A supplement in Gastroenterology (2017; 152: 309-462) provides a great update on a lot of topics. These include pathophysiology articles (eg. role of Paneth cell, role of microbiome), treatment/development of fibrosis, management advances in endoscopy and biomarkers, newest treatments and emerging treatments, complementary medicine approaches, pain/psychology issues, medications in pregnancy, and detecting dysplasia.
For me, the update on epidemiology and its relationship to diet (pgs 313-321) as well as the review on diet as a trigger or therapy for inflammatory bowel disease (398-414) were most interesting. Though, I will keep the update on complementary and alternative medicines article at my desk in case questions come about this topic
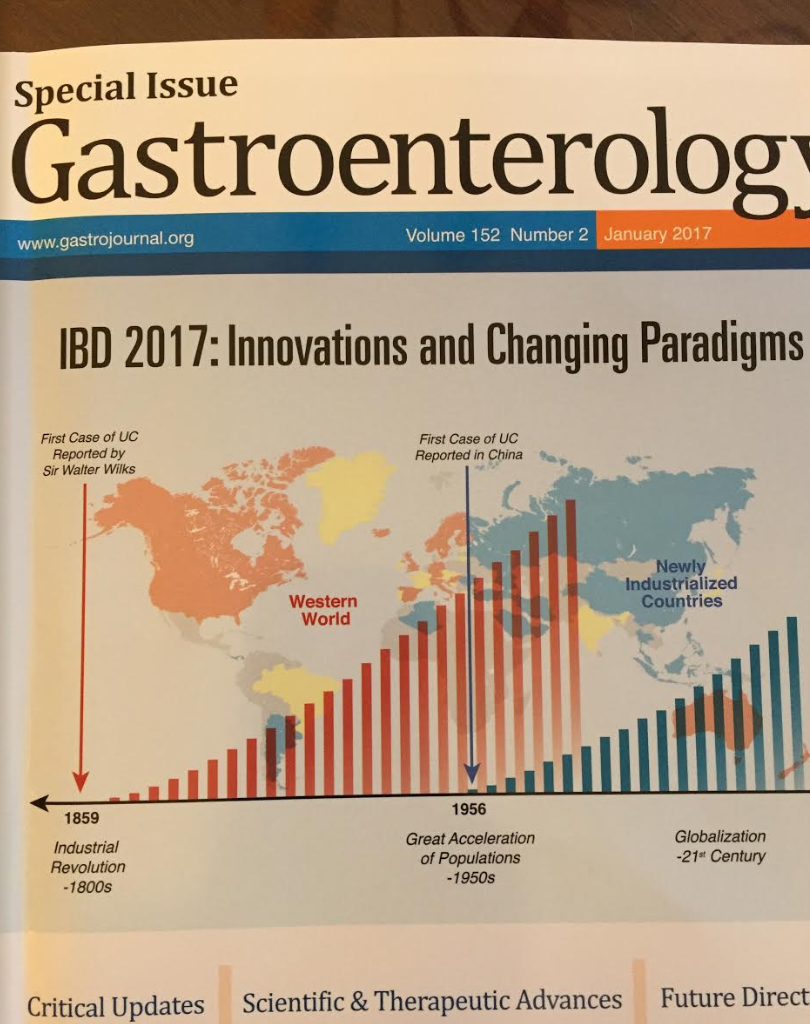
GG Kaplan, SC Ng. “Understanding and Preventing the Global Increase of Inflammatory Bowel Disease” Gastroenterology 2017; 152: 313-321
Epidemiology:
1st case of ulcerative colitis was reported in 1859. !st cases of Crohn’s disease reported in 1932 (BB Crohn et al. JAMA 1932; 99: 1323-29).
Olmstead County, Minnesota –cases per 100,000:
- 1965: 28
- 1980: 90.5
- 1991: 132.7
- 2001: 213.9
- 2011: 246.7
While rates of IBD have “shown signs of stabilization…pediatric-onset IBD continues to increase steadily in incidence.”
IBD Around the World –cases per 100,000:
- 2005 Japan: 76
- 2005 S Korea: 42
- 2013 India: 9.3
- 2013 China: 3.3. The greatest incidence is noted in areas of increased urbanization and economic advancement.
- 2005: Brazil: 9.7
Environmental factors/associations:
- Cigarette smoking –increases risk of Crohn’s disease in Western countries, and has protective effect against Ulcerative colitis
- Antibiotic use –increases risk of IBD in Western countries, but may be protective in developing countries. “Antibiotic-induced dysbiosis may not develop as easily in developing countries, owing to ubiquitous exposure to a diverse range of microbiota that rapidly repopulate the intestinal tract.”
- Breastfeeding –protects against developing IBD
- Vitamin D –low levels increase risk of IBD in Caucasians.
- Fiber –a “diet high in fiber protects against Crohn’s disease.”

JD Lewis, MT Abreu.”Diet as a Trigger or Therapy for Inflammatory Bowel Disease” Gastroenterology 2017; 152: 398-414.
“The most common question asked by patient is …’Doctor, what should I eat?'”
Key points:
- Data from studies of immigrants to higher-IBD prevalence countries show an increasing incidence of IBD, leading to the hypothesis that environmental factors such as diet affect risk of IBD.
- In early life, breast milk, in some but not all studies, has been associated with a lower risk of childhood-onset IBD.
- Before development of IBD, studies have shown lower risk of IBD “among people who consume more fruits and vegetables, and a higher risk in people who consume less of these and more animal fats and sugar.”
- “There is little information about which foods induce flares.” However, for UC, “a high intake of meat, especially red and processed meat, protein, alcoholic beverages, sulfur, and sulfate increased the likelihood of a flare” based on food questionnaires. In patients with CD, diet with higher “total fat, saturated fat, monounsaturated fatty acids, and a higher ratio of omega-6:omega-3 PUFAs was associated with disease relapses.”
- “Only approximately half of patients have ever received advice from a dietitian.”
- Oral iron may trigger flares in a small percentage of patients with IBD. The authors note that adherent E coli express genes for iron acquisition and require iron for growth.
Specific Diets/Additives: Most of these diets have been discussed in previous posts, including:
Exclusive (and Partial) Enteral Nutrition:
- “The most widely studied dietary intervention.” It has been shown to be effective for CD. More elemental formulas have NOT been shown to be more effective. “EEN and PEN therapy is less likely to normalize fecal levels of calprotectin in children.”
- “Dietary therapy reduced inflammation and led to changes in the microbiome within 1 week. Unlike TNF antagonists, however, the changes to the microbiome induced by EEN did not lead to a microbiome resembling that of healthy individuals.”
Specific Carbohydrate Diet (SCD):
- This diet has been studied in small populations. Suskind et al reported SCD effectiveness “in 7 children with CD…showed that fecal calprotectin level decreased from a mean of 685 mcg/g to 213 mcg/g at 2-6 after starting the diet.” “Cohen et al used video capsule endoscopy…in 10 children with CD…Four of 10 children achieved complete mucosal healing (Lewis score <135) and 6 of 10 children achieved clinical remission.”
Low FODMAP diet:
- While the diet may induce symptom improvement, there is no “evidence that a low FODMAP diet reduces inflammation.”
Vitamin D supplementation:
- “Vitamin D has multiple potential beneficial effects on intestinal inflammation.” The authors review studies that report lower risk of CD in patients with higher vitamin D levels and on the reduction in relapse in a study of CD patients who were in remission and treated with Vitamin D (1200 IU daily)
Curcumin supplementation:
- The authors review two small studies which suggested that curcumin for patients with ulcerative colitis increased clinical remission (when used with mesalamine)
The overall advice the authors give is that patients “should be advised to eat a well-balanced diet, such as the Mediterranean-style diet, avoiding processed foods or foods that they self-identify as worsening their symptoms. Patients who are committed to attempting to manage their disease predominantly through dietary modification should be counseled about the importance of assessing for resolution of inflammation in addition to symptoms.”
Other Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.