The authors identifed 25 studies which met inclusion criteria. Key findings:
In the analysis of studies with 3-category outcomes (n = 13), the pooled frequencies of patients (n=646) with improved, unchanged, or aggravated IBD course after LT were 29.4%, 51.4% (, and 25.2%.
Subgroup analyses revealed that patients with ulcerative colitis (UC), younger age at LT, or shorter duration of follow-up were more likely to have an improved disease course.
In the analysis of studies with 2-category outcomes (n = 12), the pooled frequencies of patients (n=672) with improved/unchanged or aggravated IBD course were 73.6% and 24.1%, respectively
My take: Despite the intensification of immunosuppression, most often the course of IBD is unchanged in patients following a liver transplantation.
In this cross-sectional multicenter study evaluating transition readiness in individuals (n=186, prospectively recruited ) with IBD 16-19 years old, the authors used the validated ON Taking Responsibility for Adolescent to Adult Care (ON TRAC) questionnaire.
Key findings:
ON TRAC scores determined that 26.6% of AYAs at pediatric and 40.4% at adult centers reached the threshold of readiness. The findings are limited by potential nonresponse & sampling bias.
Disease remission negatively (P = .03) associated with ON TRAC scores.
A significant percentage of AYAs reported moderate-to-severe depression (21.7%) and generalized anxiety (36%); however, neither were significantly associated with ON TRAC scores
The authors suggest that a joint clinic with adult/pediatric providers may be helpful to improve transition.
MB Cohen. J Pediatr 2023; 258. DOI:https://doi.org/10.1016/j.jpeds.2023.113556Are You Ready to Transition? In commentary on this article, Dr. Cohen writes the following: “a novel finding was that transition readiness was inversely related to disease remission; this confirms what had been previously suggested.1 Patients who are doing well may not be as engaged in developing skills for transition readiness and knowledge about their chronic illness, unlike those with more significant disease or symptoms.”
My take: Many studies show that adolescents and young adults with IBD are not fully prepared to transition to adult medical practices. In my view, it would be better to encourage the young adult to continue engaging with his/her parents until readiness is achieved rather than try to change to a multispecialty clinic.
Related blog posts:
Challenging Assumptions: Self-Management Skills in Adolescents and Poor Outcomes (provides detailed list of tasks needed for self-management). In this transition study of liver transplant patients, negative outcomes were more common in adolescents who reported greater self-management (RA Annunziato et al. J Pediatr 2018; 193: 128-33).
Key findings: After switching from IV infliximab to SC 120 mg every other week, 6 of 7 patients remained in clinical remission with no significant changes in laboratory markers and median infliximab trough levels (12.3 µg/mL at baseline; 13.9 and 14.0 µg/mL at 6 and 40 weeks respectively).
In this multinational trial, called LIBERTY-CD, the median trough level was 16 mcg/mL, which is higher than that typically associated with IV dosing, according to Dr. Hanauer, who presented the results at Digestive Disease Week 2023 (abstract 1028)… “most professional societies to recommend a trough of 10 mcg/mL,” Dr. Hanauer said….
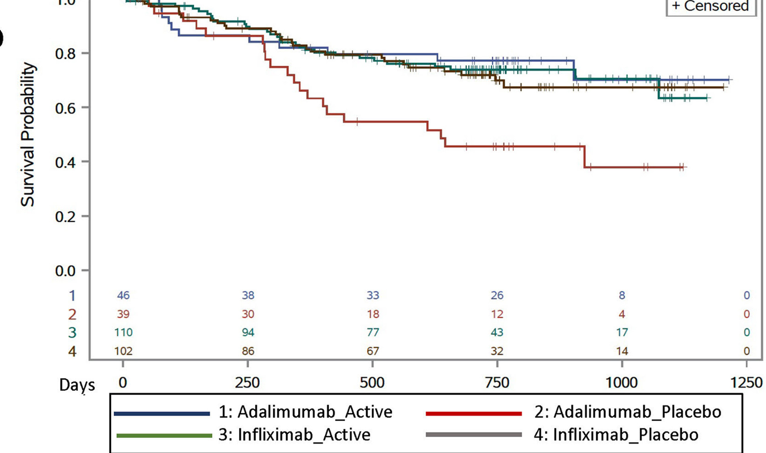
All patients received induction doses of infliximab by IV at weeks 0, 2 and 6. Those who achieved at least a 100-point reduction in the Crohn’s Disease Activity Index (CDAI), which accounted for 86% of the 396 patients initially enrolled, were randomized in a 2:1 ratio to receive 120 mg of subcutaneous infliximab (CT-P13) or placebo every two weeks.
The proportion of patients meeting the end point of clinical remission, defined on the basis of CDAI, was 62.3% for active therapy and 32.1% for placebo (P<0.0001). The proportion of patients in the active treatment arm achieving an endoscopic response was nearly three times higher than the proportion in the placebo arm (51.1% vs. 17.9%; P<0.0001).
My take: This study shows that SC infliximab (after IV induction) should be effective. A study showing that the SC product is not inferior to the IV dosing would be helpful. It is likely that vedolizumab will receive approval in U.S. for a similar IV induction followed by maintenance subcutaneous therapy in the next year.
This post hoc analysis included data from separate trials examined the response of 220 biologic-naïve CD participants to either inflximab biosimilar or ustekinumab.
Key findings:
Clinical remission: One-year clinical remission (CR) and corticosteroid-free CR rates were similar between infliximab-treated and ustekinumab-treated patients (CR, 66 of 110 [60.0%] vs 63 of 110 [57.3%]; adjusted odds ratio [aOR], 1.15), corticosteroid-free CR, 11 of 28 (39.3%) vs 27 of 51 [52.9%]; aOR, 0.58)
Endoscopic response/remission: infliximab-treated participants were more likely to achieve 1-year endoscopic response (43 of 92 [46.7%] vs 6 of 30 [20.0%], aOR, 3.59) and endoscopic remission (31 of 92 [33.7%] vs 4 of 30 [13.3%]; aOR, 3.35)
In the discussion, the authors note only 1 head-to-head study in CD with ustekinumab. “The SEAVUE trial (NCT03464136) compared adalimumab and ustekinumab among biologic-naïve CD patients. Ustekinumab demonstrated similar efficacy for the achievement of clinical and endoscopic outcomes compared with adalimumab.23 Similar rates of CR at 1 year were reported in SEAVUE (64.9% ustekinumab vs 61% adalimumab) as in our analysis (57.3% ustekinumab vs 60% infliximab)…ustekinumabdemonstrated longer retention and lower immunogenicity and has practical advantages over adalimumab, including less frequent dosing intervals (every 8 weeks for ustekinumab vs every 2 weeks for adalimumab) while providing similar efficacy.”
My take: This study suggests that infliximab may be a little better than ustekimumab in biologic-naive patients due to the higher endoscopic response; however, the study was unpowered to provide a definitive answer. A prior study suggested similar endoscopic healing rates (P Riviere et al. Inflamm Bowel Dis 2023; 29: 923-931).
Methods: “We performed a prospective analysis of clinical outcomes on upadacitinib in patients with UC and CD using predetermined intervals at weeks 0, 2, 4, and 8 as part of a formalized treatment protocol.” 84 met inclusion criteria (44 UC patients, 40 CD patients) -though complete data was available for only a fraction of these. All of the patients had received prior anti-TNF therapy and 89% had received 2 or more advanced therapies.
Key findings:
Ulcerative colitis: At 4 and 8 weeks of treatment, 19 of 25 (76.0%) and 23 of 27 (85.2%) achieved clinical response and 18 of 26 (69.2%) and 22 of 27 (81.5%) achieved clinical remission, respectively. Of those who previously were tofacitinib-exposed, 7 of 9 (77.8%) achieved clinical remission by 8 weeks.
Crohn’s disease: In CD, 13 of 17 (76.5.%) achieved clinical response and 12 of 17 (70.6%) achieved clinical remission by 8 weeks. Of those with increased fecal calprotectin and C-reactive protein levels, 62% and 64% normalized by week 8, respectively.
Results were seen as early as week 2 in both UC and CD, with clinical remission rates of 36% and 56.3.%,
Acne was the most commonly reported adverse event, occurring in 24 of 105 patients (22.9%) (Table 4). Six patients stopped upadacitinib due to adverse effects.
My take: “In this large real-world experience in medically resistant patients with UC or CD, we report that upadacitinib is rapidly effective and safe, including in those who had prior tofacitinib exposure.” In pediatrics, the effectiveness of this upadacitinib is a logical target for ImproveCareNow. More pediatric data will be needed to garner FDA approval.
A Bousvaros, BAR Schmidt, M Kurtz. Gastroenterology & Hepatology 2023; 19: 401-403. Open Access! “Treatment of Genital Crohn’s Disease with Upadacitinib in a Male Child: A Case Report”. This report describes the rapid response to upadacitinib in a 12 yo with refractory Crohn’s ileocolitis (x 5 yrs) with associated “granulomatous lymphangitis” affecting the penis and scrotum. It notes that “anti-TNF therapy was described as the most effective treatment, with either improvement or resolution of scrotal swelling in most patients. However, intermittent penile swelling persisted in a subset of the patients.18“…”Although data on the use of JAK inhibitors to treat pediatric IBD are limited, the fact that these are small molecules with wide systemic effects suggests that JAK inhibitors may be useful in the treatment of extraintestinal manifestations of IBD….[and] that JAK inhibitors such as upadacitinib may play an important role in the treatment of such refractory patients.”
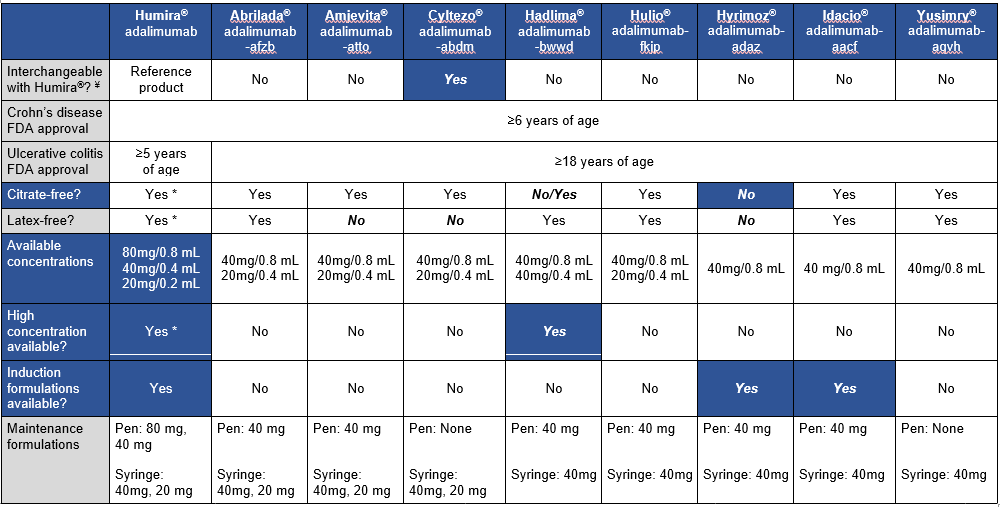
This article is a very handy update on approved adalimumab biosimilars, though even more biosimilars are expected to become available soon. The table below which is similar to a table in the article outlines the similarities and differences in these products compared to the reference product.
These biosimilars are FDA-approved for the treatment of adult and pediatric patients aged 6 and older with Crohn disease. “However, the biosimilar products are only approved for treatment of adult patients” (18 and older) with ulcerative colitis. “This may be due to the recent change in pediatric ulcerative colitis Humira FDA-approved dosing.”
My take (borrowed in part from authors): Insurance coverage decisions are likely to overlook some of these factors which are very important for pediatric patients. “The adalimumab biosimilars will likely provide a clinically effective, cost saving option for our patients, but consideration of a number of factors will be key when selecting between” them.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A previous study (SEAVUE) has suggested similar efficacy of ustekinumab and adalimumab in biologic-naive patients (post: SEAVUE: Head-to-Head Ustekimumab vs. Adalimumab) with ~60-65% clinical response at 52 weeks and ~30% endoscopic remission.
This current retrospective study sought to obtain ‘real-world’ data comparing anti-TNF agents (95 adalimumab, 61 infliximab) to ustekinumab (n=50). In the anti-TNF group, 44% (n=68) received concomitant immunomodulator therapy. Key findings:
At 3 months, clinical response rates were 86% in anti-TNF groups and 64% in the ustekinumab.
At 12 months, in adjusted multivariate analysis, clinical remission (based on Harvey-Bradshaw Index) was independently associated with the biological therapy received (odds ratio, 2.6 for anti-TNF agent vs ustekinumab;P = .02).
“In our sensitivity analysis, a significant difference in terms of efficacy was only found between infliximab and ustekinumab.”
In those with ileocolonoscopy, endoscopic healing was similar (between 6-18 months): 58% of anti-TNF group and 61% of ustekinumab group.
2% of patients in the anti-TNF group had severe adverse events compared to none in the ustekinumab group; among patients receiving adalimumab, 1 patient had cerebral aspergillosis, 1 had a postinfectious macrophage activation syndrome, and 1 had severe folliculitis needing abscess drainage.
Drug persistence at 12 months was 87% in anti-TNF group and 88% in ustekinumab group.
The discussion notes that ‘real-world’ data is important as only ~30% of patients in a regular practice would fulfill the criteria to be included in clinical trials. However, in this retrospective (non-randomized) study, there were differences in the patient population that could affect response to treatment, including a higher rate of smokers in the anti-TNF group (29% compared to 12% in the ustekinumab group).
My take: While anti-TNF therapy, particularly infliximab, may be a little better based on clinical remission, the most objective marker of efficacy, endoscopic healing, was similar. Thus, it is not clear if anti-TNF therapy is more effective than ustekinumab. To achieve optimal results, many in the anti-TNF group received immunomodulator cotherapy and dose escalation.
Joel Andres, Chef & Philanthropist, World Central Kitchen
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This retrospective cohort study identified 1037 patients with Crohn’s disease who underwent ileocecal resection (ICR). Only 5.4% were younger than 18 yrs at the time of surgery. In this cohort, 278 (26%) received a biologic agent as prophylaxis to prevent recurrence with 80% receiving an anti-TNF agent. In those receiving an anti-TNF agent, 35% were started on therapy within 4 weeks of surgery and 65% were started between 4 and 12 weeks. Recurrence was defined by endoscopy (≥ i2b Rutgeerts score) or radiography (active inflammation in neoterminal ileum). Key findings:
After adjusting for factors associated with postoperative recurrence (POR), compared with no biologic prophylaxis, the initiation of an anti-TNF agent (n=223) within 4 weeks following an ICR was associated with a reduction in POR (adjusted hazard ratio, 0.61).
Prophylaxis after 4 weeks following an ICR or with vedolizumab or ustekinumab was not associated with a reduction in POR compared with those who did not receive prophylaxis –though sample size with vedolizumab (n=27) and ustekinumab (n=28) was very limited
Most patients receiving biologic prophylaxis had prior anti-TNF exposure including 73% of the anti-TNF group, 96% of the vedolizumab group, and 93% of the ustekinumab group.
In their discussion, the authors note that their findings reinforce previous studies which showed beneficial effects of anti-TNF therapy for POR, including the PREVENT trial. This randomized controlled trial with infliximab initiation within 45 days postoperatively in high risk individuals reduced endoscopic recurrence at 18 months (22.4% compared with 51% in placebo group).
My take: Anti-TNF therapy, even in those with prior exposure, likely improves outcomes in patients with Crohn’s disease following ileocecal resection. This study indicates that starting therapy within the first 4 weeks is more beneficial.
This study enrolled 297 children with Crohn’s disease starting anti-TNF therapy. Patients initiating infliximab or adalimumab were randomized in 1:1 allocation to methotrexate or placebo and followed for 12–36 months.
Methotrexate dosing: For those in the active arm, oral methotrexate was administered with a weekly dose of 15 mg for children ≥40 kg, 12.5 mg for children 30 to <40 kg, and 10 mg for children 20 to <30 kg. All participants received pretreatment with ondansetron 4 mg (or placebo) to prevent nausea and folic acid (1 mg/d).
Key findings:
For treatment failure: among infliximab initiators, there were no differences between combination and monotherapy (hazard ratio, 0.93; 95% CI, 0.55–1.56)
For treatment failure: among adalimumab initiators, combination therapy was associated with longer time to treatment failure (hazard ratio, 0.40; 95% CI, 0.19–0.81).
A trend toward lower anti-drug antibody development in the combination therapy arm was not significant (infliximab: odds ratio, 0.72; 95% CI, 0.49–1.07; adalimumab: odds ratio, 0.71; 95% CI, 0.24–2.07).
In our study, only 38% of participants underwent colonoscopy during follow-up (41% had calprotectin measurement).
My thoughts on this study:
The COMMIT study Gastroenterol 2014; 146: 681-88 found similar findings with regard to infliximab (see blog post: Digging into the COMMIT Study). In this study, MTX with IFX was not superior to monotherapy but did result in fewer antibodies and better levels.
With IFX the benefits of combination therapy seem to be minimal in those with good therapeutic levels, S Lega et al. Inflamm Bowel Dis 2019; 25: 134-41, JF Colombel et al. Clin Gastroenterol Hepatol 2019; 17: 1525-32: (blog posts: Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy for IBD?; Combination Therapy Study Points to Central Role of Adequate Drug Levels). In the discussion, the authors note that intensive therapeutic drug monitoring may contribute to better outcomes with infliximab compared to adalimumab. “The observed benefit of combination therapy among adalimumab users was demonstrated in the setting of standard of care TDM. Of note, anti-TNF dose or interval adjustment and TDM were more frequent in infliximab-treated patients than adalimumab-treated patients, likely due to ease of obtaining trough levels during infusions and more flexible dosing.”
My take: Given the increased difficulty monitoring the kids on adalimumab, they are probably better off on dual therapy. My suspicion, though, is that if they had optimized levels, the benefit of dual therapy is probably small and would mirror the findings with IFX.
This position paper regarding dilatation of strictures in Crohn’s disease provides mostly vague advice.
Here are a few examples:
Imaging: “The need for fluoroscopy is dependent on the stricture phenotype and the treating team…The advantage of live imaging is obvious: it provides greater certainty of balloon position and dilatation success; however, it is difficult and impractical in some centers…In simple strictures, where balloon passage and deployment can be performed with reasonable confidence under direct vision,…it is reasonable to dispense with imaging.”
Dilatation Size: “In the recent pediatric case series…a median of 15 mm was used” as a target dilatation….”It is wise to set reasonable goals for dilatation…Inherited wisdom recommended limiting esophageal dilatation to no more than 3 mm per session. However,…subsequently challenged in several studies demonstrating safe dilatation up to 5 mm per session…As an informal rule, the authors limit dilatation to 2 balloon sizes per session which roughly translates to 5-6 mm. An alternative approach…is to dilate to a maximum of three times the initial stricture diameter; however, neither of these approaches are based on any robust data.”
The main clear cut recommendations are to obtain careful consent, expecting a complication rate of ~4% (eg. bleeding, sepsis, perforation), and to have surgical backup.
My take: This “position paper” offers very few positions on management advice and gives little clear guidance in terms of dilating strictures in Crohn’s disease.