A total of 46 studies fulfilled the eligibility criteria, comprising approximately 8 million participants from 21 countries.
Key findings:
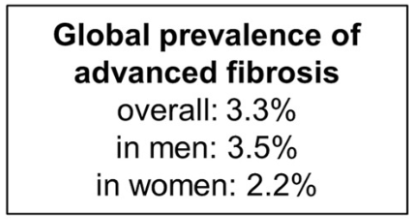
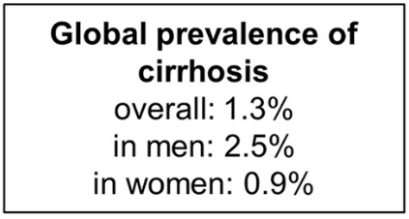
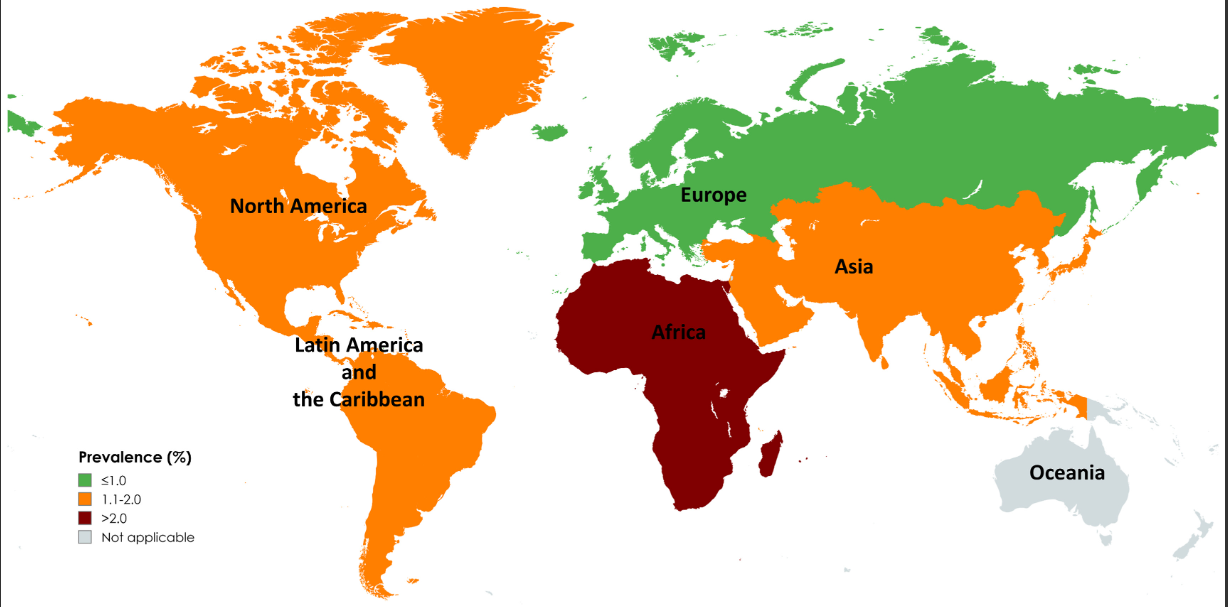
The pooled prevalence rates of advanced liver fibrosis and cirrhosis in the general population were 3.3% (95% CI, 2.4%–4.2%) and 1.3% (95% CI, 0.9%–1.7%) worldwide, respectively
Risk factors for cirrhosis were viral hepatitis, diabetes, excessive alcohol intake, obesity, and male sex
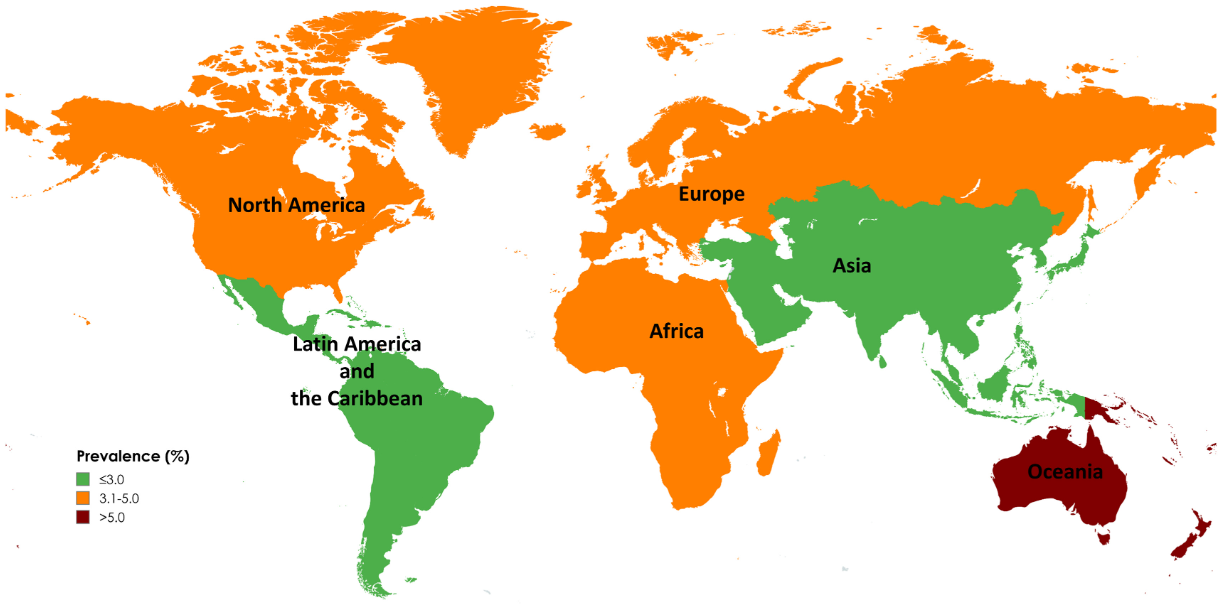
Limitations: 1. All included studies used noninvasive tests to diagnose advanced fibrosis and cirrhosis, which might overestimate prevalence in general populations. The diagnostic performance of these tests is influenced by baseline prevalence, leading to a higher rate of false positives in low-prevalence populations 2. Significant differences in prevalence by geographic region and time period. However, these differences could be influenced by variations in health care infrastructure, access to health care, and disease awareness, which may only partially reflect the true prevalence of advanced liver fibrosis and cirrhosis. In addition, the data is influenced by the number of studies (eg. Oceania had only 1 individual study).
Map of Global Prevalence of Advanced FibrossiMap of Global Prevalence of Cirrhosis
My take: This study provides estimates of the high and increasing prevalence of advanced liver fibrosis and cirrhosis. This data is essential in determining if we are making progress and how to mitigate the disorders leading to advanced liver disease.
From editorial (which is more expansive than the study):
Kappelman et al4 report the US prevalence of pediatric-onset IBD (diagnosed before the age of 20 years by a physician) as well as rates of disease based on race and ethnic background. To ensure that a representative population was captured, they combined multiple health administrative databases…
The authors report that the US currently has a pediatric IBD prevalence of 125 per 100,000 population, increased from 110 per 100,000 in 2011. This is higher than previously reported in Canada (82 per 100,000 in 2023)6 and Sweden (75 per 100,000 in 2010).7These differences may be due to the older age cutoff used in the US data, <20 years vs <18 years in the Canadian and Swedish studies. However, misclassification bias may also play a role...
Nevertheless, understanding the approximate prevalence of pediatric IBD in the US allows for adequate human and financial resource planning for this important population of children with an impactful chronic disease. The high prevalence should raise concerns among health care practitioners and policy makers that we have under-resourced IBD care in children, especially considering the high rate of use of biologics and the growing direct health costs incurred in the treatment of this population.11
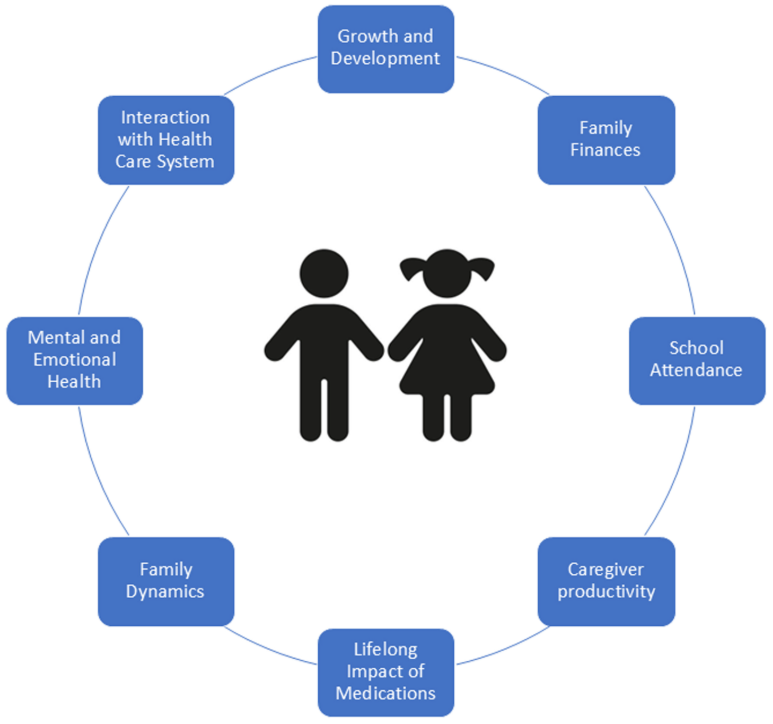
The burden of IBD in pediatrics goes beyond that of the child. Compared with adult IBD, it disproportionately affects caregivers and families (owing to missed work for appointments, hospitalizations, and home care), mental health of both the patient and the parents, and the health system...
They report that pediatric IBD is more frequent among White children and adolescents (145 per 100,000) compared with Black (91 per 100,000) and Hispanic (88 per 100,000) children, whereas children of Asian origin have markedly lower rates (52 per 100,000).“
My take: The updated prevalence data helps understand the increasing frequency of pediatric IBD. The associated commentary reminds us of the broader burden the disease has for families and for our communities.
Methods: Using two large administrative databases, MarketScan and Medicare, the authors estimated annual prevalence of EoE, as well as age- and sex-stratified estimates, standardized to the U.S. population. Health care utilization, including medications and endoscopic procedures, was quantified, and annual EoE-associated costs were calculated.
Key findings:
There was a 5-fold increase in prevalence in both databases since 2009.
Standardized to the U.S. population, the prevalence of EoE was 142.5/100,000, extrapolating to 472,380 cases. This equates to ~1 in 700 persons.
Total EoE-associated annual health care costs were estimated to be $1.32 billion in 2024 dollars after accounting for inflation.
PPIs were used more commonly than steroids for treatment. For Marketscan in 2022, PPIs were used in 41% and steroids in 26%.
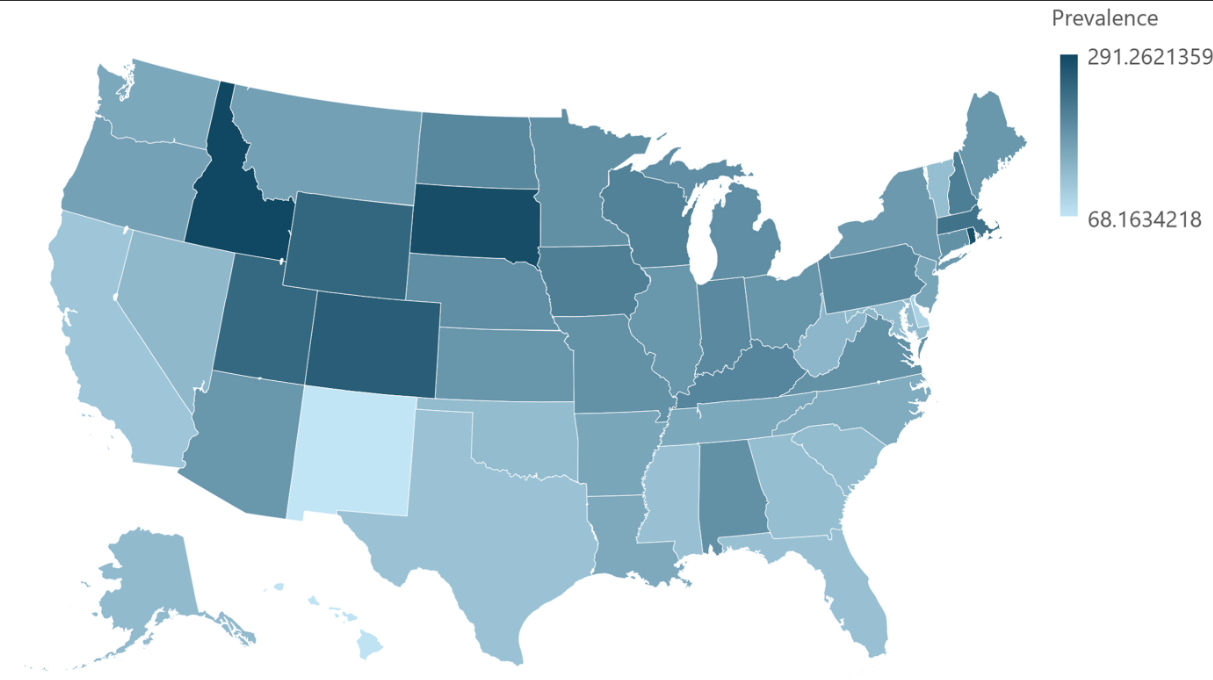
There has been a 5-fold prevalence increase since 2009Prevalence by State. Overall, ~1 in 700 EoE Prevalence in U.S.
My take: There is likely a true increase in the number of affected individuals, though some changes in prevalence are due to an increased recognition/testing of eosinophilic esophagitis.
9698 participants in NHANES during the 2017-2020 cycle completed a transient elastography examination. After excluding patients less than 18 years, these were the key findings:
37.87% had steatotic liver disease
32.45% had MASLD
2.56% had MetALD
1.17% and ALD
Limitations: database study, lack of liver biopsy, reliance on self-reports of alcohol consumption
Methods: 336,866 adults aged ≥30 years were prospectively enrolled in a health screening program between 1997–2013
Key findings:
122,669 (36.4%) had MASLD. Over a mean follow-up of 15 years, 5562 new cases of cirrhosis and 2273 new cases of HCC were diagnosed.
Hazard ratios for HCC were 8.86 for MASLD with HBV or HCV, compared with non-SLD without HBV or HCV
Hazard ratios for HCC were 8.81 for HBV or HCV with non-SLD (SLD), and 1.52 for MASLD without HBV or HCV
My take: MASLD significantly increased cirrhosis and HCC risks; however the risk of HBV or HCV was much greater. The high prevalence rates of MASLD guarantees a huge need for liver disease management for the foreseeable future.
This research utilized 40 studies which met the eligibility criteria, including over 288 million participants and 147,668 patients with EoE from 15 countries across the five continents.
Key findings:
The global pooled incidence and prevalence of EoE were 5.31 cases per 100,000 inhabitant-years and 40.04 cases per 100,000 inhabitant-years, respectively.
The pooled prevalence and incidence of EoE were higher in high-income countries, males, and North America.
The pooled prevalence and incidence of EoE have increased from 1976 to 2022.
Time trends of incidence (A) and prevalence (B) of EoE, 1976 to 2022. Pooled estimates, cases per 100,000 inhabitant-years.
“This review summarizes the data leading to FDA approval for dupilumab and provides a practical approach for clinical use of dupilumab.” Dupilumab, a humanized monoclonal antibody that blocks interleukin (IL)-4 receptor alpha, is currently the only FDA-approved medication for EoE. It is noted that in the trials leading to FDA approval, all patients were PPI refractory and ~70% had received topical steroids (with about half either intolerant or nonresponsive).
Dosing: 300 mg weekly injection with a single-dose prefilled autoinjector pen or a syringe with a needle shield. It is recommended that refrigerated medicine is brought to room temperature for at least 45 minutes prior to injection. It “can remain unrefrigerated up to 14 days.”
In Figure 1, the articles details positioning of use of dupilumab in EoE management algorithm:
New diagnosis, patient preference
Additional atopic condition with approved dupilumab use (strong indication)
Lack of response to current treatment (diet, PPI, swallowed steroids) or adverse effects from current treatment (strong indications)
“It is reasonable to repeat endoscopy with biopsy 24 weeks after initiation of dupilumab in many patients…However, endoscopy may be completer earlier” in selected patients.
At least 5 other biologics are in phase 2 or phase 3 studies (listed in Table 1).
My take: EoE is increasing in prevalence and new therapies (often expensive) are emerging.
Also, there is a fairly good patient education 7-page pamphlet from the makers of Dupixent encouraging patients with symptoms suggestive of EoE to speak with their physicians.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
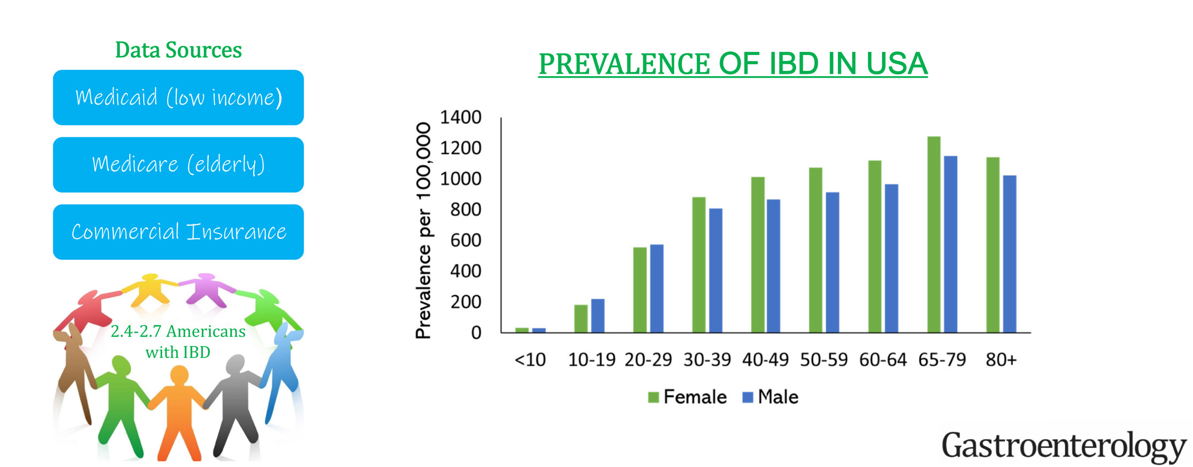
This “INPUT” (INcidence, Prevalence, Treatment and OUTome in Patients with IBD) study used 4 different data sets to provide “the clearest depiction to date of IBD [epidemiology] in the U.S.
Key findings:
The age-, sex- and insurance-standardized prevalence of IBD was 721 per 100,000 population. This equates to estimated 2.39 million Americans with IBD.
Sub-category prevalence: the prevalence of IBD per 100,000 population was 812 in White, 504 in Black, 403 in Asian, and 458 in Hispanic Americans.
My take: The prevalence of IBD continues to increase and the U.S. has one of the highest rates in the world.
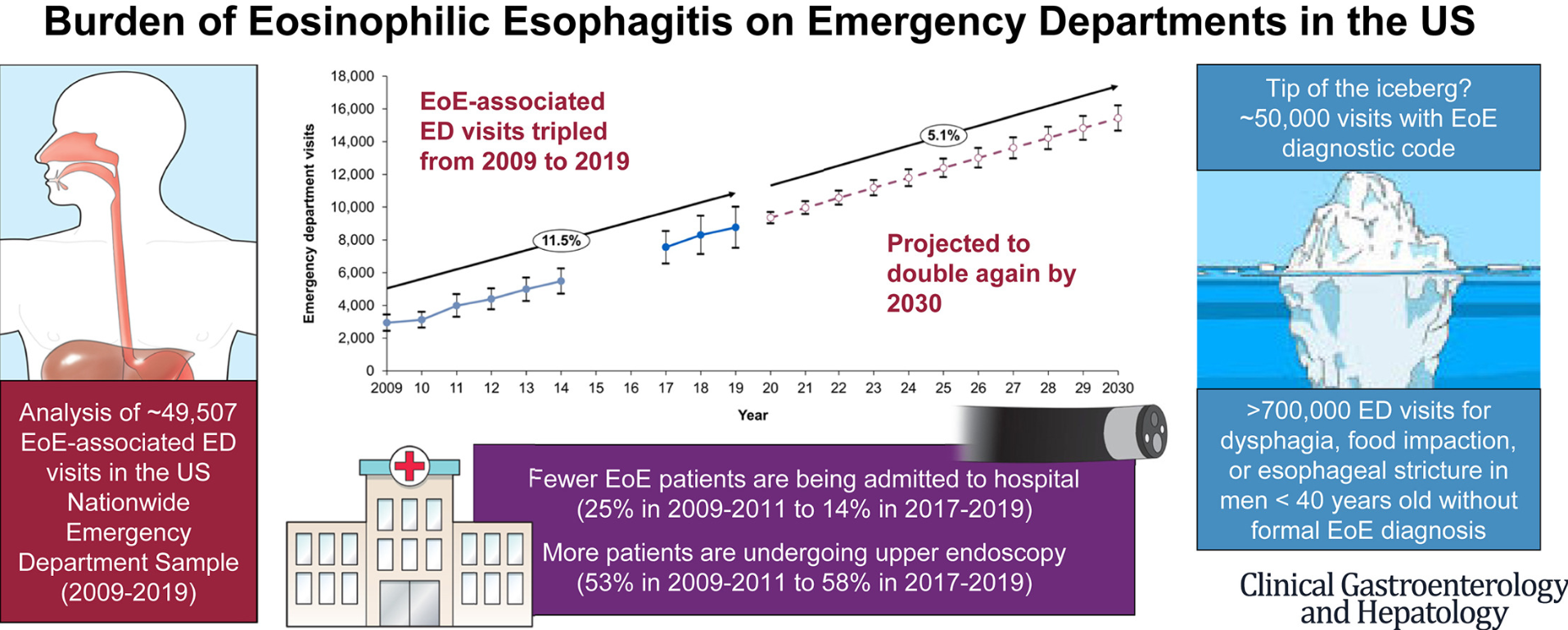
Methods: Data from the US Nationwide Emergency Department Sample (NEDS) were used to estimate weighted annual EoE-associated ED visits from 2009 to 2019. Autoregressive integrated moving average (ARIMA) models were used to project EoE-associated ED visits to 2030. NEDS is a large, publicly available, all-payer ED database in the United States, approximating a 20% stratified sample of US hospital-based EDs.
Key points:
There has been a near tripling of the frequency of EoE-associated ED visits over the course of the past decade which is correlated with an increasing prevalence of EoE. The annual volume of EoE-associated ED visits increased from 2934 in 2009 to 8765 in 2019, and is projected to reach 15,445 by 2030.
Without new interventions, this article projects further increases with doubling again by 2030 (using conservative estimates).
Increasingly EoE is being managed without admission, though average charges associated with ED visits for EoE have tripled since 2009. Total mean inflation-adjusted charges for an EoE-associated ED visit were $9025 US dollars in 2019.
Half of EoE patients presenting to the ED required an endoscopy and 40% required a foreign body/food impaction removal.
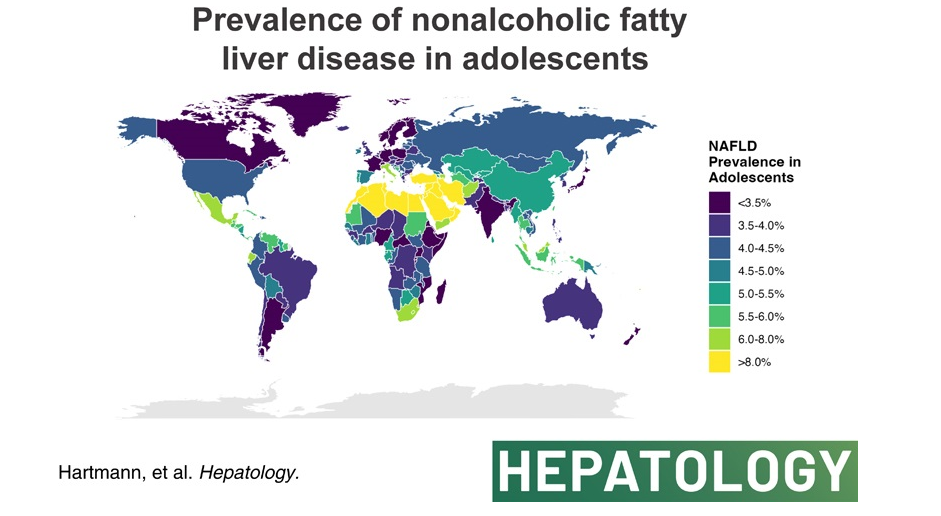
The authors analyzed data from the Global Burden of Disease Study 2019 to compare global, continental, and national prevalence rates of adolescent (15-19 yrs of age) NAFLD.
Key finding:
The global NAFLD prevalence in adolescents increased from 3.73% in 1990 to 4.71% in 2019 (a relative increase of 26.27%). NAFLD is now termed metabolic dysfunction-associated steatotic liver disease (MASLD).
High body mass index and not type 2 diabetes mellitus correlated with NAFLD prevalence in adolescents globally.
In the associated editorial (S Xanthakos, Hepatology78(4):p 1017-1019, October 2023, Rising tide of NAFLD in youth: A warning bell and call to action), some of the key points:
“The Global Burden of Disease (GBD) Study is the most comprehensive and long-standing effort to systematically and scientifically collate data on hundreds of diseases and injuries across the globe, including related clinical outcomes. Beginning in 1990, the GBD Study initially collected data on 106 conditions and 10 risk factors, across 5 age groups.1 Over time, the GBD Study has expanded through serial iterations to involve >9000 international researchers collecting data on 369 diseases and injuries across 204 countries and territories in the most recent 2019 report.1“
” From the GBD Study, we learned that NAFLD is the most rapidly rising cause of chronic liver disease in adolescents and adults,2 and the fastest-growing contributor to cirrhosis, liver cancer, and liver-related deaths globally.”
“The global prevalence of NAFLD in adolescents shows no sign of abating, rather has continued to increase steadily from 3.7% in 1990 to 4.7% in 2019.”
“As with all epidemiological research, the GBD study faces the primary limitation of relying on data sources that employ varying and less accurate measures of NAFLD prevalence (alanine aminotransferase and/or ultrasound primarily). However, the rigorous methodological approach employed by the GBD including frequent assessment of face validity, and the tremendous input of data sources (>80,000 in 2019) nonetheless results in the most comprehensive global data set available.”
My take (borrowed from editorial): Without intervention, “the increase in adolescent NAFLD certainly portends a future increase in NAFLD-related cirrhosis and liver-related deaths in young adults in the coming decades, and a likely escalation in cardiovascular and diabetes-related morbidity.
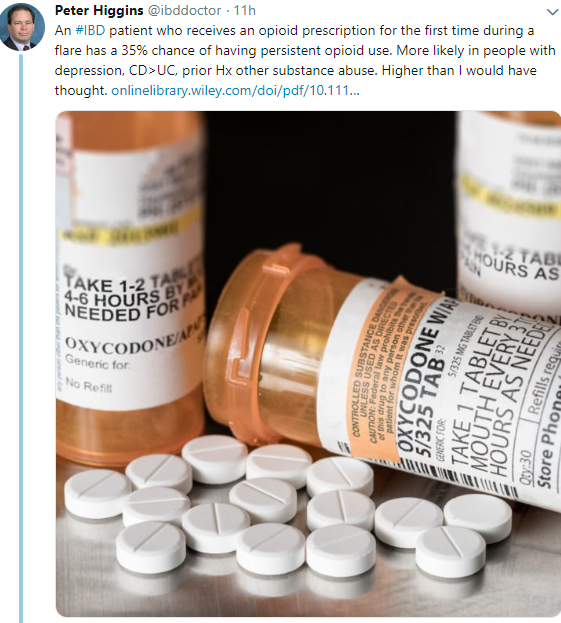
According to a recent study (Full Link: MR Noureldn, PDR Higgins et al. Aliment Pharmacol Ther. 2019;49:74–83. Incidence and predictors of new persistent opioid use following inflammatory bowel disease flares treated with oral corticosteroids), and with the limitation of using an insurance database –Key Findings:
5411 (35.8%) were opioid‐naïve patients (mean age 43.9 yrs) of which 35.0% developed persistent opioid use after the flare
Factors associated with new persistent opioid use include a history of depression (hazard ratio [HR] 1.29, 95% confidence interval [CI] 1.13‐1.47), substance abuse (HR 1.36, 95% CI 1.2‐1.54), chronic obstructive pulmonary disease (COPD) (HR 1.17, 95% CI 1.04‐1.3), as well as, Crohn’s disease (HR 1.26, 95% CI 1.14‐1.4) or indeterminate colitis (HR 1.6, 95% CI 1.36‐1.88)
My take: As noted in previous blog (Increased Narcotic Usage in Pediatric Patients with IBD), opioid usage is an issue with pediatric IBD patients as well, particularly in those with associated depression and/or anxiety.
A recent study (AC Skinner et al. Pediatrics 2018; 141: e20173459) examined obesity prevalence data in children 2-19 years of age from a nationally representative sample (n=3340). Specifically, the authors used NHANES data from 1999-2016. Thanks to John Pohl’s twitter feed for pointing out this reference.
This article is packed with data and breaks down obesity in categories: overweight, class I obesity, class II obesity & class III obesity. It provides data based on gender, age, and ethnicity.
The trend in obesity prevalence is best captured in Figure 1.
Among girls:
In 1999-2000: class I obesity noted in 14.6% –>17.8% in 2015-16
In 1999-2000: class II obesity noted in 4.0% –>5.2% in 2015-16
In 1999-2000: class III obesity noted in 0.9% –>1.8% in 2015-16
Among boys:
In 1999-2000: class I obesity noted in 14.7% –>19.1% in 2015-16
In 1999-2000: class II obesity noted in 4.1% –>6.7% in 2015-16
In 1999-2000: class II obesity noted in 1.0% –>2.0% in 2015-16
My take: This article indicates that the prevalence of childhood obesity in the U.S. is not improving and does not appear to have leveled off as has been suggested by some studies.