E Crawford et al. JPGN Reports 2021; 22 – Issue 4 – p e129. Open Access: Association of Fecal Calprotectin With Endoscopic and Histologic Activity in Pediatric Inflammatory Bowel Disease
This retrospective study used data from 331 patients (n=107 with IBD). Fecal calprotectin (FC) was done between 30 days and 1 day before colonoscopy.
Key findings:
- Correlation with endoscopy: median FC was lowest for all IBD patients with no active disease (181 μg/g) and highest in severe disease (921 μg/g), with significant difference between no disease and moderate and severe disease (P = 0.019, 0.003), and between mild and severe disease (P = 0.012)
- Correlation with histology: median FC was lowest with no active disease (328 μg/g) and highest in severe disease (895 μg/g), with significant difference between no disease and moderate and severe disease (P = 0.021, 0.018)
- The control population had median FC of 35.5 compared to 181 μg/g for the IBD population in endoscopic remission (P = 0.018).
My take: Calprotectin levels are particularly helpful as a screen for IBD (probably using threshold of at least 120) and its use to monitor clinical response. This study shows it has some utility in predicting disease severity.
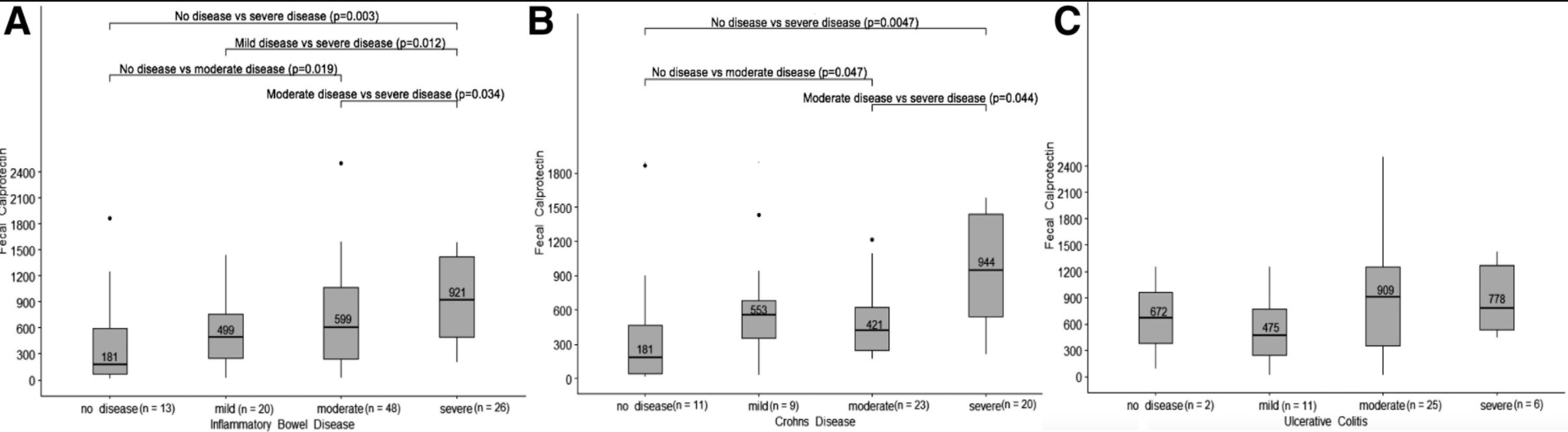
(A), Crohn’s disease (B) and ulcerative colitis (C). IBD = inflammatory bowel disease.