Prospective Study n=365 adult patients with post-operative Crohn’s disease. Findings: At first colonoscopy, 109 [29.9%] had recurrence. Male gender (odds ratio [OR] = 1.95), non-White ethnicity [OR = 2.48], and postoperative smoking [OR = 2.78] were associated with recurrence, while prophylactic anti-TNF reduced the risk [OR = 0.28]. Postoperative anti-TNF prophylaxis had a protective effect on anti-TNF experienced patients but not on anti-TNF naïve patients. Among patients without recurrence at first colonoscopy, Rutgeerts score i1 was associated with subsequent recurrence [OR = 4.43]
A Lecoutour et al JPGN 2024; 78:1116–1125. Efficacy of infliximab after loss of response of/intolerance to adalimumab in pediatric Crohn’s disease: A retrospective multicenter cohort study of the “GETAID pédiatrique”
Key findings: In this retrospective study, 27 of 32 patients (84.4%) were still on IFX at 12 months of the switch. Among them, 13 had discontinued ADA because of a LOR, 12 for insufficient response and 2 due to primary nonresponse. At 1 year, 22 patients were in corticosteroid free clinical remission (68.7%).
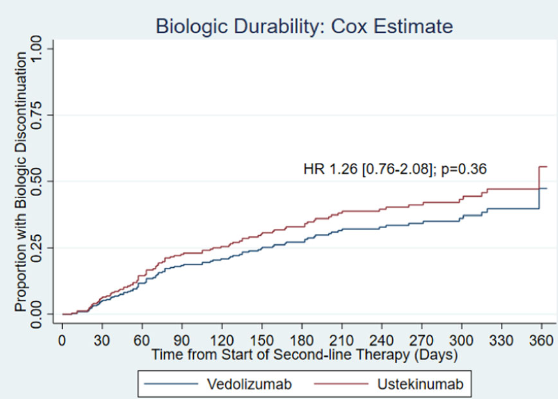
PV Patel et al. JPGN 2024; 78:1126–1134. Real‐world effectiveness of ustekinumab and vedolizumab in TNF‐exposed pediatric patients with ulcerative colitis
Using the ICN registry, this observational study had 262 anti-TNF refractory patients receiving VDZ and 74 patients receiving UST. Key finding: At 6 months, 28.3% of patients on VDZ and 25.8% of those on UST achieved CFCR (p= 0.76)
Methods: Studies included in the current analysis were parallel-group, randomised controlled trials (RCTs) that evaluated treatment with IFX SC, following induction therapy with IFX IV, or treatment with VDZ (either with VDZ IV or with VDZ SC [following IV induction therapy]). The authors identified three eligible CD trials and four eligible UC trials that assigned over 1200 participants per disease cohort to either IFX SC or VDZ.
Key findings:
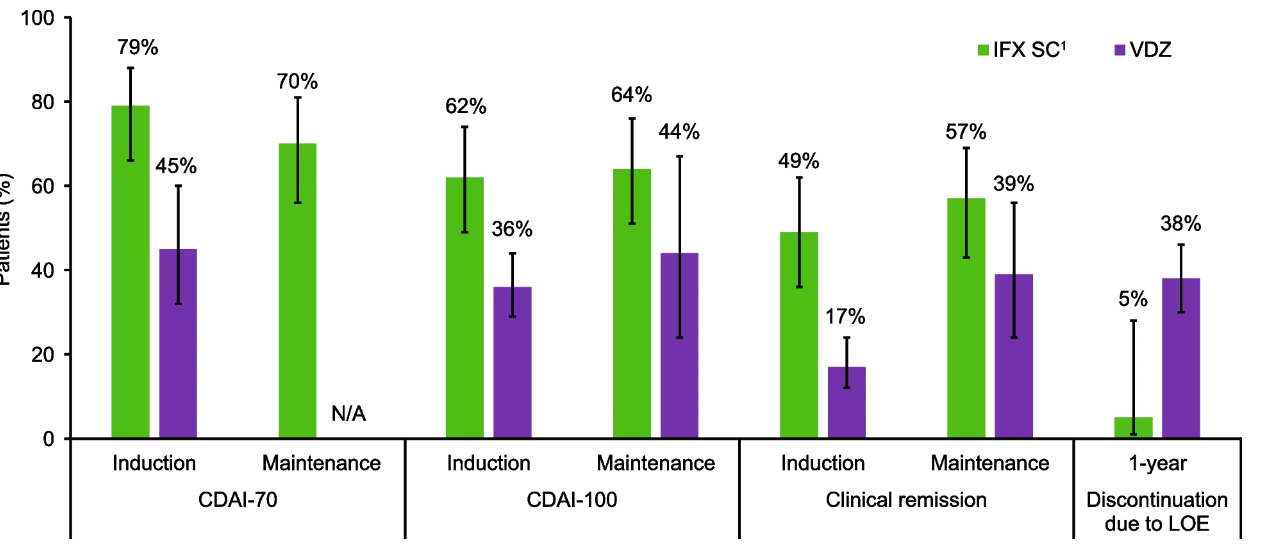
Crohn’s disease: Intravenous induction therapy with IFX demonstrated better efficacy compared with VDZ; during the maintenance phase, IFX SC showed numerically better efficacy than VDZ. A lower proportion of IFX SC-treated patients discontinued therapy due to lack of efficacy over 1 year.
Comparison of IFX SC versus VDZ for key efficacy outcomes in patients with Crohn’s disease
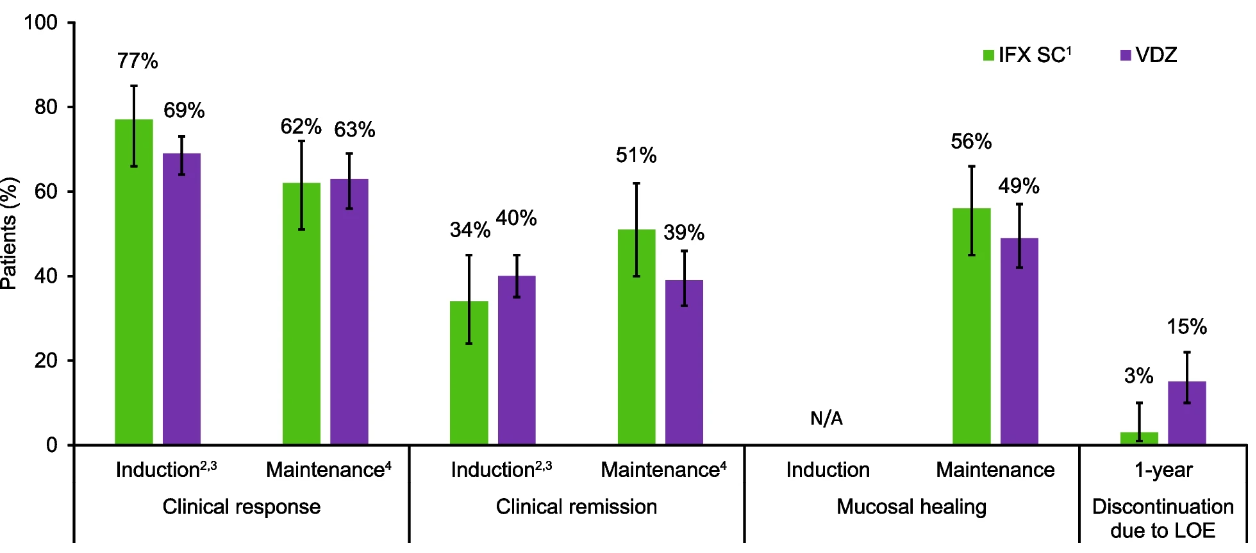
Ulcerative colitis: Efficacy profiles were similar with IFX SC and VDZ during the induction and maintenance phases, and a lower proportion of IFX SC-treated patients discontinued therapy due to lack of efficacy over 1 year.
Comparison of IFX SC1versus VDZ for key efficacy outcomes in patients with ulcerative colitis
Safety: In both cohorts, safety profiles for IFX SC and VDZ were generally comparable during 1 year.
Discussion Points:
The authors discuss some limitations of their study. “The GEMINI I, GEMINI II, and VISIBLE 1 trials were rated as being at high risk of bias for the category ‘other’ bias, because only patients who achieved a clinical response during induction went on to participate in the maintenance phase, which could potentially lead to a higher estimate of efficacy during the maintenance phase than if patients who did not achieve a clinical response were also included.”
The vedolizumab studies notably included a high proportion of patients who failed to respond to anti-TNFs. “All VDZ studies permitted enrolment of patients with prior TNFi failure, accounting for 47.5% of VDZ-treated patients overall.” Thus, in a true head-to-head study with patients unexposed to biologics, VDZ may achieve better results.
My take: This study indicates that SC infliximab (like IV infliximab) appears to be more effective than vedolizumab for patients with Crohn’s disease and similarly effective for ulcerative colitis, keeping in mind the aforementioned discussion points. While not evident in this study, vedolizumab has a superior safety profile.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Dr. Joel Rosh gave our group an excellent update on sequencing therapy for ulcerative colitis (UC). My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of his slides.
There are only two FDA-approved biologics in pediatric Ulcerative Colitis. It typically takes 8-10 years for a medication with approval in adults to receive FDA approval in children
The concept of IBD as two diseases, Crohn’s disease and UC, is flawed; there are more than 200 susceptibility genes for inflammatory bowel disease
There has been an increasing incidence and prevalence of IBD. Some of this increase is likely due to our diet and its effects on the microbiome
Ultrasound is a nice tool to see what is going on in real time and shows that UC is really a transmural disease. UC changes in the bowel can result in fibrosis
Consider cytokine-basis for disease as a way to conceptualize disease presentation compared to organ-based disease. Many autoimmune diseases (eg. JIA, RA, Psoriasis) are different manifestations related to cytokine-based autoimmunity
Almost all pediatric IBD can be considered higher risk based on known risk factors including disease extent (>80% of pediatric UC is pancolitis) and disease age of onset
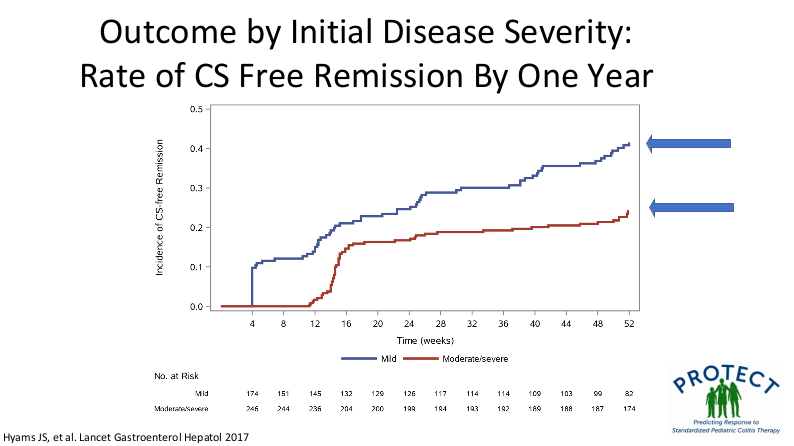
Mesalamine steroid-free clinical remission rates are about 1/3rd after 1 year of treatment
Overall, there has been an improvement in colectomy rates since 2001; there still appears to be a bump in the colectomy rate after having UC for more than 10 years
Elevated CRP is less common in patients with UC, compared to Crohn’s disease, and is a marker for more severe disease activity
Dr. Rosh prefers to avoid some terms including biologic-naive and steroid failure; he favors biologic-unexposed for the former. For the latter, he tries to make it clear that the patient was not a steroid failure. Steroids failed the patient rather than the patient failing the steroids
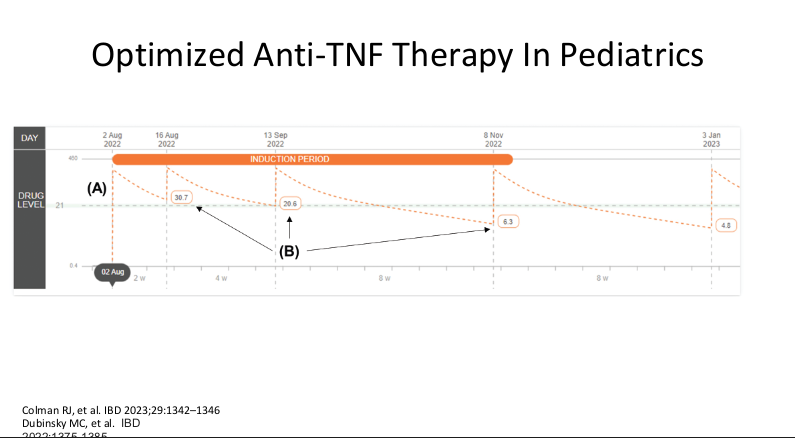
Therapeutic drug monitoring (TDM) is mainly beneficial for anti-TNF agents at this time. Use of TDM can help monotherapy achieve similar results as combination therapy. For infliximab, Dr. Rosh’s ‘rule of thumb’ is 28-18-8 for 2 week trough, 6 week trough, and maintenance trough. Therapeutic levels will meet or exceed these trough levels.
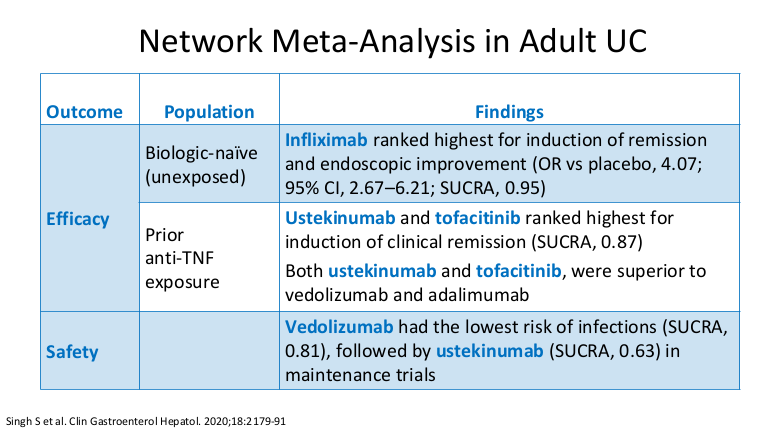
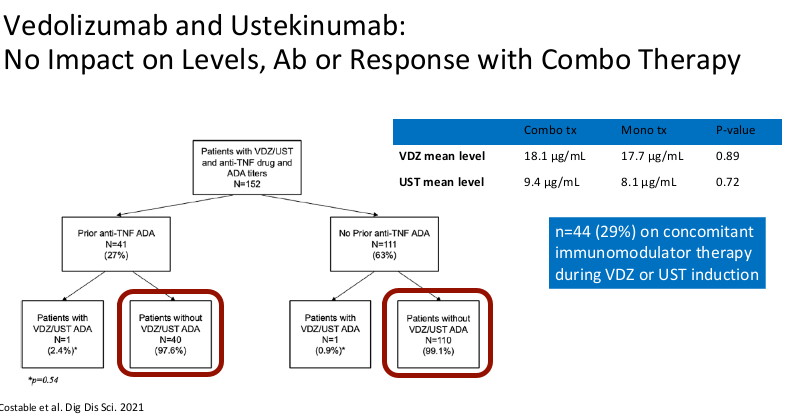
Combination therapy has not been shown to improve pharmacokinetics for vedolizumab or ustekinumab
Generally, a washout period is not needed when changing biologic therapies. In fact, having some overlap in the medications may have some therapeutic benefit
Upadacitinib (Rinvoq) appears to be the most effective JAK for IBD. It is labelled for use as a 2nd-line agent but may be superior for some sicker patients. Rinvoq could be considered as a ‘bridge’ medication in patients with acute severe ulcerative colitis with transition to another biologic like vedolizumab
It is important for families to be informed that there is a black box warning for the use of JAK inhibitors. However, major cardiac adverse events (MACE) do not appear to be increased in patients without preexisting cardiac disease risk factors
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Congratulations to my colleagues at Emory who led/participated in this study.
This study examined 5-year longitudinal data from the pediatric multicenter RISK cohort (n=1075). RISK=risk stratification and identification of immunogenetic and microbial markers of rapid disease progression in children
Key findings:
For children with a low BMIz at diagnosis (n = 294), BMIz normalization within 6 months of diagnosis were associated with a decreased risk for surgery (HR 0.47). Patients without BMIz normalization were enriched for genes in cytokine production and inflammation.
Unsurprisingly, baseline B2 (stricturing disease) and B2+B3 (stricturing and penetrating disease) were associated with increased risk of surgery with HR, 4.20 and HR, 8.24 respectively
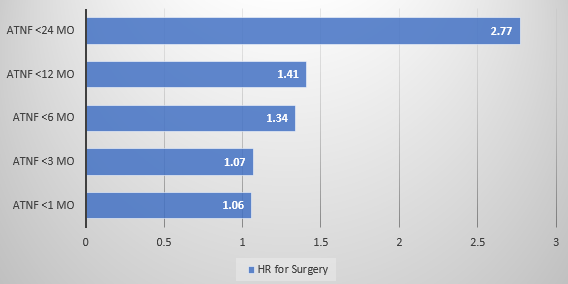
Earlier anti-TNF therapy was associated with a lower hazard rate (HR) of needing surgery
My take: It appears that early anti-TNF therapy lowers the risk of surgery. Improved BMI with treatment is another good prognostic variable. There may be an early window in which effective treatment prevents long-term damage to the GI tract in pediatric patients with Crohn’s disease.
In this observational retrospective study with 40,693 patients: 93% anti-TNF, 3% UST (ustekinumab), and 4% VDZ (vedolizumab), “Anti-TNF therapy was associated with a lower risk of LPD and PPD [luminal and perianal penetrating disease] compared with VDZ, and lower risk of LPD compared with UST.”
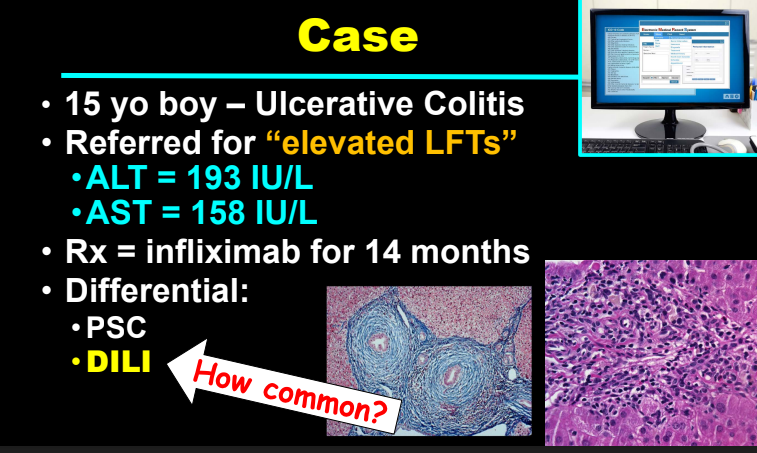
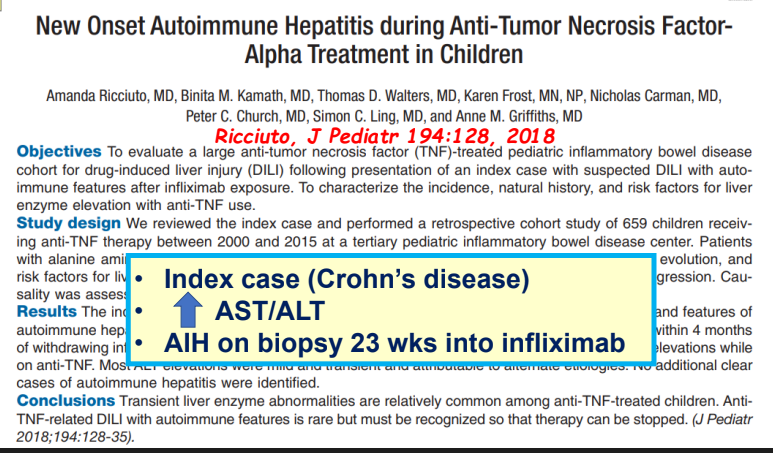
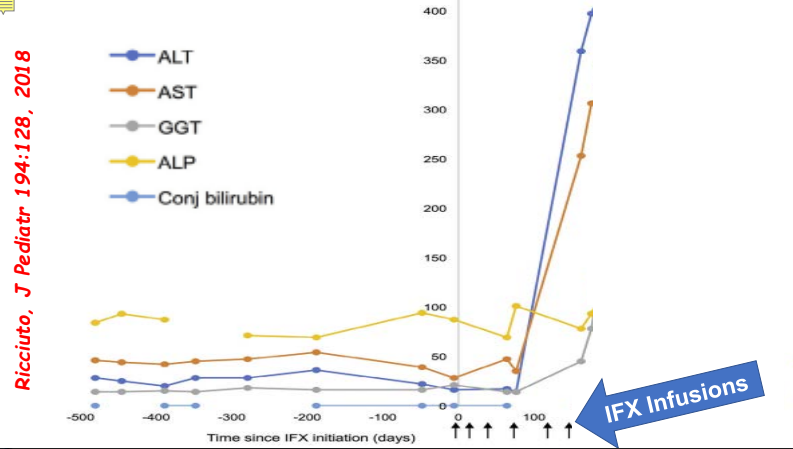
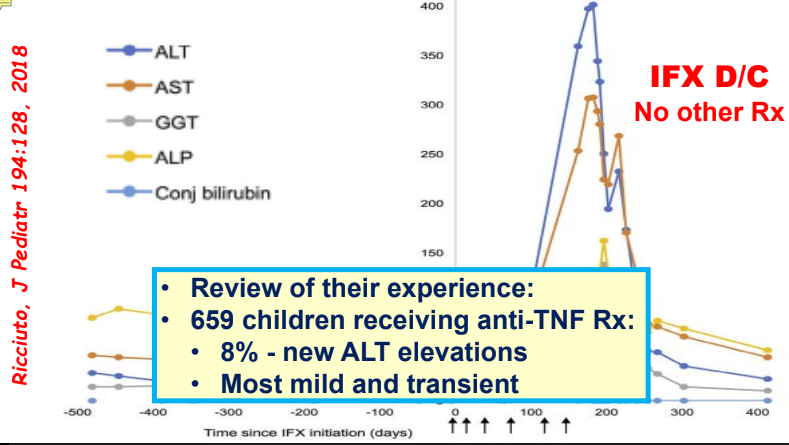
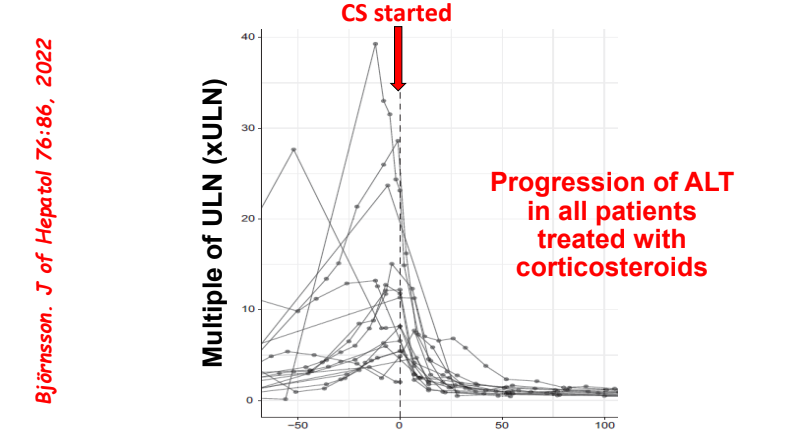
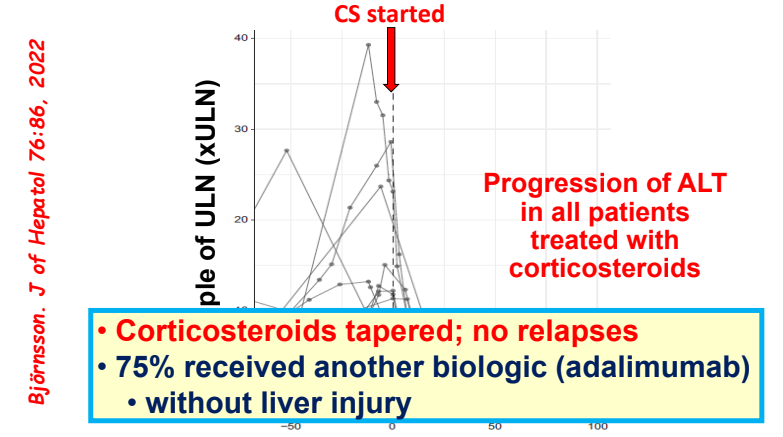
Yesterday’s post highlighted immune-mediated disorders likely caused by anti-TNF therapy; this includes rheumatoid arthritis, psoriasis, hidradenitis suppurativa, and chronic recurrent multifocal osteomyelitis. Anti-TNF inhibitors can be the reason for drug-induced liver disease (DILI) including autoimmune hepatitis (AIH) as well.
In one study, 8% of children receiving anti-TNF therapy developed a new elevation in ALT.
Most often liver enzyme elevation is mild and transient
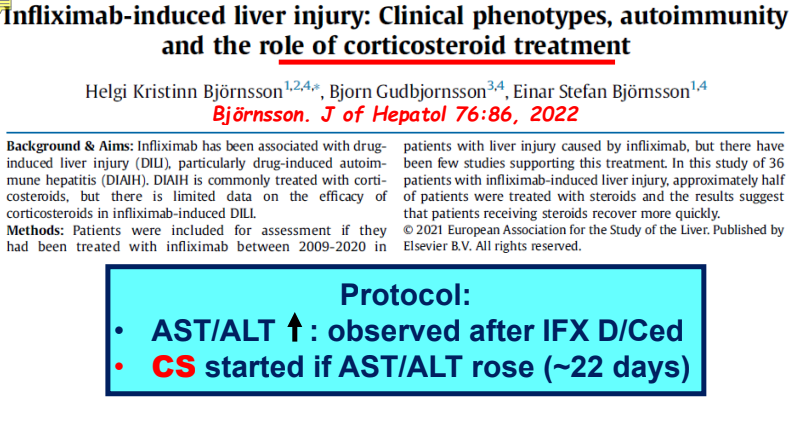
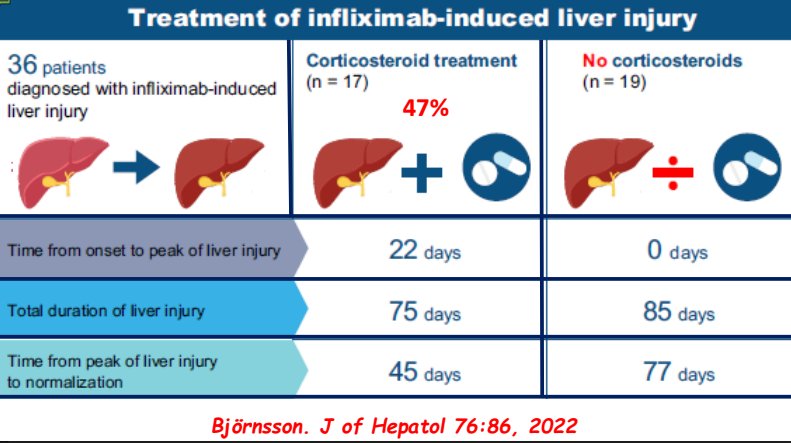
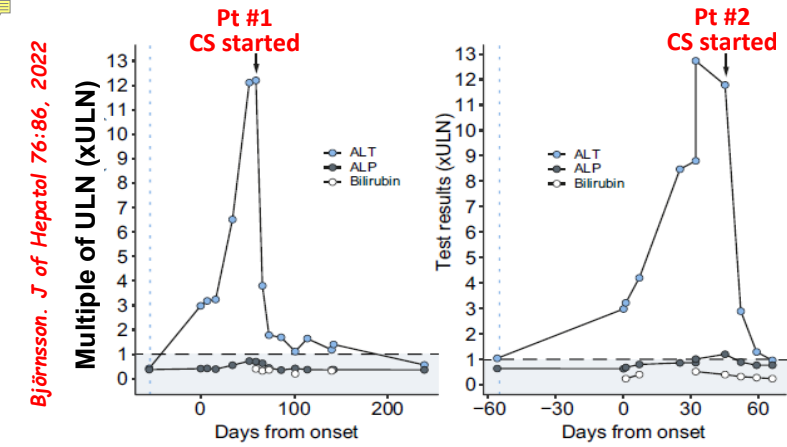
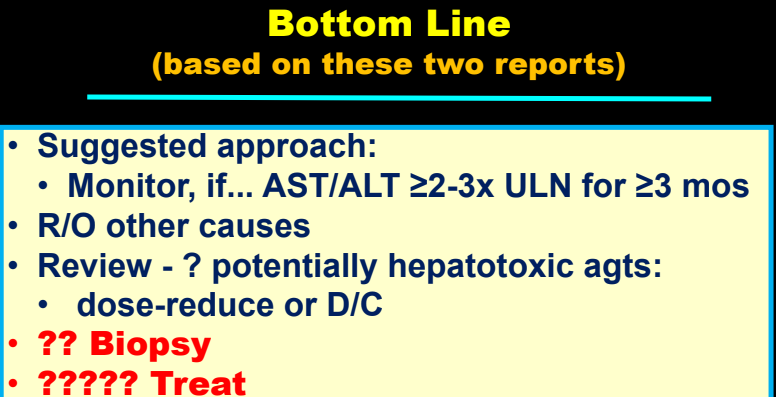
Differential diagnosis for persistent elevation can be due to DILI, autoimmune liver disease (eg. PSC, AIH), or rarely due to a combination (autoimmune drug-induced liver disease). The latter can improve with drug cessation and with corticosteroid treatment.
Some slides on this topic (courtesy of William. Balistreri):
My take: Serious liver injury related to anti-TNF therapy is rare. When liver enzymes are persistently elevated, consider DILI including anti-TNF agents.
Related blog posts:
Autoimmune Hepatitis Associated with Anti-TNF Therapy. Serious liver injury related to anti-TNF therapy is rare. A great place to understand the spectrum of liver problems potentially related to infliximab is the livertox website
The authors performed population pharmacokinetic (popPK) simulations to determine optimal dosing recommendations.
Key points:
Infliximab: “The Q2W SC dosing regimen of infliximab has been selected with the purpose of exceeding a C,trough,ss of 5 mg/L.” This tends to align with 5 mg/kg Q8W IV dosing.
Infliximab: “Patients on Q6W or Q8W IV infliximab can safely switch to Q2W SC infliximab…only patients on Q4W IV infliximab need Q1W SC dosing”
Vedolizumab: “Only patients on Q4W IV vedolizumab should switch to Q1W SC dosing”
Both agents: “Switching 4 instead of 8 weeks after the last IV dose can hit SS[steady state] faster, thereby avoiding the risk of temporary underexposure.”
My take: It is still important to see how switching from IV to SC route affects clinical outcomes in real-world cohorts. This study, though, does provide a good starting point when trying to provide the right dose frequency to achieve good therapeutic troughs.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
JB McCannon et al. NEJM 2023; 389: 1902-1911. Case 35-2023: A 38-Year-Old Woman with Waxing and Waning Pulmonary Nodules
In this case report, A 38-year-old woman was evaluated because of dyspnea, chest discomfort, and waxing and waning pulmonary nodules. She had a prior history of ulcerative colitis. This article reviews reasons for pulmonary nodules including cancer, infection, vasculitis, connective tissue disorders, sarcoidosis and inflammatory bowel disease (IBD) which has a number of pulmonary manifestations including necrobiotic nodules.
In this case, the granulomatous lung disease was attributed to be an extraintestinal manifestation of IBD. She was treated with TNF-alpha targeted therapy which has been effective in a prior case report (J Crohns Colitis 202; 14: 480-489).
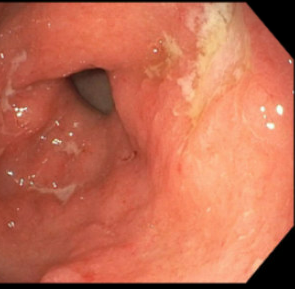
My first reaction to this article — I have seen this! However, our case was atypical in that the 15 year old patient presented with respiratory symptoms (no preceding GI diagnosis). It was noted that her gastric wall was severely thickened as an incidental finding on her chest CT which showed extensive tiny pulmonary nodules. Her endoscopy showed disease isolated to her stomach. Both her gastric findings and CT of her chest resolved with infliximab treatment. This included mucosal healing of her stomach on followup endoscopy.
CT scan showing severely thickened gastric wallMucosal appearance of stomach with erythema and numerous ulcerations prior to treatment
Related blog post: IBD Update January 2015 (Part 1)NEJM 2014; 371: 2418-27 -case report of 9 yo with Crohn’s Disease and pulmonary nodules
On meta-analysis of 13 studies (3756 patients; median follow-up, 12 months; 41% with variants), HLA-DQA1∗05 variants were associated with 75% higher risk of immunogenicity compared with non-carriers (relative risk, 1.75) with considerable heterogeneity (I2 = 62%) (low certainty evidence).
In addition, patients with HLA-QQA1*05 variants had clinical loss of response (LOR) in 67% compared to 30% in those without this variant (wild-type); thus, a 124% higher risk of LOR.
Positive and negative predictive values of HLA-DQA1∗05 variants for predicting immunogenicity were 30% and 80%, respectively
Proactive therapeutic drug monitoring, but not concomitant use of IMMs, IMIDs, and TNF-α antagonist-type, modified this association.
My take:
The ~40% of individuals with HLA-DQA1*05 variants are at higher risk of LOR and are more likely to benefit from both therapeutic drug monitoring and probably from use of combination (with immunomodulator) therapy.
The positive predictive value (30%) is low indicating that the majority of patients with these variants will not develop anti-drug antibodies within 12 months.
In those with negative testing for HLA-DQA1*05 (~60%), the higher negative predictive value indicates a patient is more likely to do well with monotherapy.
HLA-DQA1*05 testing is available commercially (usually part of Celiac HLA typing).
This is the Initiation Well at Quinta da Regaleira in Sintra, Portugal. It is pretty cool because it seems to start at ground level and then goes down many floors. There is an exit to a number of tunnels at the lower level.
Briefly noted: Case report of a 17 yo with Crohn’s disease who developed urticaria and pruritus approximately 6 hours after her very first infliximab infusion; the patient was diagnosed with Alpha-Gal and responded to change to adalimumab which is not glycosylated with alpha-gal.
Sigal Music Museum (Greenville, SC) -has a large number of very old harpsichords and pianos. A harpsichord plucks strings to make the sound whereas a piano has a small hammer that strikes the strings to make the sound. This musical instrument is a harpsichord.
Methods: A systematic search was conducted from August 1999 to July 2021 for studies (50 studies identified) reporting loss of response and dose escalation during infliximab and/or adalimumab use in ulcerative colitis patients with primary response
Key findings:
Annual loss of response was 10% for infliximab and 13% for adalimumab, with higher rates during the first year.
The annual LOR incidences were higher during the first 65 weeks of treatment for both IFX (14%) and ADA (23%).
Annual dose escalation rates were 14% (infliximab) and 21% (adalimumab), with clinical benefit in 72% and 52%, respectively
Key finding: 4 patients (age 18-25 yrs) received upadacitinib for acute severe ulcerative colitis (ASUC) after failing to respond to infliximab and IV steroids. 3 of 4 responded to treatment (45 mg/day) between 4 to 8 days. Three months later, two of these patients were in steroid-free clinical-endoscopic remission and one had maintained a clinical response.
In their discussion, the authors note a similar response rate to tofacitinib, another JAK inhibitor, for ASUC; though, the authors speculate that upadacitinib may be efficacious.
In a a prospective cohort study of 133,137 individuals between the ages of 20 and 80 from 24 countries, the authors examined the relationship between exposures to antibiotics, NSAIDs and hormonal therapies with the development of IBD over a median 11 year period.
Key findings:
Incident IBD was associated significantly with baseline antibiotic (aOR, 2.81; P = .0001) and hormonal medication use (aOR, 4.43; P = .001).
Nonsteroidal anti-inflammatory drug users also were observed to have increased odds of IBD (aOR, 1.80 P = .002), which was driven by long-term use (aOR, 5.58; P < .001)