
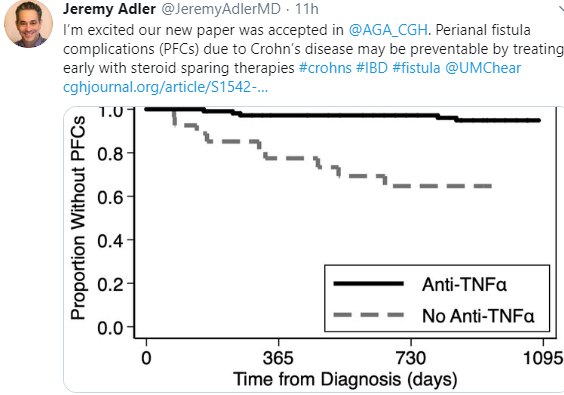
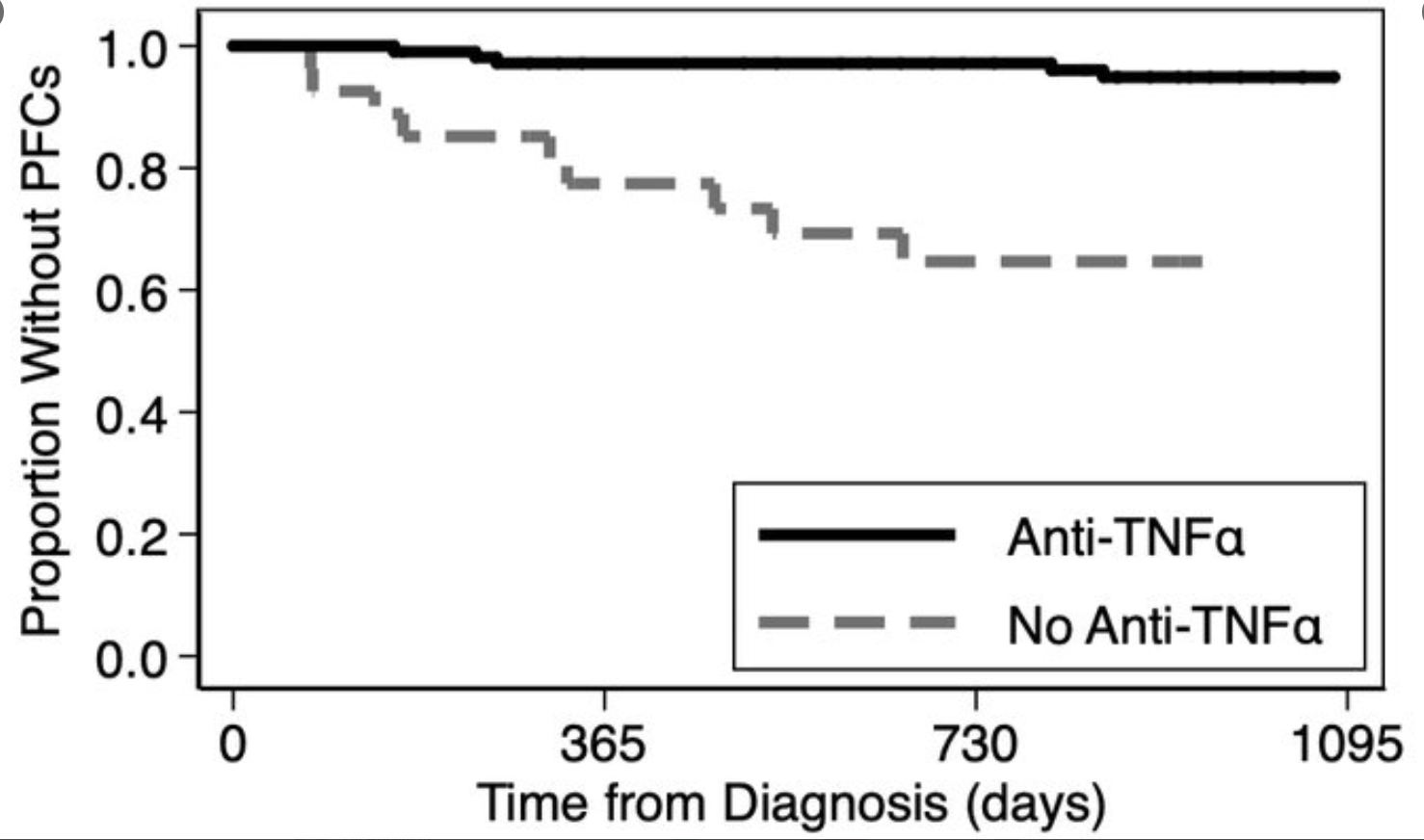
AAM Singer, DA Bloom, J Adler. Clin Gastroenterol Hepatol 2020; In Press: Factors Associated With Development of Perianal Fistulas in Pediatric Patients With Crohn’s Disease
Also, related article:
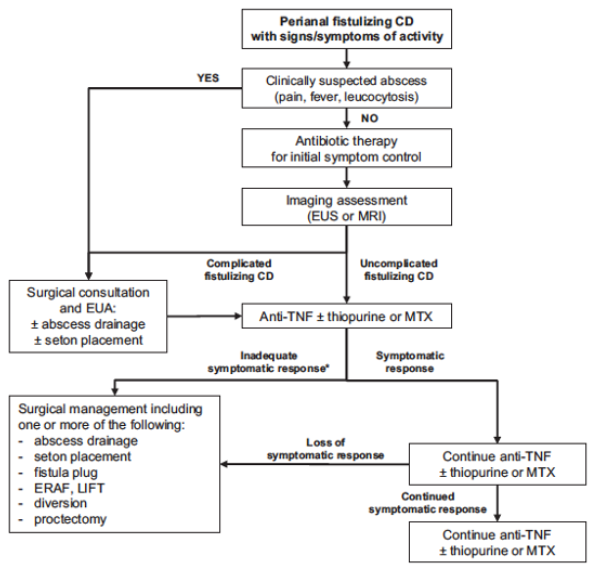
Full Text: Inflamm Bowel Dis. 2019 Jan 1;25(1):1-13. doi: 10.1093/ibd/izy247. Clinical Practice Guideline for the Medical Management of Perianal Fistulizing Crohn’s Disease: The Toronto Consensus.

Related blog posts:
- Efficacy of Anti-TNF Agents for Internal Fistulas
- Video for Patients: Benefits and Risks of IBD Treatment
- Anti-TNF Therapy Associated with Reduced Surgical Resections
- RISK Study -CCFA 2017 Update
- Do Biologics Alter the Natural History of Crohn’s Disease in Children?
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.









{kind=link}
{kind=link}