In this sample of 113 pediatric patients with IBD, 77% of initial denials for biologic therapy were ultimately approved.
The median time to receiving medication was 18 days, with administrative time (prior authorization and appeal) requiring a median of 180 min.
More than half (60%) of patients experienced adverse outcomes or worsened quality of life due to delays in treatment.
My take (borrowed in part from authors): “Barriers to treatment by payors, of which 77% are ultimately approved, result in substantive treatment delay, patient harm, and hospitalization.” While 18 days (or more) may not seem like a lot, it is when you know the right therapy at the outset and delays lead to suffering and worsened outcomes. In addition, the insurance companies and PBMs (pharmacy benefit managers) know that exhausting valuable physician/office staff time is a disincentive. It makes physicians determine whether it is worth the fight.
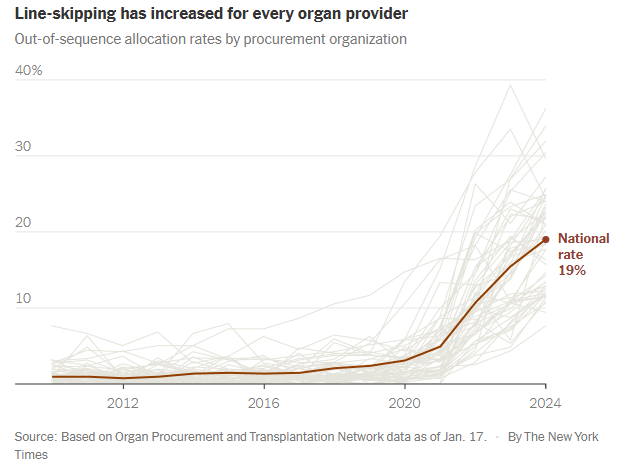
The sickest patients are supposed to get priority for lifesaving transplants. But more and more, they are being skipped over…For decades, fairness has been the guiding principle of the American organ transplant system…today, officials regularly ignore the rankings, leapfrogging over hundreds or even thousands of people when they give out kidneys, livers, lungs and hearts…
Last year, officials skipped patients on the waiting lists for nearly 20 percent of transplants from deceased donors, six times as often as a few years earlier. It is a profound shift in the transplant system, whose promise of equality has become increasingly warped by expediency and favoritism…
Under government pressure to place more organs, the nonprofit organizations that manage donations are routinely prioritizing ease over fairness. They use shortcuts to steer organs to selected hospitals, which jockey to get better access than their competitors.
These hospitals have extraordinary freedom to decide which of their patients receive transplants, regardless of where they rank on the waiting lists. Some have quietly created separate “hot lists” of preferred candidates...
More than 100,000 people are waiting for an organ in the United States, and their fates rest largely on nonprofits called organ procurement organizations…
The procurement organization is supposed to offer the organ to the doctor for the first patient on the list. But the algorithms can’t necessarily identify exact matches, only possible ones. So doctors often say no, citing reasons like the donor’s age or the size of the organ…
Until recently, organizations nearly always followed the list. On the rare occasion when they went out of order and gave the organ to someone else, the decision was examined by the United Network for Organ Sharing — the federal contractor that oversees the transplant system — and a peer review committee. Ignoring the list was allowed only as a last resort to avoid wasting an organ...
Procurement organizations regularly ignore waiting lists even when distributing higher-quality organs. Last year, 37 percent of the kidneys allocated outside the normal process were scored as above-average…
Skipping patients is exacerbating disparities in health care. When lists are ignored, transplants disproportionately go to white and Asian patients and college graduates…
How a rare shortcut became routine
In 2020, procurement organizations felt under attack. Congress was criticizing them for letting too many organs go to waste. Regulators moved to give each organization a grade and, starting in 2026, fire the lowest performers... the organizations increasingly used a shortcut known as an open offer. Open offers are remarkably efficient — officials choose a hospital and allow it to put the organ into any patient...
Open offers are a boon for favored hospitals, increasing transplants and revenues and shortening waiting times. When hospitals get open offers, they often give organs to patients who are healthier than others needing transplants…Healthier patients are likelier to help transplant centers perform well on one of their most important benchmarks: the percentage of patients who survive a year after surgery...
It is impossible to gauge whether line-skipping prevents wasted organs. But data suggests it does not. As use of the practice has soared, the rate of organs being discarded is also increasing.
My take: This article was eye-opening for me as I am not actively involved in listing patients for transplantation. I was unaware of this increasing tendency of line-skipping and open source allocation. It is disturbing to see the distribution process undermined in this manner –better oversight is needed to assure fairness for those whose lives are at stake.
M Cananzi et al. J Pediatr Gastroenterol Nutr. 2025;80:260–270. Current practice in the management of paediatric autoimmune liver disease in Europe
Methods: Thirty-six centers from 22 European countries responded to the survey that was sent to European Reference Network for Rare Liver Disorders (ERN RARE-LIVER) and members of the Hepatology Interest Group (HIG) of the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN)
Key findings:
All centers use predniso(lo)ne as first-line therapy, alone (15/36) or with azathioprine (21/36)
Azathioprine and mycophenolate are the preferred second-line options in centres using first-line steroid monotherapy (11/15) or combined steroid-azathioprine (19/21)
Tacrolimus is used as third-line agent in 15/36 centers
Proactive measurement of drug metabolites and target levels vary widely among centers. About 27/36 centers have thiopurine methyltransferase (TPMT) genotyping available, of which 21 (58%) routinely perform this test before prescribing AZA. Among the 12 centres that reported target metabolite levels, 10 aim for levels between 200 and 300 pmol/8 × 108 red blood cells (RBC).
About 24/36 centers routinely incorporate PPIs into steroid treatment protocols, seven prescribe PPIs solely when there are risk factors for peptic ulcer disease, and the remainder refrain from using PPIs unless gastrointestinal symptoms occur.
My take: There is a great deal of variation in the management of autoimmune hepatitis indicating the need for more collaborative efforts to advance evidence-based therapeutic strategies.
MT Fioretti et al. J Pediatr Gastroenterol Nutr. 2025;80:300–307. A decade of real-world clinical experience with 8-week azithromycin–metronidazole combined therapy in pediatric Crohn’s disease
Methods: This retrospective study over 10 years examined the efficacy of azithromycin-metronidazole for induction treatment in 44 children. All patients were given metronidazole (15–20 mg/kg/day two times daily, maximum of 1000 mg/day) administered daily for 8 weeks and azithromycin (7.5 mg/kg to a maximum of 500 mg/once a day) administered 5 days per week for the first 4 weeks, followed by 3 days per week for the final 4 weeks as per the initial publications.17, 18
Key findings:
After 8 weeks, the overall remission rate was 64%.
Of the 38 patients who completed the CD AZCRO course, 28 patients (74%) entered remission (Group 1) and 10 (26%) did not (Group 2)
After 8 weeks, Group 1 showed improved CRP levels and higher albumin and hemoglobin levels than Group 2. Median FC declined significantly from 650 mcg/g at baseline to 190 mcg/g at Week 8 in Group 1 (p < 0.001).
The authors conclude that “a combination treatment of azithromycin and metronidazole represents an alternative induction therapy for mild to moderate pediatric CD, offering benefits in terms of cost and practicalities compared to EEN and in side effects compared to steroids.”
My take: There are a small number of children with mild Crohn’s disease who could benefit from this induction regimen. An alternative would be the use of a more modest dietary approach (eg. Mediterranean diet)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: Hypermobility spectrum disorders (HSD) and hypermobility Ehlers–Danlos syndrome (hEDS) are frequently associated with gastrointestinal symptoms, although the underlying mechanisms remain unclear. Since recruitment occurred before the 2017 criteria for hEDS were established, it was not possible to distinguish between HSD and hEDS.
Methods: Retrospective review of all patients (>18 yrs) referred t for gastrointestinal motility evaluation and undergoing ADM were consecutively included from 2009 to 2023. This included 239 patients (50 HSD/hEDS and 189 non-HSD/hEDS). The HSD/hEDS group showed a lower BMI and higher use of enteral feeding than the control group (p < 0.001 and p = 0.026, respectively). This group was also younger, with a mean age of 30.4 ± 11.1 years versus 45.3 ± 15.4 years (p < 0.001).
Key findings:
The prevalence of antroduodenal dysmotility was not different between both groups, but enteric dysmotility was less common in the HSD/hEDS group (13% vs. 34%, p = 0.006).
There were similar percentages of delayed gastric emptying than non-HSD/hEDS patients; delayed gastric emptying was highly prevalent in both groups, 85% in patients with HSD/hEDS and 94% in non-HSD/hEDS patients
There were no differences in predominant symptoms between patients with and without HSD/hEDS.
In the discussion, the authors note that the lower rate of dysmotility combined with higher rates of enteral nutrition indicate that “factors like visceral hypersensitivity and autonomic function could be relevant in this context.”
My take: Most patients at this referral center had delayed gastric emptying. However, Ehlers-Danlos patients, in fact, had lower rates of enteric dysmotility.
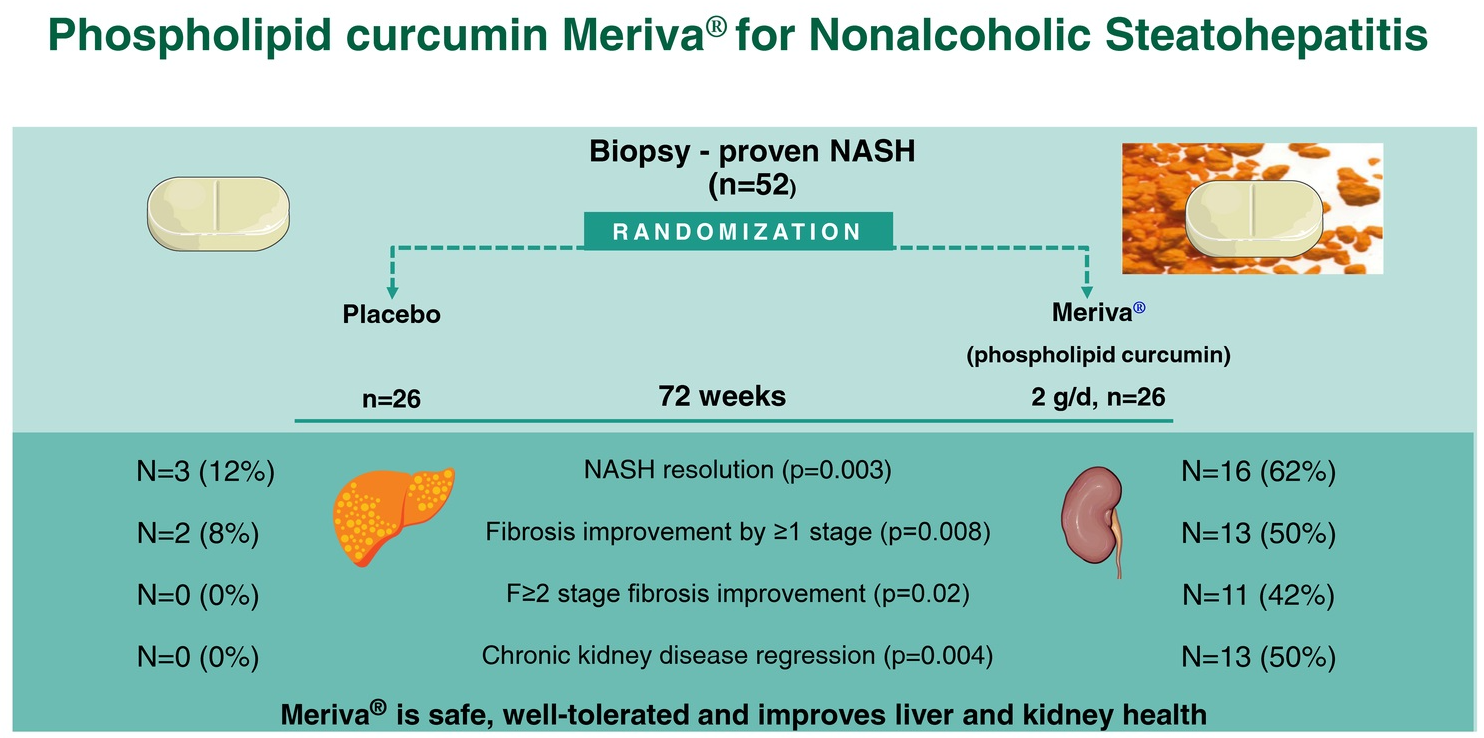
“Let food be thy medicine” is a well-known phrase usually attributed to Hippocrates (though it is unclear if he said this). Regardless, this study indicates that added curcumin in the diet could be beneficial for steatotic liver disease.
Methods: In this double-blind trial, 52 patients with biopsy-proven NASH (71% with stage ≥F2 fibrosis, 58% with stage A2-G2/A2-G3a chronic kidney disease) were randomized 1:1 to receive Meriva 2 g/d (1 g BID) or placebo for 72 weeks. Meriva is a formulation of curcumin extract with phospholipids that has improved oral bioavailability of curcumin metabolites.
Key findings:
Sixteen (62%) patients on Meriva (curcumin) versus 3 (12%) patients on placebo had NASH resolution (RR = 5.33)
hirteen (50%) patients on Meriva versus 2 (8%) patients on placebo had ≥1 stage fibrosis improvement (RR = 6.50)
Eleven (42%) patients on Meriva versus 0 (0%) on placebo had regression of significant liver fibrosis (RR = 18.01)
Thirteen (50%) patients on Meriva versus 0 (0%) on placebo had chronic kidney disease regression (RR = 10.71)
Compared with placebo, Meriva improved eGFR (difference in adjusted eGFR change: +3.59 [2.96–4.11] mL/min/1.73 m2/y, p = 0.009), fasting glucose(−17 mg/dL; 95% CI = −22, −12), HbA1c (−0.62%; 95% CI = −0.87%, −0.37%), LDL-C (−39 mg/dL; 95% CI = −45, −33), triglycerides (−36 mg/dL, 95% CI = −46, −26), HDL-C (+10 mg/dL; 95% CI = +8, +11), and inflammatory markers
The observed benefits were associated with downregulation of hepatic NF-kB which is a proinflammatory transcription factor and a known curcumin target
My take: A larger multicenter study is needed to confirm these promising results. This study shows that dietary changes and lifestyle modification remain important tools in treating MASH (aka NASH).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“Health insurers process more than five billion payment claims annually, federal figures show. About 850 million are denied, according to calculations by appeals company Claimable, based on data from health-policy nonprofit KFF and the Centers for Medicare and Medicaid Services. Less than 1% of patients appeal.
Few people realize how worthwhile those labors can be: Up to three-quarters of claim appeals are granted, studies show…”
The author then details how one man overcame a denial to receive a life-saving liver transplantation and how a family helped their child receive immunoglobulin therapy for her neurologic condition. However, this only occurred after numerous appeals and after letters to the Georgia governor and Georgia attorney general.
Excerpts from the second article:
“Here are five things you can do to appeal a denied health-insurance claim.
1. Read up
Know what your plan covers. A good place to start is the summary of benefits and coverage. More detailed information should be available from your employer or insurer, which can provide a more in-depth document sometimes called the “evidence of coverage.” Check to make sure a denial met your insurer’s own rules. These policies are generally available online.
2. Take note
Log dates of calls to your insurer and whom you spoke to. Save paperwork including billing codes for denied services. And act quickly: Insurers have deadlines to file appeals.
3. Fight back
Call your insurer at the number on the back of your insurance card and ask why treatment wasn’t covered. You can ask how to file an appeal. If you have a denial or explanation of benefits letter, look for the section explaining appeals.
4. Get help
State assistance programs and nonprofits including the Patient Advocate Foundation and the Medicare Rights Center can help craft appeals. A startup called Claimable is trying to use technology to smooth the process. You can hire an advocate, looking through a directory or a third-party company, Solace Health. The nonprofit Dollar For helps with hospital bills. You can also ask your doctor’s office or hospital to appeal for you, and try to ensure they keep you in the loop on their communications.
5. Escalate
After you determine why your insurer denied a claim, you can write a letter explaining why the rejection wasn’t warranted. Your doctor can write a letter explaining why care is medically necessary. Pertinent medical studies can strengthen your case. Request the “designated record set” relevant to your case.
If your appeal is rejected, you can often appeal to a higher authority within the insurer. If that fails, you can generally appeal to a third party, often an independent review organization or a government-administered program. Your rejection letter or state insurance department should explain those steps. Practices vary state by state. You can also escalate your appeal to an administrative law judge.”
FDA IBD Workshop -Take-Home PointsOff-label does not equate to experimentalFDA Statement: The FD&C Act does not, however, limit the manner in which a physician may use an approved drug. Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling. Such “unapproved” or, more precisely, “unlabeled” uses may be appropriate and rational in certain circumstances, and may, in fact, reflect approaches to drug therapy that have been extensively reported in medical literature
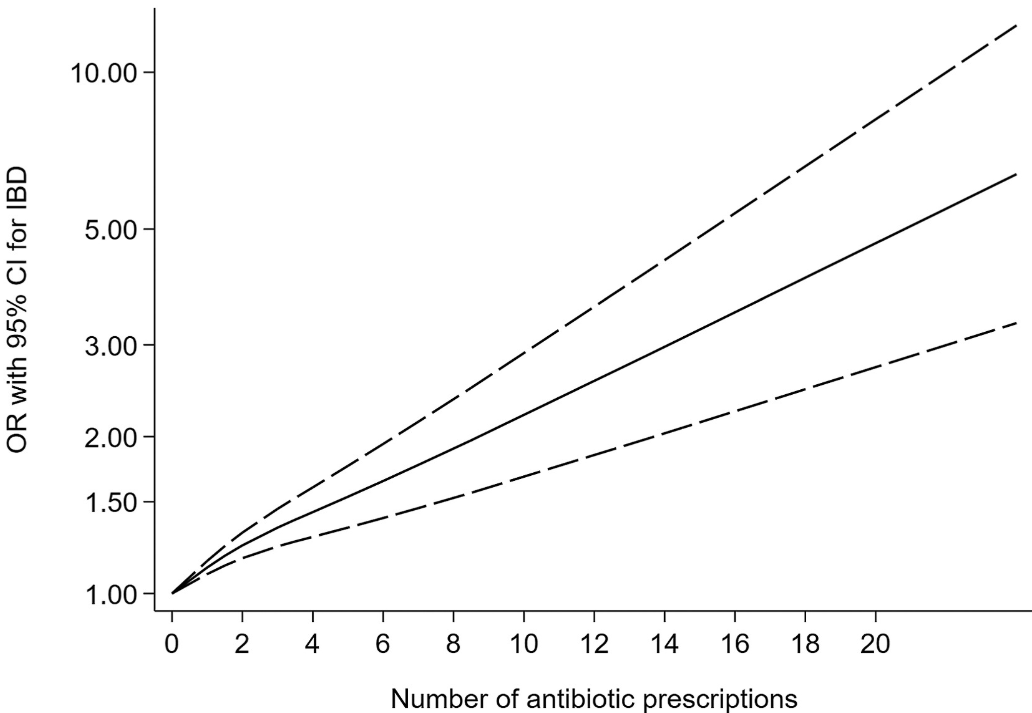
Twenty-eight studies involving 153,027 patients with IBD were included.
Key findings:
Antibiotic exposure was significantly associated with an increased risk of new-onset IBD for prescription-based studies (pooled OR, 1.41; 95% CI, 1.29–1.53) and for questionnaire-based studies (pooled OR, 1.35; 95% CI, 1.08–1.68). ‘
This association existed for both Crohn’s disease and ulcerative colitis, as well as in children and adults for prescription-based studies.
Some of the limitations:
There was statistical heterogeneity was high in the primary analysis, possibly because of inconsistencies in study design
Most studies included a clear lag time, yet an inadequate lag time still creates the possibility of reverse causality.
The authors could not disentangle the risk of antibiotics from the risk of infection in leading to the development of IBD.
Nonlinear dose-response relationship between antibiotic exposure and risk of new-onset IBD (solid black line and short dash black line represent estimated ORs and corresponding 95% CIs of nonlinear relationship)
My take: This is another study showing an association between antibiotic use and new-onset IBD. While this study does not prove causation, it is another reason for good antibiotic stewardship.
K Underhill, KM Nelson. NEJM 2025; 392: 523-525. Legal Threats to Clinicians and Patients
An excerpt:
In January 2023, Utah added a section to its Health Care Malpractice Act (see box). The change was part of Senate Bill 16, a larger package of laws targeting gender-affirming care. The new Malpractice Act language specifies that for “hormonal transgender treatment” and surgery on “sex characteristics,” patients treated when they are minors have the option to disaffirm — revoke — their consent before 25 years of age...
Although patients consent at the time of treatment, Utah’s new law enables them to withdraw their informed consent retroactively, even years later, and pursue legal claims based on being treated without consent...
Utah’s new law places a tremendous burden on clinicians…
It is unrealistic and unreasonable to expect clinicians to predict which patients may later reverse their consent to treatment. Clinicians who undertake these predictions will make mistakes in both directions — either failing to predict regrets (which are rare2) or, more likely, erroneously denying medically necessary care to minors who would benefit from it…
Allowing minors to recant their consent undermines the efforts that many states have made to strengthen minors’ independent access to care for sexual health, mental health, and substance use. Laws that have a chilling effect on medical services can also interfere with the pipeline of clinicians who have the training and experience to deliver care, reducing access for all patients…
Utah’s law is more worrisome, however, as a potential harbinger of things to come…As legislators develop and test state laws interfering with gender-affirming care, the same strategies become available for other politically contested forms of health care.
My take: Allowing individuals to recant consent for treatment years later will undermine access to all types of health care.
Related article: DG Aaron, C Konnoth. NEJM 2025; 392: 526-528. This article explains the flawed “Cass Review” which was a a 388-page report commissioned by England’s National Health Service (NHS) concluded that “there is not a reliable evidence base upon which to make clinical decisions” regarding gender-affirming care (GAC).
“Our concern here is that the Review transgresses medical law, policy, and practice, which puts it at odds with all mainstream U.S. expert guidelines. The report deviates from pharmaceutical regulatory standards in the United Kingdom. And if it had been published in the United States, where it has been invoked frequently, it would have violated federal law because the authors failed to adhere to legal requirements protecting the integrity of the scientific process..3 The Review calls for evidentiary standards for GAC that are not applied elsewhere in pediatric medicine.“
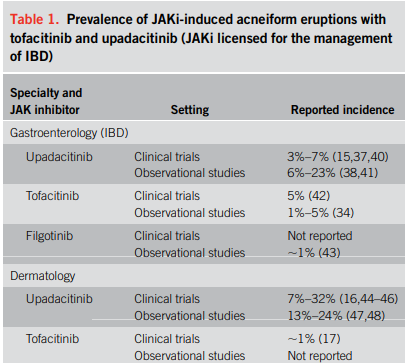
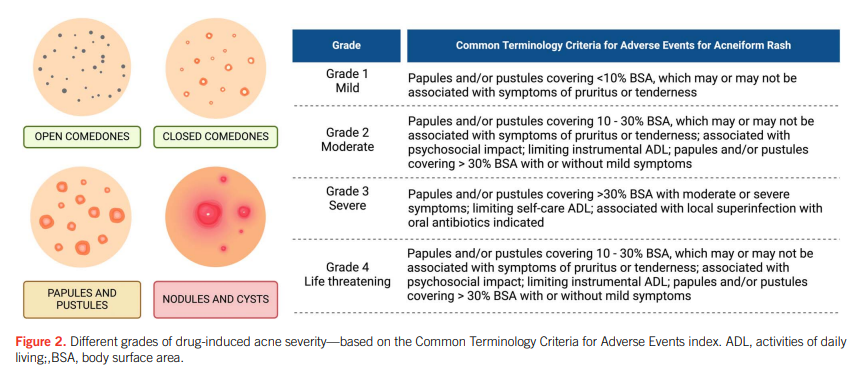
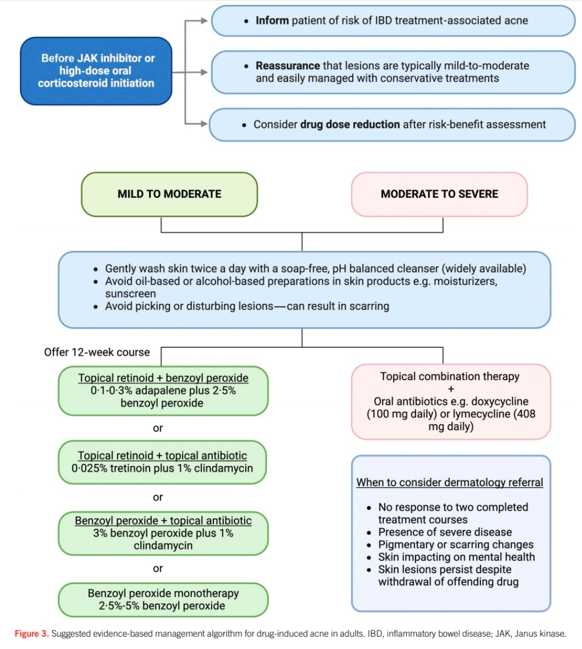
“Corticosteroids and Janus kinase inhibitors (JAKi) are commonly used for the treatment of inflammatory bowel disease (IBD) and are known to aggravate a prior tendency to acne or trigger the development of new acneiform eruptions. Both randomized controlled trials and real-world studies have identified acne as one of the most common treatment-emergent adverse events in JAKi… This review examines the characteristics of drug-induced acne in IBD treatments, provides a practical guide for gastroenterologists to manage mild-to-moderate occurrences, and highlights when to seek specialist dermatology advice.”
My take: This is a helpful review of acne management in the setting of IBD.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.