D Patel et al. J Pediatr Gastroenterol Nutr. 2025;80:956–962. Efficacy of anal botulinum toxin injection in children with functional constipation
Methods: This was a retrospective, multicenter study including pediatric patients (n=63) who received anal botulinum toxin (BTX) for functional constipation (FC) refractory to medical therapy. Response to therapy was assessed based on improvement in weekly frequency of BM (bowel movements) to 3 or more per week and/or resolution of functional incontinence (FI)
Key findings:
- There was a a response rate of 10% in group 1 (FC +FI), 50% in group 2 (only FC) and 14% in group 3 (only FI); the an overall symptom resolution in 21% of patients
- Fecal incontinence was the most common side effect, reported in 11% of all patients
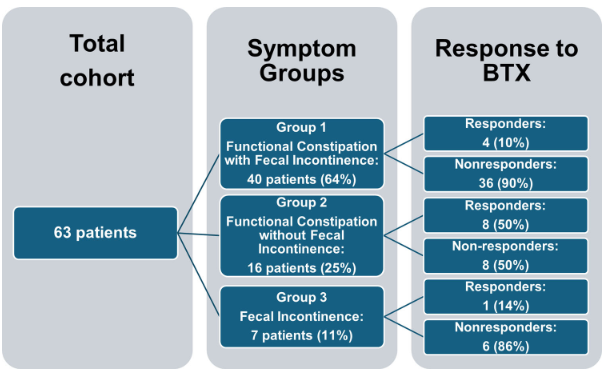
My take: In this highly-selected refractory population, there was a poor response to BTX in those with fecal incontinence (groups 1 and 3). The results should be interpreted with caution due to the retrospective nature of the study and the a lack of a control group.
Related blog posts:
- Position Paper: Pediatric Refractory Constipation Management (2025). “There is no clear role of anal botox in the treatment of patients with RC without a diagnosis of IAS achalasia”
- NASPGHAN Postgraduate Course 2017 (Part 5): Refractory constipation, Extraesophageal GERD, POTS, Recurrent Abdominal Pain
- Refractory Constipation -Terrific Update (2015)
- ANMS Virtual Symposia on Constipation
- Pictographic Constipation Action Plan
- New Data on Bisacodyl for Pediatric Constipation
- Safety of Senna-Based Laxatives
- Constipation Action Plan: Better Instructions, Fewer Phone Calls
- Does It Make Sense to Look for Celiac Disease in Children with Functional Constipation?
- You Can Do Anorectal Manometry in Your Sleep, But Should You?
- More than Two Years of Constipation Before Specialty Help
- Is There a Residual Impact of a Tethered Cord on Colonic Motility
- AGA Constipation Guidelines
- Radiographs and Constipation -Bad Practice and Good Study
- Quality Improvement: Fewer Xrays for Constipation
- Long Term Use of Polyethylene Glycol (PEG 3350)
- Is It a ‘Waste’ to Do Colonic Manometry in Kids with Autism?
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.