“Red Man” syndrome “calls up historical narratives that endorse and reinforce discrimination against Native American and Indigenous peoples”
Vancomycin infusion reactions are more readily documented in white males than in females and black patients. The combination of rash, itching, flushing and hives may be less apparent in some groups and/or mistaken as a true allergy.
“We recommend using the term “infusion reaction” for all non-immune-mediated drug reactions”
My take: I agree with the authors that the term “red man syndrome” should be dropped. It is both an insensitive term and also hinders appropriate diagnosis of vancomycin infusion reactions.
A recent political cartoon by Mike Lukovich had a caption/commentary on U.S. troops leaving Afghanistan: “Our times up here. We are being redeployed to a war zone.”
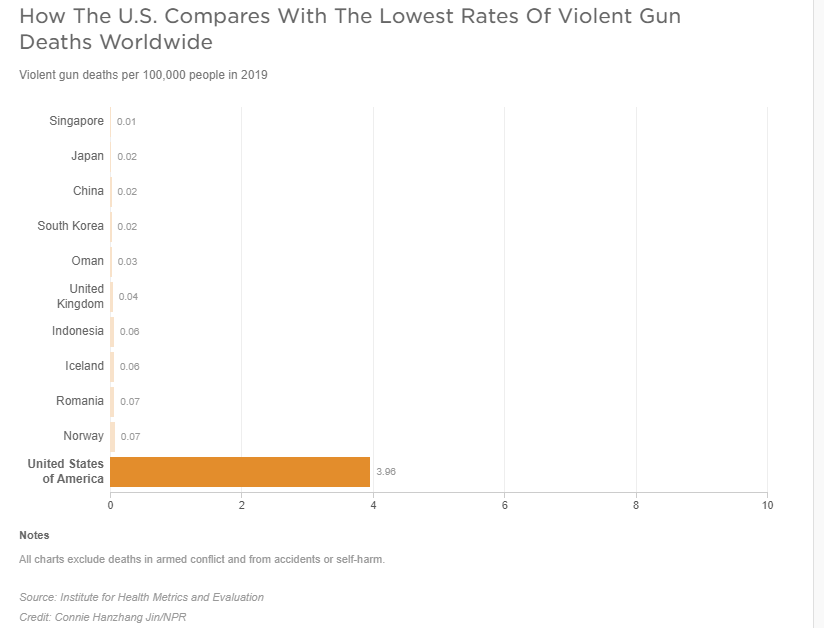
No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
A recent study by the APPETITE (Alberta Provincial Pediatric EnTeric Infection TEam) describes the frequency of abdominal pain with acute gastroenteritis (AGE).
This was a prospective cohort study with 2136 patients (median age 21 months) who were recruited from 2 pediatric EDs
Key findings:
In the 24 hours before enrollment, most caregivers reported moderate (28.6% [610/2136, 95% CI 26.7-30.5]) or severe (46.2% [986/2136, CI 44.0-48.3]) pain for their child.
In the ED, they reported moderate (31.1% [664/2136, 95% CI 29.1-33.1]) or severe ([26.7% [571/2136, 95% CI 24.9-28.7]) pain; analgesia was provided to 21.2% (452/2131). The most common analgesics used in the ED were acetaminophen and ibuprofen.
In their discussion, the authors note the need for research on the development of effective, safe, and timely pain management plans. In my view, all gut pain, especially in those with chronic conditions, needs more effective treatments.
My take: This is an interesting study as very little has been published about AGE and abdominal pain. The study’s conclusions are limited by the age of the participants.
In his book, Critical path, Buckminster Fuller (Fuller 1981), American architect, systems theorist, author, designer, inventor, and futurist, created the ‘knowledge doubling curve’. He noticed that until 1900 human knowledge doubled approximately every century and by the end of World War II knowledge was doubling every 25 years (Knowledge is not everything, Paul Chamberlain). Now the doubling of knowledge, in the age of the internet and social media, has become even shorter, perhaps less than a year.
I was thinking about this knowledge doubling curve after reading two practice guidances in a recent issue of Hepatology:
The first guidance is mainly for reference as pediatric gastroenterologists do not focus on reproductive health. The authors do provide guidance on contraceptive options which is an important topic for adolescents. The main guidance is disease-specific information for pregnancy in the setting of underlying liver conditions including liver transplantation, cirrhosis, viral hepatitis, autoimmune hepatitis, PSC, PBC, Wilson’s disease, hepatitis C, nonalcoholic fatty liver disease, HELLP, acute fatty liver disease of pregnancy, Budd-Chiari, FNH, hepatocellular adenoma, and others. The guidance also provides recommendations for how to evaluate abnormal liver tests in pregnancy and reviews liver medications during pregnancy (Table 4).
The second guidance reviews the following:
An overview of the current understanding of bleeding and thrombosis in cirrhosis.
An evidence‐based justification for bleeding risk assessment in patients with cirrhosis before invasive procedures, including current concepts in preprocedural testing and laboratory analysis and their role in predicting bleeding complications.
An outline of established and recently identified risk factors for venous thrombosis in the portal and hepatic venous systems in both patients with and without cirrhosis along with thrombophilia testing recommendations.
A review of the strengths and weaknesses of the various classification systems for portal vein thrombosis and a proposal for standard nomenclature regarding characterization of portal vein thrombosis location, time course, and progression.
Useful points:
In patients with cirrhosis, there are “complex hemostatic changes that are not adequately captured by traditional laboratory measures of hemostasis, such as PT, aPTT, and platelet count.”
“Because of conflicting data in the literature, there is no data-driven specific INR or platelet cut-off in which procedural bleeding risk is reliable increased.” In some studies, the authors conclude that “that the low platelet count may have been merely a reflection of advanced portal hypertension and not a causative risk factor for bleeding.”
For Platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count...An individualized approach to patients with severe thrombocytopenia before procedures is recommended because of the lack of definitive evidence for safety and efficacy of interventions intended to increase platelet counts in patients with cirrhosis.” The authors note in Table 4, that the AASLD does not have a specific threshold for platelets, whereas other societies have used values of >30 or >50.
For INR in setting of cirrhosis: “The INR should not be used to gauge procedural bleeding risk in patients with cirrhosis who are not taking vitamin K antagonists (VKAs)…Measures aimed at reducing the INR are not recommended before procedures in patients with cirrhosis who are not taking VKAs…FFP transfusion before procedures is associated with risks and no proven benefits.”
The guidance lists a step‐by‐step treatment and surveillance algorithm for portal vein thrombosis in patients with cirrhosis (and without cirrhosis).
The guidance provides updated diagnostic, treatment, and management recommendations for sinusoidal obstruction syndrome (formerly known as hepatic-veno-occlusive disease), hereditary hemorrhagic telangiectasia, and hepatic vein thrombosis (aka Budd-Chiari).
Classification and management recommendations for idiopathic noncirrhotic portal hypertension and the portosinusoidal vascular disorders.
Surveillance and evaluation recommendations for hepatic and splenic artery aneurysms.
A review of the management issues in vascular liver disorders specific to children and guidance on early intervention in extrahepatic portal vein obstruction in children.
My take: In essence, these two articles are condensed textbooks. The first on Liver Disease, Pregnancy and Reproductive Health. And the second on Bleeding in the Setting of Chronic Liver Disease and Vascular Liver Diseases.
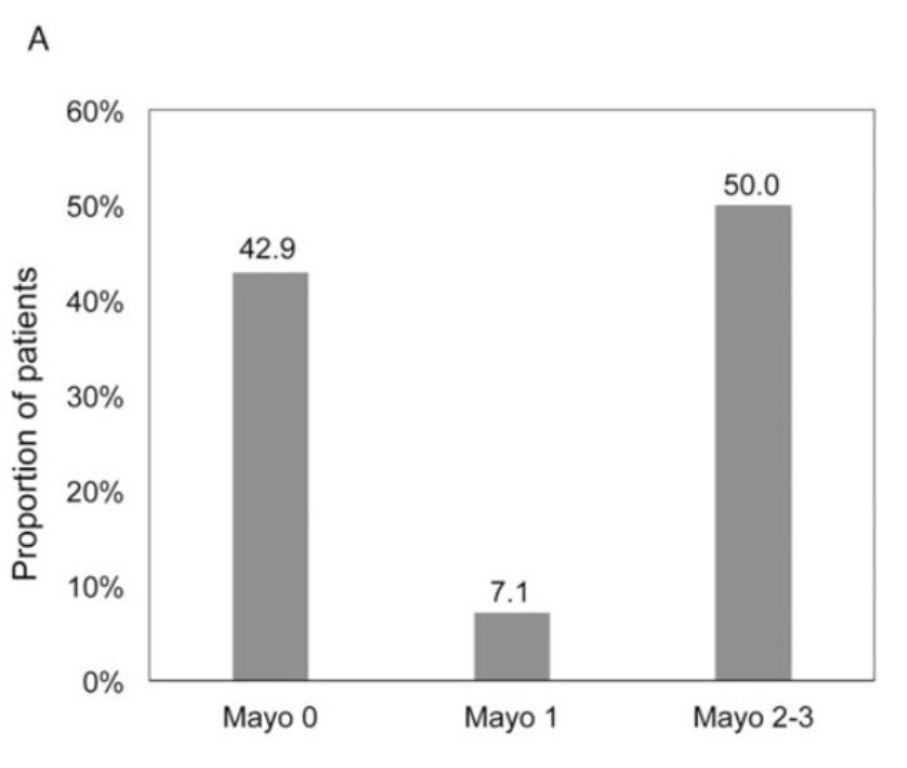
This study prospectively assessed for mucosal healing by endoscopy 3 to 5 months after clinical remission, PUCAI <10, was documented. Key findings:
28 children in continuous clinical remission at time of sigmoidoscopy were included. Mayo 0 was present in 12/28 (43%), Mayo 1 in 2/28 (7%) and Mayo 2 to 3 in 14/28 (50%) endoscopies.
Among 23 patients with follow-up through 18 months, remission was sustained in 6/12 (50%) with Mayo score 0 to 1 versus 2/11 (18%) of patients with Mayo 2 and 3
16 (57%) of the patients were receiving 5-ASA treatment
It would have been helpful to have calprotectin values as well. In their discussion, the authors note that “a normal calprotectin is quite convincing with regard to endoscopic remission” and ECCO ESPGHAN guidelines “provide guidance that a colonoscopy should only be performed if fecal calprotectin” is >250 mcg/g.
My take: Clinical remission in ulcerative colitis should be verified. It is reasonable to start with a fecal calprotectin and if elevated to proceed with endoscopic evaluation (colonoscopy or sigmoidoscopy).
Also: new therapy for Crohn’s disease with favorable phase III study. From Pharmacy Times: Risankizumab (Skyrizi) Demonstrates Significant Improvements In Patients with Crohn Disease Two studies, ADVANCE and MOTIVATE showed similar results for Crohn’s disease. In the ADVANCE study: “40% of patients receiving 600 mg, and 32% of patients receiving 1200 mg achieved endoscopic response at week 12, compared to 12% in the placebo group.” In the MOTIVATE study, “29% and 34% of patients receiving 600 mg and 1200 mg achieved endoscopic response, respectively, compared to 11% in the placebo group.”
Previous studies have indicated that prolonged cholestasis before liver transplantation is associated with adverse neurodevelopmental outcomes. LH Rodijk et al (JPGN 2021; 72: 592-596. Full text: Early Motor Repertoire in Infants With Biliary Atresia: A Nationwide Prospective Cohort Study) prospectively investigate early neurologic impairment in infants with biliary atresia (n=35).
The author’s utilized Prechtl’s General Movement (GM) Assessment which is a noninvasive, cost-effective, and worldwide used method to identify infants who are at risk of neurodevelopmental impairments. This requires video recordings of 10 minutes; this was avoided in the 24 hours following liver biopsy or general anesthesia.
Key finding:
The proportion of infants with atypical GMs was significantly higher in BA (46%) than in 2 reference groups of healthy infants (vs 10%, P < 0.001; vs 18%, P < 0.001).
My take (from authors): “At the time of diagnosis, almost half of the infants with BA showed an atypical early motor repertoire, suggesting that neurological impairment is present already in early infancy. Compared to healthy infants, approximately 2 to 3 times more infants showed an atypical motor repertoire.”
Related blog posts:
Neurodevelopmental Outcomes in Biliary Atresia -same group of authors ( LH Rodijk et al) published data showing a fairly high rate of neurodevelopmental problems in children with BA (25% requiring special education)
Two recent articles delve into the topic of Pediatric to Adult Care Transition.
M Katz et al. J Pediatr (Epub head of publication) 2021. African American Pediatric Liver Transplant Recipients Have an Increased Risk of Death After Transferring to Adult Healthcare (Thanks to a friend who shared this reference & congratulations to my Emory colleagues and senior author Nitika Gupta on this publication)
This retrospective study examined 101 patients between 1990 and 2015. 64 had long-term followup data available.
Key findings:
African Americans had higher rates of death after transfer than patients of other races (44% mor- tality vs 16%, representing 67% of all cases of death; P = .032)
18 of the 64 (28%) died. Of those 18 deaths, 4 (22%) occurred within the first 2 years after transfer, and 10 (55%) within 5 years of transfer.
There was a high rate of medication nonadherence in patients who died. ” Death in our cohort was typically caused by chronic rejection and graft failure, with a high frequency of severe infections or bleeding events ultimately causing a patient to die.”
The average age of transplant in deceased patients was 15. Transplantation in teenage years could be a risk factor as well.
The authors note that “the years directly after transfer of care from pediatrics to adult medicine are high risk for death and poor patient outcomes. Racial disparities seen in pediatric medicine also hold true after transfer to adulthood.”
This retrospective study with 104 subjects defined suboptimal transition as “either a return to pediatric care or requiring care escalation within 1 year of transfer.
Key findings:
37 (36%) were determined to have a suboptimal transition.
Risk factors: mental health diagnosis (OR 4.15), medication non-adherence (OR 5.15), public insurance (OR 6.60), and higher Physician Global Assessment score at time of transition (OR 6.64).
Comments: This is a small study and included only 26 patients receiving public insurance, which the authors considered as a proxy measure of socioeconomic status.
My take: These studies show the difficulties and potential deadly outcomes that face these young adults during transition from pediatrics to adult care. In many cases, medication non-adherence is a key factor and can be affected by access to care, insurance coverage, and mental health. Most young adults with serious medical problems probably would benefit from keeping their parents actively involved in their care.
Outcomes of VEO-IBD. B Kerur et al. Inflamm Bowel Dis 2021; 27: 295-302.Bowel Disease in North America: A Retrospective Cohort Study The study population included 269 children (105 [39%] Crohn’s disease, 106 [39%] ulcerative colitis, and 58 [22%] IBD unclassified). Key findings:
By the end of follow-up, stricturing/penetrating occurred in 7 (6.6%) children.
Median age at diagnosis was 4.2 years. 71 (26%) were ❤ yrs.
Only 5 (1.7%) had a coexisting immunological disorder.
Over 5 years, cumulative use of an immunomodulator and biologic was 61% and 41% respectively. Exclusive enteral nutrition was used in 10 children (4%).
11.5% (n=19) had a change in diagnosis from UC/IBD-U to Crohn’s disease
The risk of any bowel surgery in Crohn’s disease was 3% by 1 year, 12% by 3 years, and 15% by 5 years and did not differ by age at diagnosis.
The risk of colectomy in ulcerative colitis/IBD unclassified was 0% by 1 year, 3% by 3 years, and 14% by 5 years and did not differ by age of diagnosis.
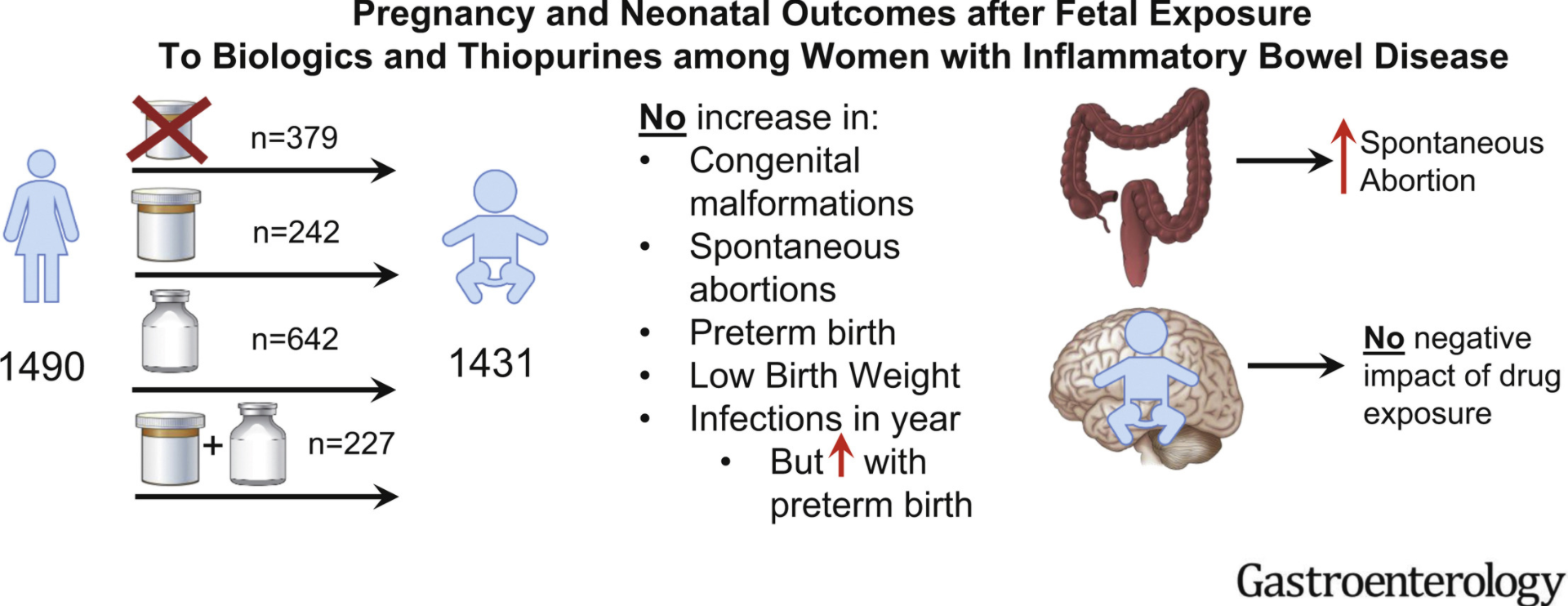
In this PIANO study (2007-2019), pregnant women with IBD were enrolled in a prospective, observational, multicenter study across the United States. PIANO is an acronym for Pregnancy in Inflammatory Bowel Disease and Neonatal Outcomes.
Exposure was to thiopurines (n = 242), biologics (n = 642), or both (n = 227) vs unexposed (n = 379).
In this study, which analyzed Medicaid Analytic eXtract data from 4 states (California, Georgia, North Carolina, and Texas) between 2006 and 2011, the authors identified 14,735 patients with IBD (4672 black [32%]). Key finding: “In patients with Medicaid insurance, where access to IBD-specific therapy should be similar for all individuals, there was no significant disparity by race in the utilization of IBD-specific therapies.”