R Mahmoud et al. Clin Gastroenterol Hepatol 2023; 21: 750-760. Open Access! Complete Endoscopic Healing Is Associated With Lower Relapse Risk After Anti-TNF Withdrawal in Inflammatory Bowel Disease
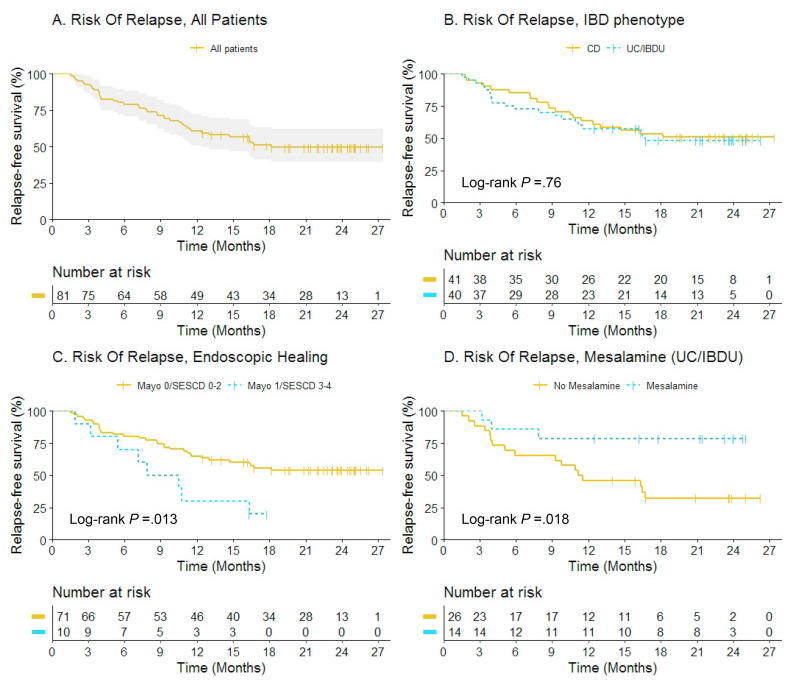
This was a prospective observational study (n=81). In order to participate, patients (all adults) had to be in confirmed baseline steroid-free clinical remission (for at least 6 months) and endoscopic healing; endoscopic healing was defined as endoscopic Mayo score <2 or Simple Endoscopic Score for CD (SES-CD) <5 without large ulcers. Endoscopic healing was subclassified as complete endoscopic healing (Mayo 0/SES-CD 0–2) versus partial endoscopic healing (Mayo 1/SES-CD 3–4).
Key findings:
- At 12 months, 70% (7 of 10) versus 35% (25 of 71) of patients with partial versus complete endoscopic healing relapsed, respectively (adjusted hazard rate [aHR], 3.28; 95% confidence interval [CI], 1.43–7.50)
- Mesalamine use was associated with fewer relapses in UC/IBDU patients (aHR, 0.08; 95% CI, 0.01–0.67)
- Thirty patients restarted anti-TNF, and clinical remission was regained in 73% at 3 months.
The authors highlight the lower relapse rate between those with complete endoscopic healing and those with partial healing. They acknowledge that those eligible for anti-TNF de-escalation are highly selected (~7% in a prior study) and “few patients with an unfavorable IBD phenotype, such as stricturing or penetrating CD, anti-TNF for perianal fistulizing CD, young age at diagnosis, or prior biological failure, were included in this study. Therefore, our findings may not be generalizable to patients with a more severe IBD phenotype.
My take: Even in those with complete endoscopic healing, there is a high rate of relapse. In addition, stopping anti-TNF therapy likely increases risk of not responding to anti-TNF therapy when it is restarted. This study does show that transitioning from anti-TNF therapy to mesalamine therapy in those with ulcerative colitis (or IBDU) could be a reasonable consideration.
Related blog posts: