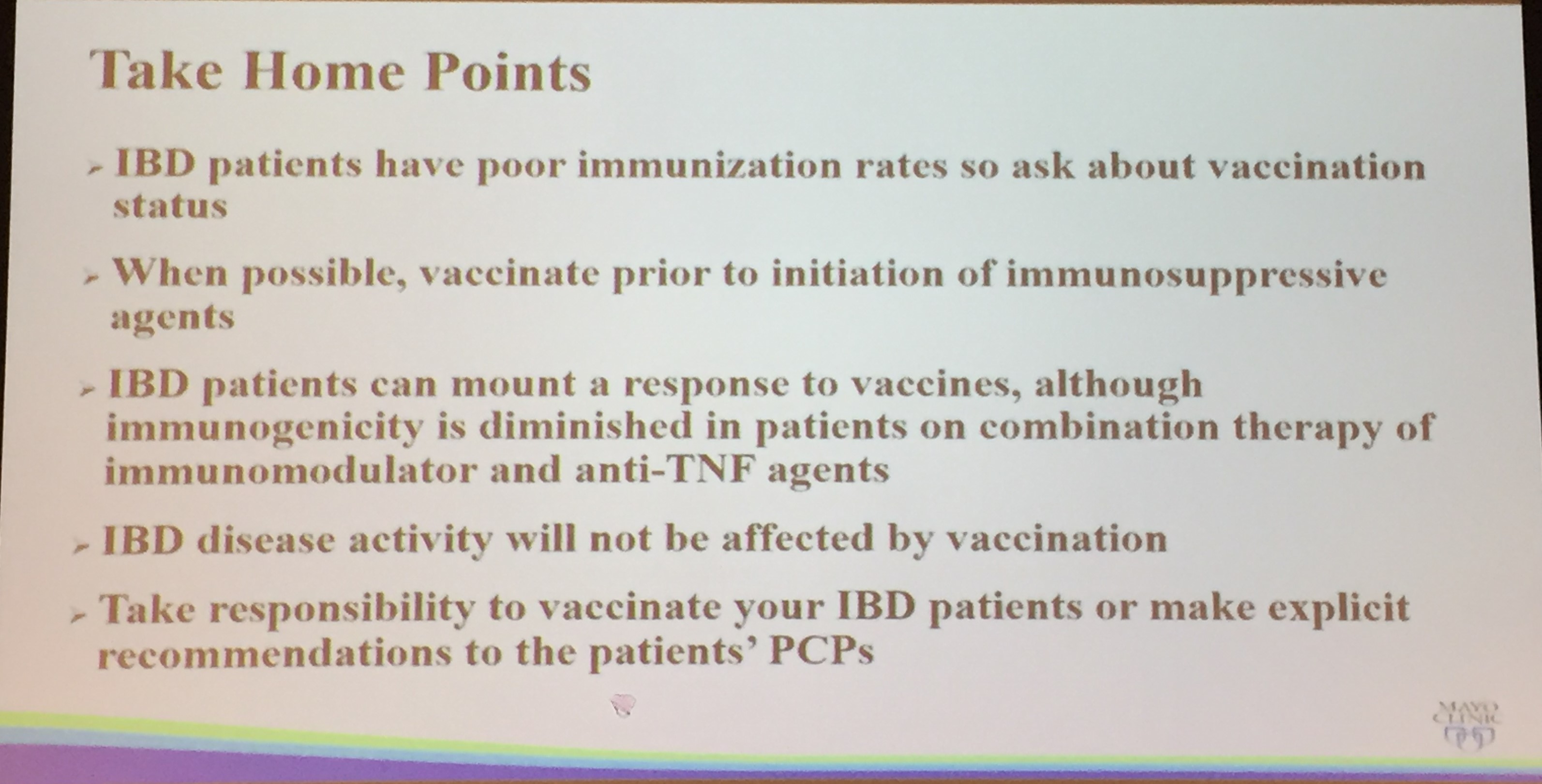
Frank Farraye, MD –Mayo Clinic
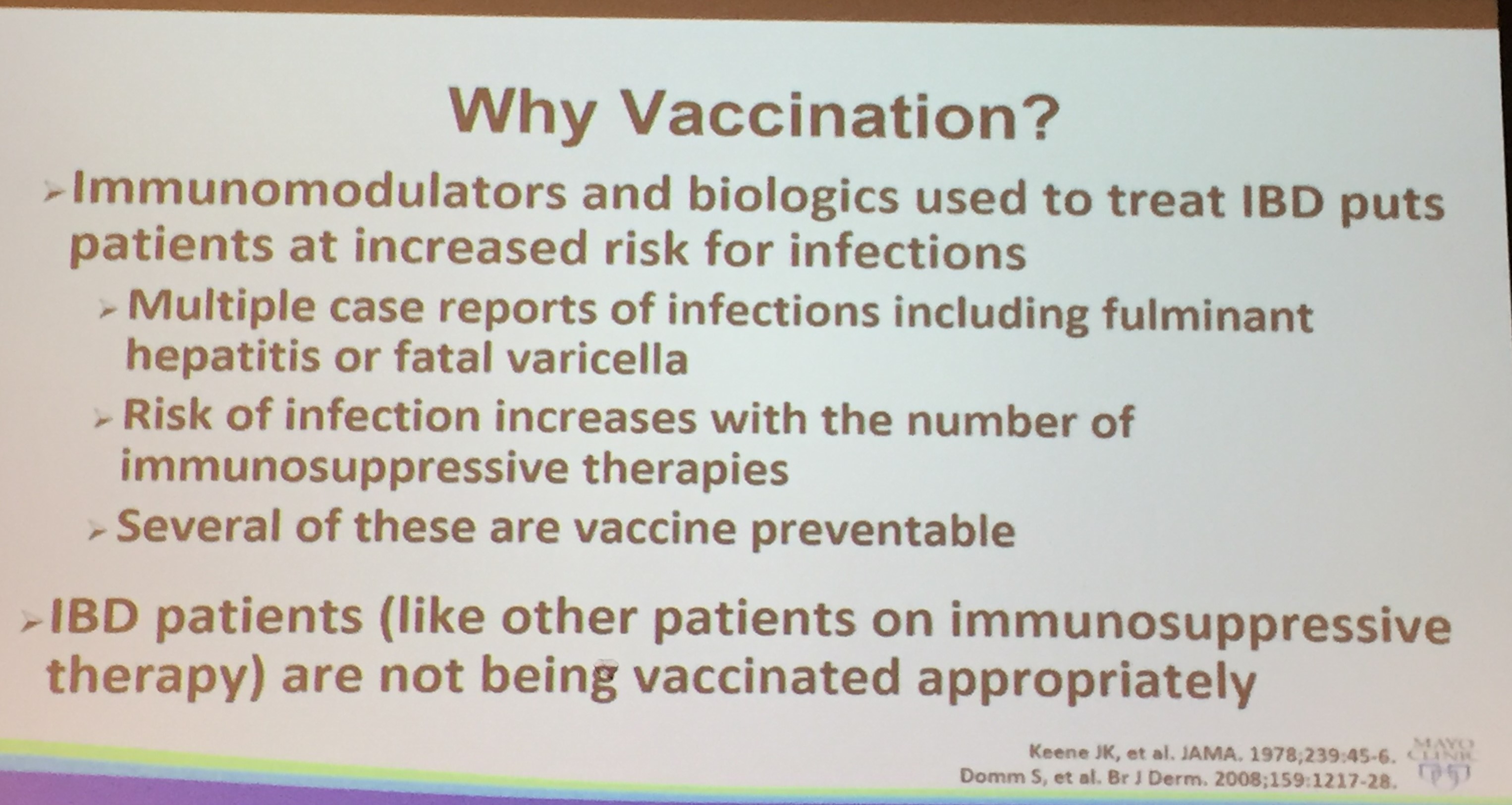
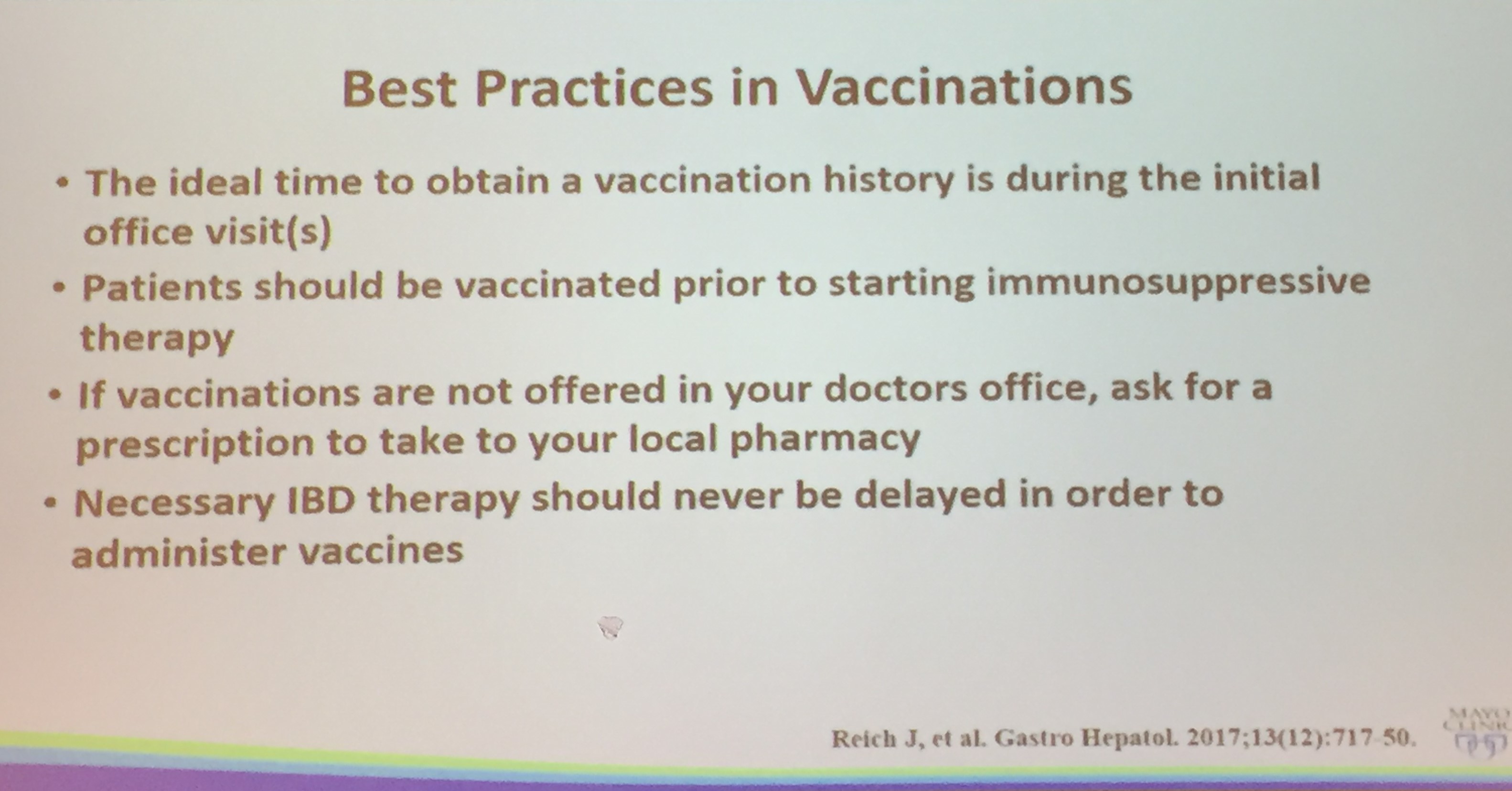
Health Maintenance in the Adult Patient with IBD
One audience member (Jeff Lewis, MD) pointed out that more attention needs to be paid to depression and anxiety which are much more common and more frequently health-threatening than issues like vaccination.
Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
My notes from a recent Georgia Chapter of CCFA’s conference. There could be errors of omission, transcription and/or errors in context based on my understanding.
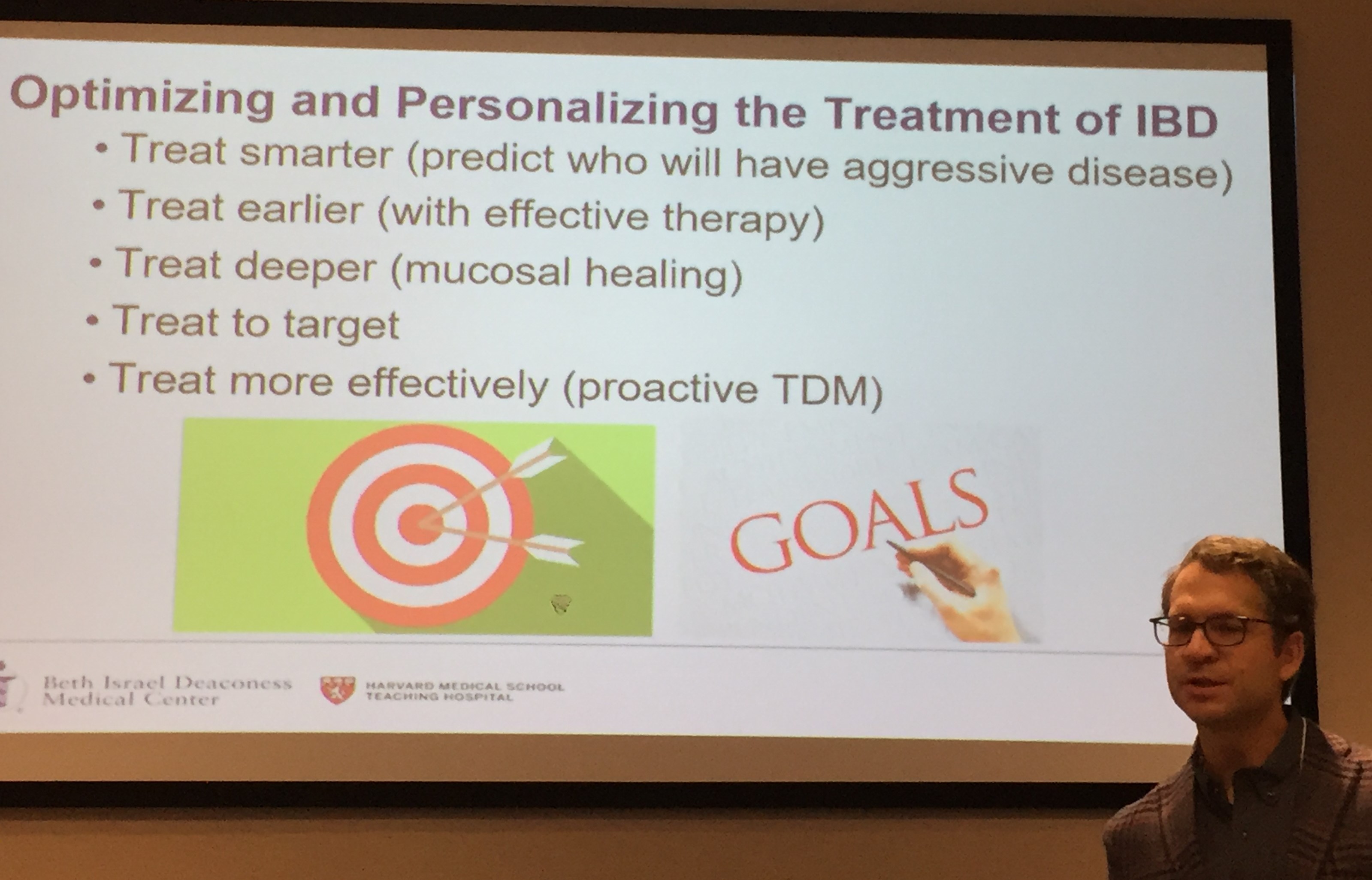
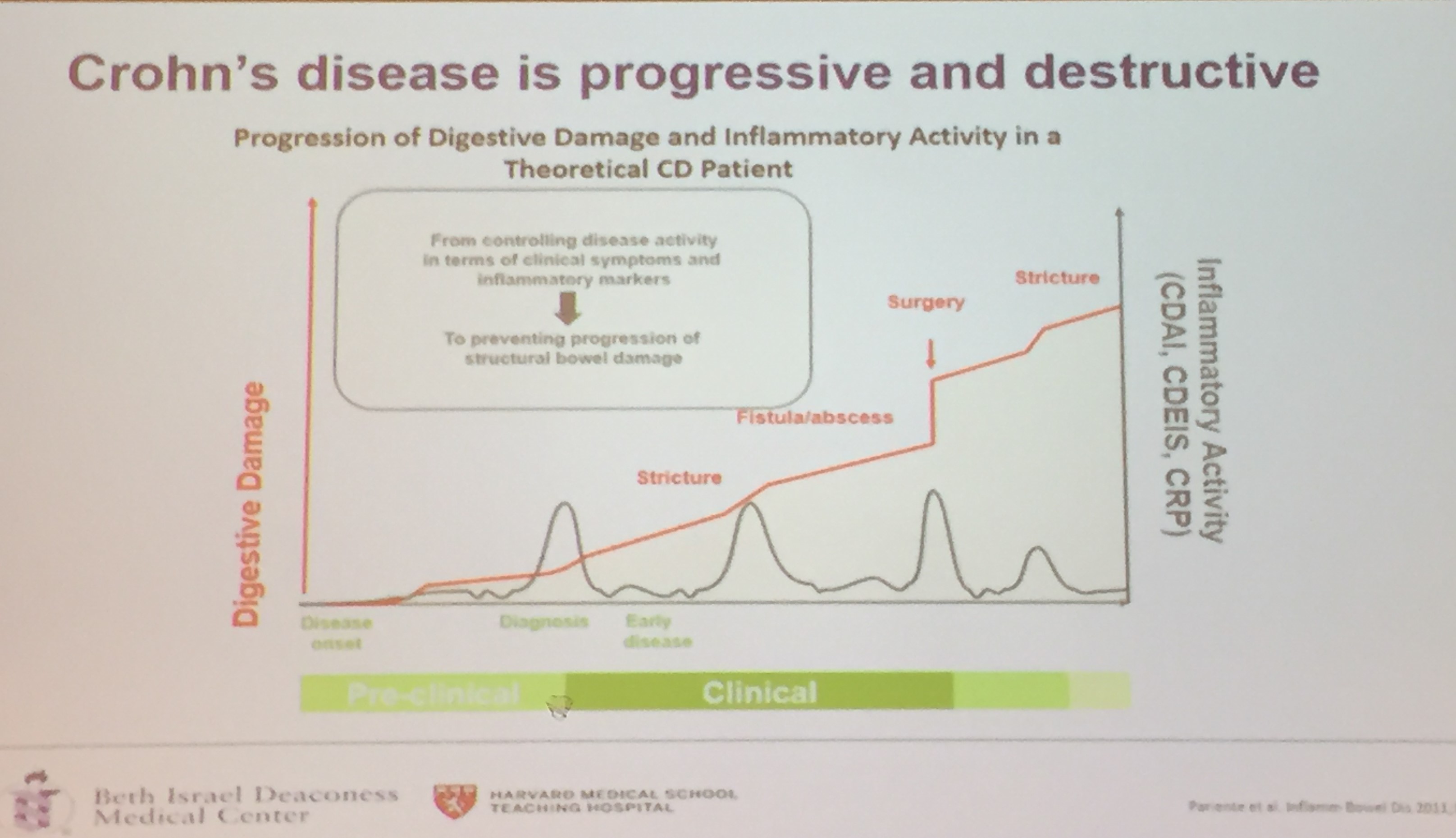
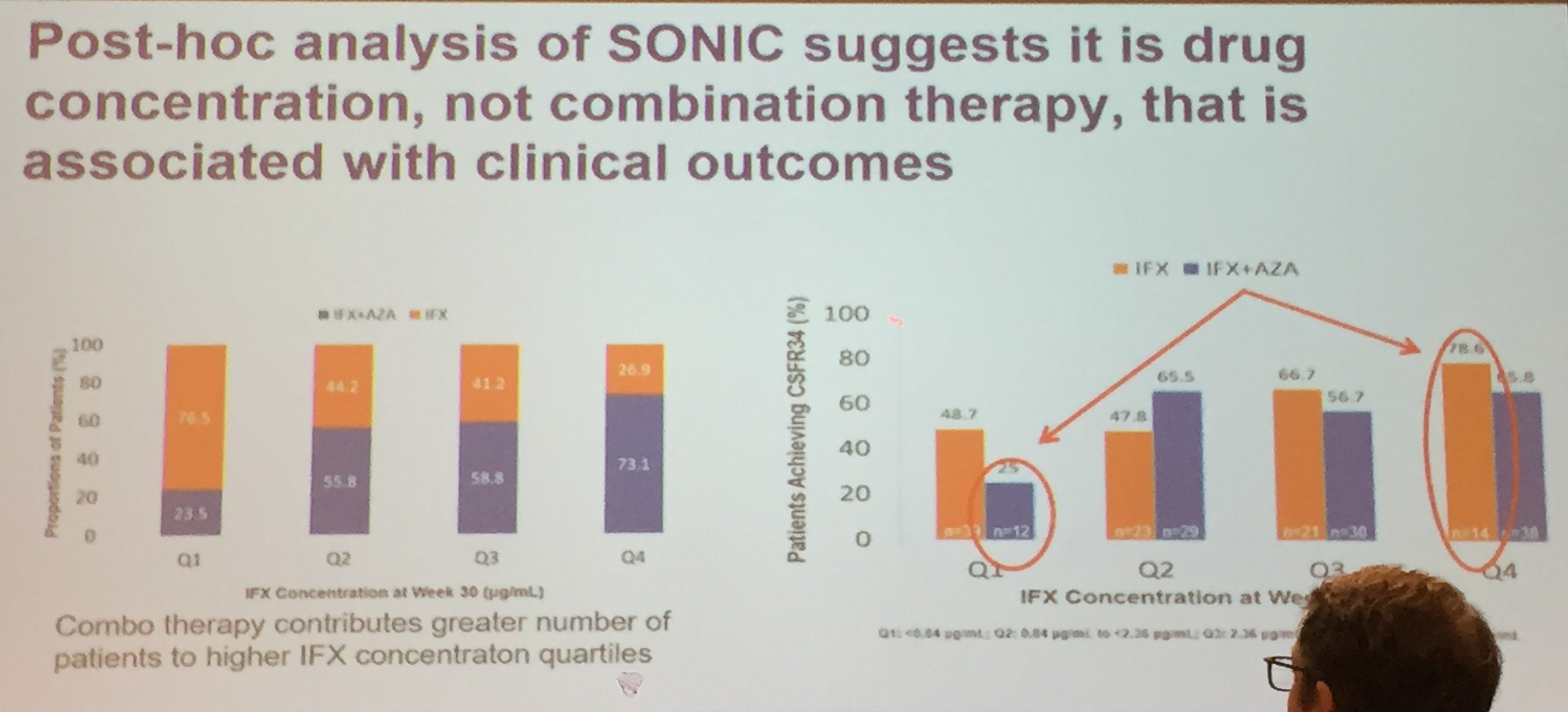
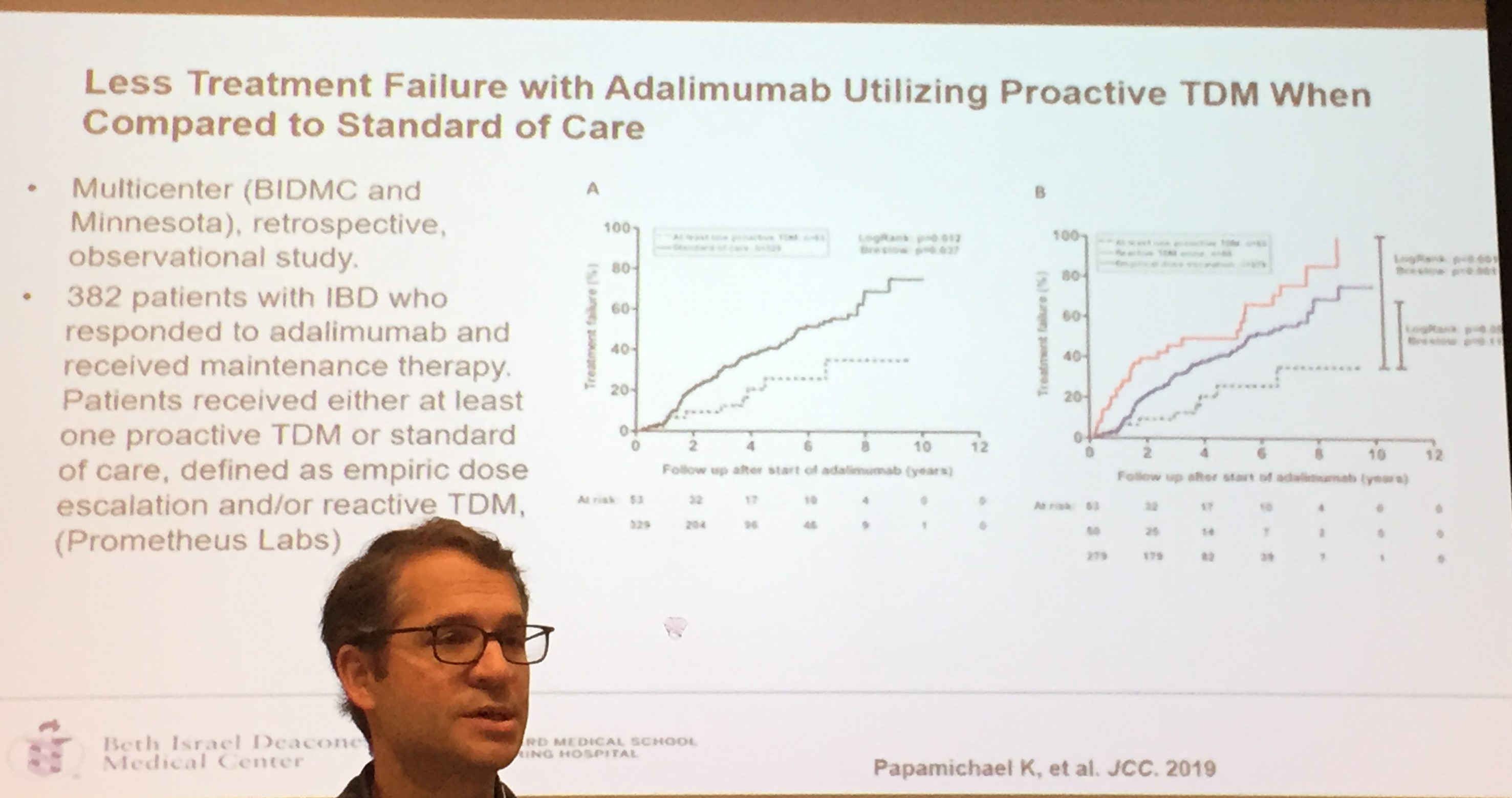
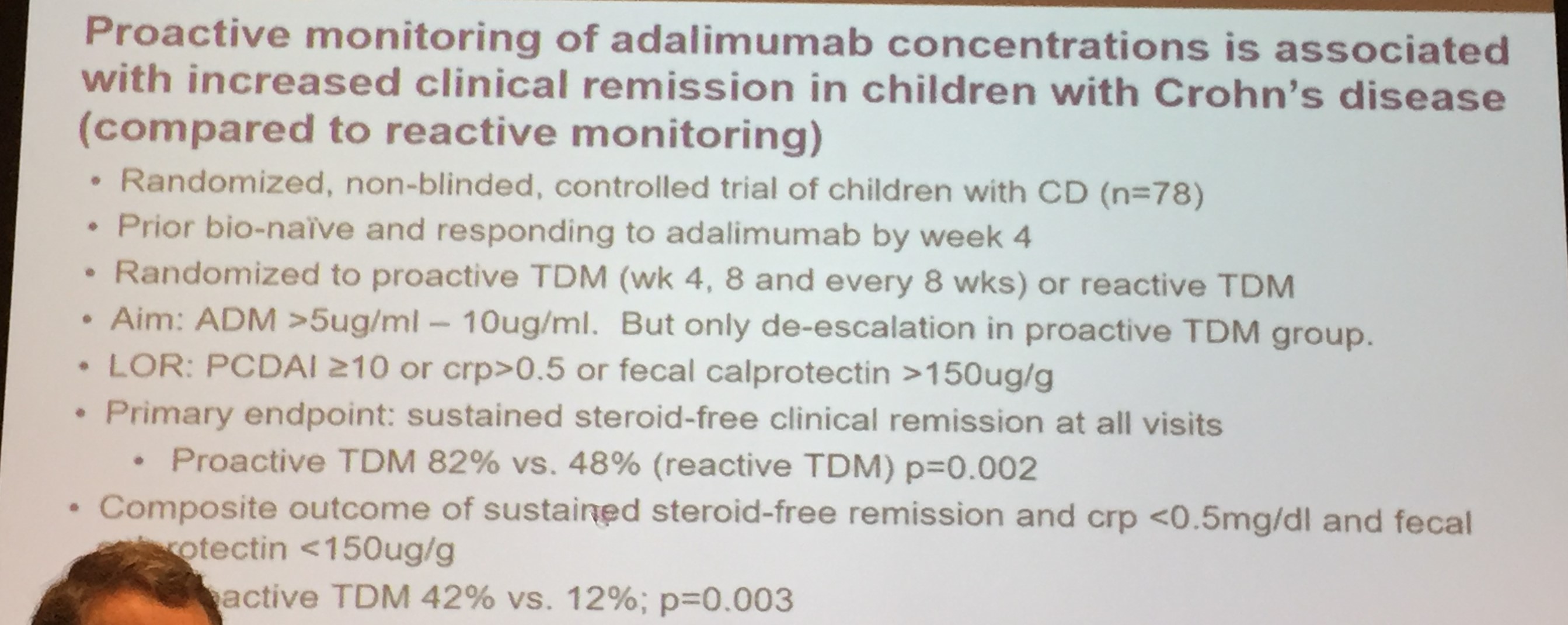
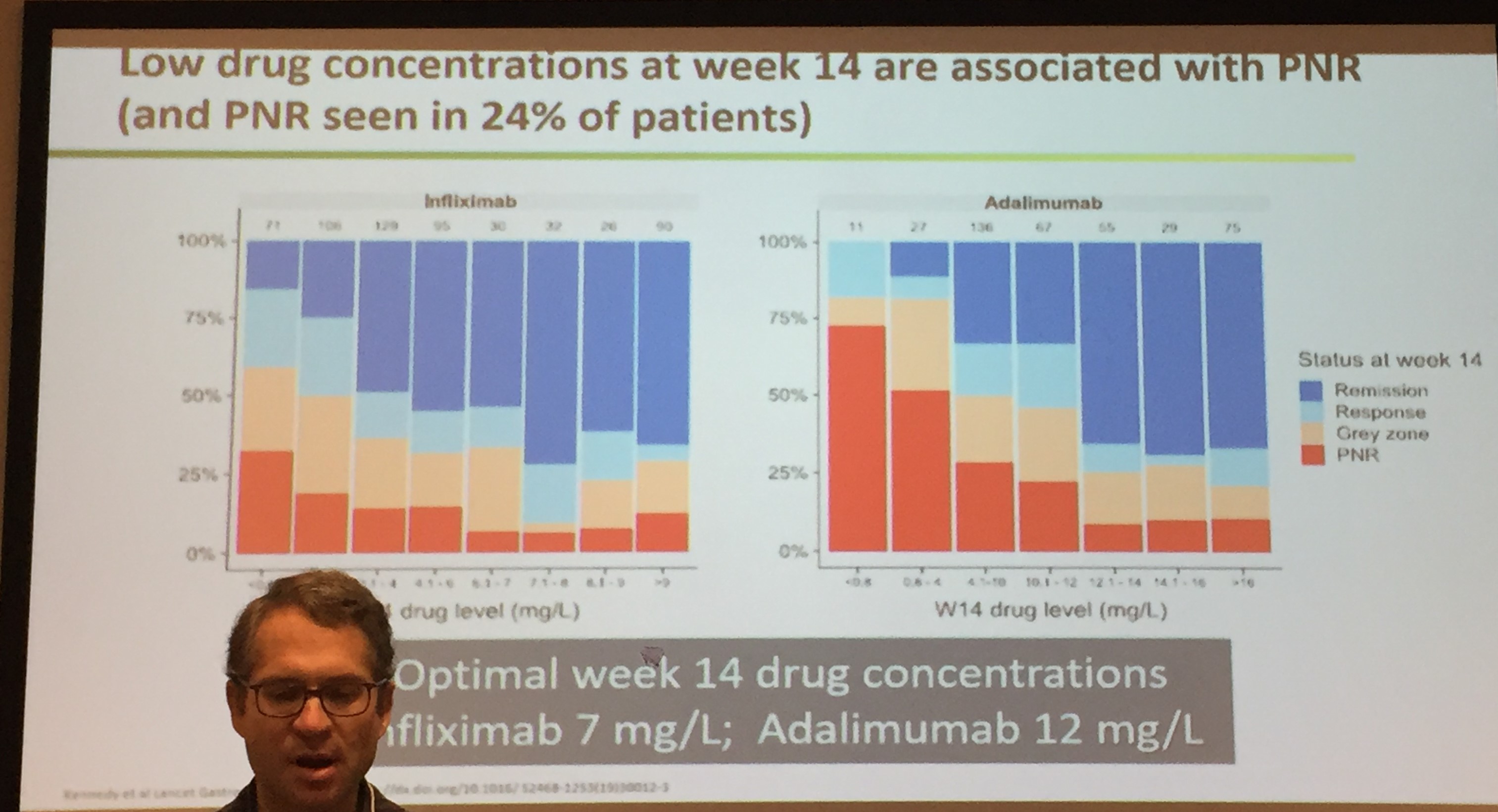
Adam Cheifetz, MD —Harvard School of Medicine
Optimizing IBD Treatments
Goals are clinical and endoscopic remission
Biologic Agents:
Therapeutic Drug Monitoring:

Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A recent study (LE Targownik, EI Benchimol, J Witt et al. Inflamm Bowel Dis 2019; 25: 1718-28) shows that direct health care costs are increased with anti-TNF therapy.
In this retrospective study using the Manitoba IBD Database, the authors examined the direct costs associated with anti-TNF therapy initiation in 928 patients (676 CD, 252 UC). Only 84 subjects were <18 years.
Key findings:
Discussion:
Limitations:
My take: This study shows that saving money is not the main reason to use anti-TNF therapies; rather, their effects on improved health and fewer complications.
Related blog posts:

Haystack Rock, Cannon Beach OR
Briefly noted:
D Piovani et al. Gastroenterol 2019; 157: 647-59. This study examined environmental risk factors for inflammatory bowel disease after extensive literature review and assessment of meta-analysis.
9 factors that were associated with increased risk of IBD:
7 factors that associated with reduced risk of IBD:
EL Barnes et al. Inflamm Bowel Dis 2019; 1474-80. In this review which identified 12 studies and 4843 with an IPAA ( ileal pouch-anal anastomosis) for ulcerative colitis, 10.3% were ultimately diagnosed with Crohn’s disease. Link to full text and video explanation: The Incidence and Definition of Crohn’s Disease of the Pouch: A Systematic Review and Meta-analysis
EV Loftus et al. Inflamm Bowel Dis 2019; 1522-31. In this study with 2057 adalimumab-naive patients, “the proportion of patients in HBI remission increased from 29% (573 of 1969; baseline) to 68% (900 of 1331; year 1) and 75% (625 of 831; year 6). Patients stratified by baseline immunomodulator use had similar HBI remission rates.” Full text: Adalimumab Effectiveness Up to Six Years in Adalimumab-naïve Patients with Crohn’s Disease: Results of the PYRAMID Registry
The following study was summarized in previous blog: Oral Antibiotics For Refractory Inflammatory Bowel Disease Full text link: Efficacy of Combination Antibiotic Therapy for Refractory Pediatric Inflammatory Bowel Disease

Washington Park, Portland, OR
Briefly noted: NE Burr et al. Clin Gastroenterol Hepatol 2019; 17: 2042-49.
In a retrospective cohort (1994-2013) using a primary care database from England, the authors identified decreasing risk of surgeries with Crohn’s diseae (CD).
The reasons for this reduction are not certain but could include better clinical care or reduction in other risk factors (like smoking).

Atlanta Botanical Garden
A landmark study (BE Sands et al. NEJM 2019; 381: 1201-14) shows that ustekinumab (Stelara) can be an effective therapy for moderate-to-severe ulcerative colitis (UC); it is already an approved, established therapy for Crohn’s disease. This randomized placebo-controlled study included an 8-week induction trial (n=961) followed by a 44-week maintenance trial (n=523) for patients with response.
Clinical remission was defined as a total socre of ≤2 on the Mayo scale (range 0-12) and no subscore >11 on any of the four Mayo scale components.
Key findings:
In terms of dosing, the authors note that there was greater improvement in calprotectin values during induction in the group who received 6 mg/kg compared to those who received 130 mg. At week 44, using more objective and stringent end points (eg. endoscopic improvement), greater clinical benefit was observed with the every 8 week regimen.
Visual abstract from NEJM Twitter Feed:

The following image depicts patients response during the maintenance phase –the lightest color is placebo, followed by every 8 weeks, and then the darkest color is every 12 weeks. The x-axis measures (left to right) are clinical remission, maintenance of clinical response at week 44, endoscopic improvement, corticosteroid-free remission, and remission at 44 weeks in those with remission after induction.
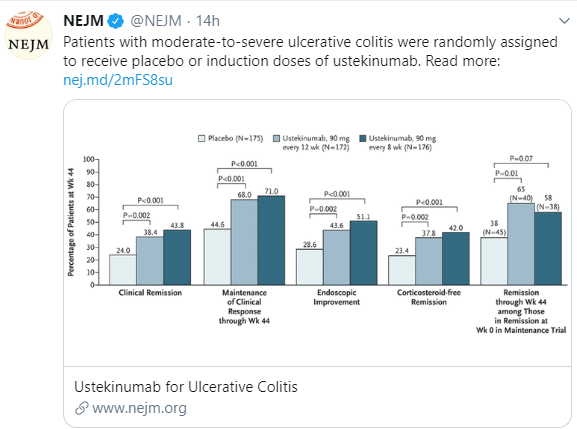
My take: Ustekinumab is more effective for placebo in patients with ulcerative colitis. More experience is needed to understand its long-term safety.
Related blog posts:
S Olivia et al (including Stanley Cohen from GI Care for Kids) Clin Gastroenterol Hepatol 2019; 17: 2060-7. “A Treat to Target Strategy Using Panenteric Capsule Endoscopy in Pediatric Patients with Crohn’s Disease” In this prospective study with 48 children with Crohn’s disease, pan-enteric capsule endoscopy (PCE) detected inflammation in 34 (71%) at baseline, 22 (46%) at week 24, and 18 (39%) at week 52. PCE results were used to manage treatment and resulted in change in therapy in 71% at baseline and 23% at week 24. Furthermore, PCE increased the proportions of patients in deep remission, up to 58% at week 52.
M Wright, et al. J Pediatr 2019; 210: 220-5. This case report of a 4 year-old boy with a perianal abscess and granulomatous colitis identified a NCF4 mutation causing severe neutrophil dysfunction. He developed osteomyelitis with anti-TNF therapy and did not respond to vedolizumab. He had an excellent outcome following a hematopoietic stem cell transplantation. This study reinforces the potential benefit of investigating VEO-IBD which could allow more targeted therapy. Related blog post: Patterns and Puzzles with Very Early Onset Inflammatory Bowel Disease
P Zapater et al. Inflamm Bowel Dis 2019; 25: 1357-66. This study with 112 patients with Crohn’s disease showed that serum interleukin-10 levels were directly related to infliximab and adalimumab levels. This suggests that serum anti-TNF levels are significantly influenced by immunological activation.
JE Axelrad et al. Clin Gastroenterol Hepatol 2019; 17: 1311-22. This study, using the Swedish National Patient Register, showed that gastrointestinal infection increased the odds of developing IBD in a nationwide case-control study. “Of the patients with IBD, 3105 (7%) had a record of previous gastroenteritis compared with 17,685 control subjects (4.1%). IBD cases had higher odds for an antecedent episode of gastrointestinal infection (aOR 1.64), bacterial gastrointestinal infection (aOR 2.02) and viral gastrointestinal infection (aOR 1.55)…a previous episode of gastroenteriitis remained associated with odds for IBD more than 10 years later (aOR 1.26).” The authors note that they cannot formally exclude misclassification bias, but it appears that enteric infections contribute to the development of IBD in susceptible individuals.

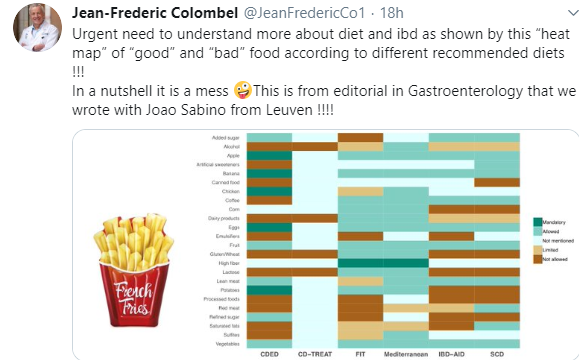
As noted in a previous blog (IBD Briefs August 2019), there have been numerous diets proposed to help with Crohn’s disease. The chart below illustrates the lack of any consensus.
Related blog posts: