TJ Woodruff. NEJM 2024; 390: 922-933. Health Effects of Fossil Fuel–Derived Endocrine Disruptors
Initially, I was tempted to title this post ‘Burying the Evidence and the Bodies from Pollution.’ That sounded too alarmist, though. That said, this review article asserts that “chemical pollution is estimated to be responsible for at least 1.8 million deaths each year…This number is probably an underestimate, since less than 5% of approximately 350,000 chemicals registered for use globally have been adequately studied.1” (90% of pollution-related deaths occurring in low- and middle-income countries).
In addition, “polluting industries [are] “weaponizing” scientific uncertainty to foster distrust in scientific findings and lobbying for weaker regulations.71 For example, previously secret industry documents show that the industries knew about the health harms of PFAS decades before the scientific and public health community did.72” The science behind pollution is hampered by the inability (unethical) to conduct randomized trials of pollution exposure.
This article focuses on Endocrine Disruptors Chemicals (EDCs).
Health Effects of Fossil Fuel–Derived Endocrine Disruptors
- Fossil fuels contribute to chemical pollution through production of petrochemicals, many of which interfere with hormonal function (endocrine-disrupting chemicals [EDCs]). Examples include perfluoroalkyl and polyfluoroalkyl substances in food packaging and fabrics and phthalates in plastics and consumer products.
- Petrochemical production is increasing, and people are exposed through contaminated air, water, food, and manufactured products (e.g., plastics, pesticides, building materials, and cosmetics).
- EDCs can increase several health risks, including cancer, neurodevelopmental harm, and infertility.
- Risks are higher with exposures during fetal and child development and with exposure to multiple EDCs and occur at low exposure levels. Exposures are higher in communities of color and low-income communities and contribute to health inequities.
- Clinicians can provide advice to patients toward reducing some exposures, but policy change is needed to establish legal requirements for comprehensive safety testing and to reduce health threats from petrochemicals. Clinicians are important advocates for these changes.
Figure 2 reviews the potential individual modifiers to the effects of pollution as well as the increased adverse health effects.

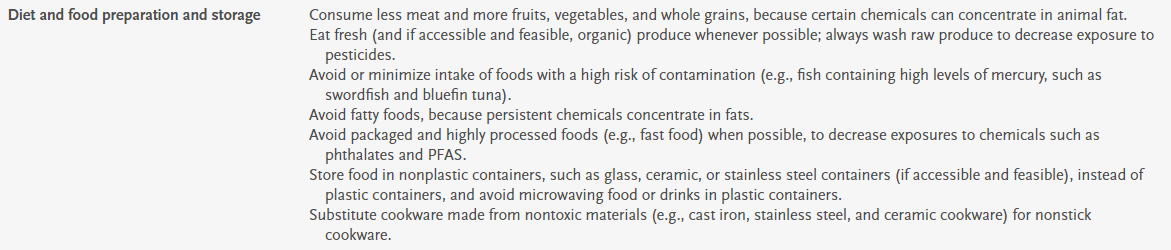
Table 2 provides recommendations for reducing exposures including diet/food preparation, cleaning/use of cleaning products, minimizing occupational exposures, and advocacy.
My take: There are limited steps that individuals can take to reduce their exposures. In order to make our environment safer, this requires policy changes. Most individuals do not even know if they are being exposed to dangerous pollutants and would have limited ability to move away from unsafe areas.
Related blog posts: