A recent terrific review article (H Bashaw et al. JPEN 2020; https://doi.org/10.1002/jpen.1738) provides a good advice on nutritional therapy for eosinophilic esophagitis (Thanks to Kipp Ellsworth for sharing this reference).
Full text: Tutorial: Nutrition Therapy in Eosinophilic Esophagitis—Outcomes and Deficiencies
An excerpt:
- “Diet elimination addresses the root cause of inflammation, treats EoE by removing the underlying trigger(s) of inflammation, and is a preferred approach for many patients… A registered dietitian is essential to ensure adequate macronutrients and micronutrients are present in the diet and to educate families in learning to read labels and prevent contamination.”
- ” Each type of elimination diet is associated with inherent nutrition risks.” Table 1 lists the potential nutrient deficiencies with each diet.
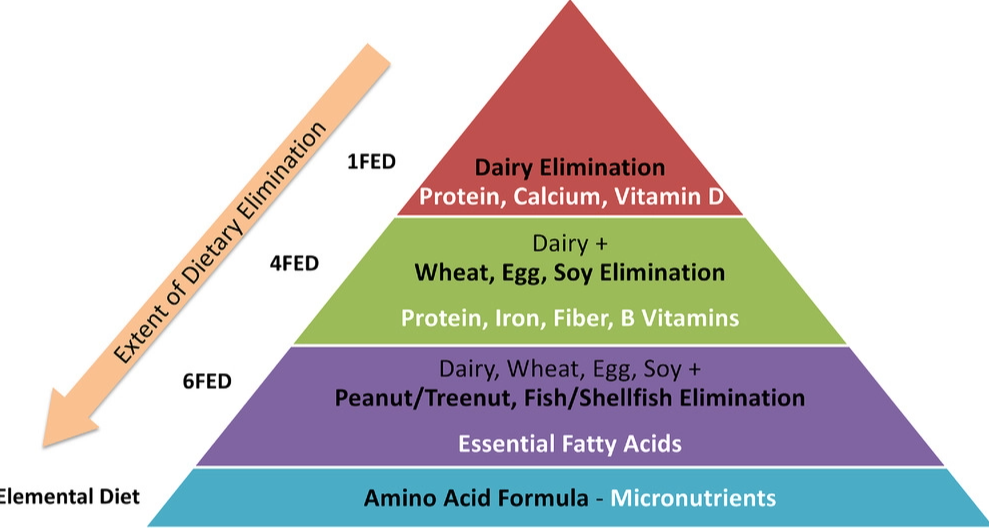
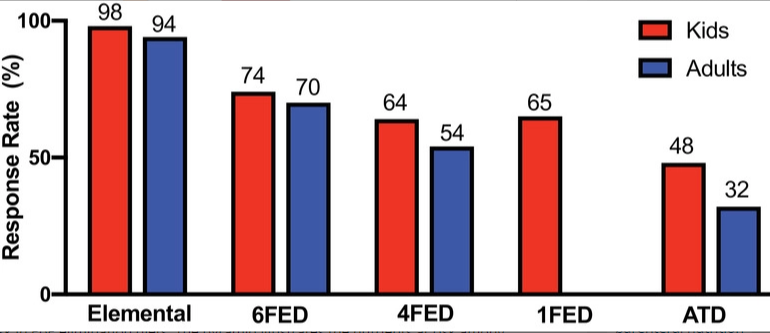
While the response rate is lower with fewer food group elimination, “the benefits of eliminating fewer foods from the diet include improved adherence, greater dietary variety, and a shorter time frame for reintroduction, with fewer endoscopies needed to identify triggers”
My take: As with topical steroids and PPI treatment, dietary treatment for EoE has to be maintained to be effective. Concerns for adherence with medications are applicable for dietary therapy as well.
Related blog posts:
- 2020 Eosinophilic Guidelines (AGA)
- Changing the Dietary Approach for EoE
- New Therapy for EoE (2020)
- Could Immunotherapy (EPIT) Work For Eosinophilic Esophagitis? & Coronavirus Up-to-Date Tally
- Grading Treatment Response in Eosinophilic Esophagitis | gutsandgrowth
- Four-food group elimination diet | gutsandgrowth
- Diet and Stress in Pediatric Eosinophilic Esophagitis
- Useful information on EoE Dietary Therapies
- Eosinophilic Esophagitis -Six Food Group Diet
- Systemic Review of Dietary Treatments for Eosinophilic …
- What is the Role for Allergy Testing in Eosinophilic …
- Orodispensable Budesonide Tablets for Eosinophilic Esophagitis | gutsandgrowth
- Head-to-Head: Budesonide vs Fluticasone for Eosinophilic Esophagitis | gutsandgrowth
- What Happens When Topical Steroids Are Stopped in Eosinophilic Esophagitis
- Neglibible Effect of Eosinophilic Esophagitis Treatment on Longitudinal Growth
- What is EoE?
- EoE Update 2018 (Dr. Seth Marcus)
- Updated Consensus Guidelines for Eosinophilic Esophagitis