I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Methods: Retrospective chart review of 86 patients transplanted between 2003 and 2013
Key findings:
Intestinal graft survival was 71% and 65% after 5 and 10 years, respectively
Five-year graft survival was attained in 79% of patients with a history of anatomic intestinal failure (n=63) compared with 45% with functional intestinal failure (n=22) (P = 0.0055).
In their cohort, graft-versus-host and post-transplant lymphoproliferative disease were 11 times greater and 8 times greater in the functional compared with anatomic intestinal failure group. “Severe functional gastrointestinal diseases are more likely to be component of inherited multisystem disorders not fully correctable with ITx (intestinal transplantation) alone.”
Graft survival depends on avoidance of severe infectious and immunological complications including GVHD, whereas inclusion of a liver graft provides no obvious survival benefit
My take: In this cohorts, intestinal transplantation outcomes have improved for anatomic intestinal failure but not for functional intestinal failure. “Reduced success with functional intestinal failure may reflect inherently increased susceptibility to complications in this group.”
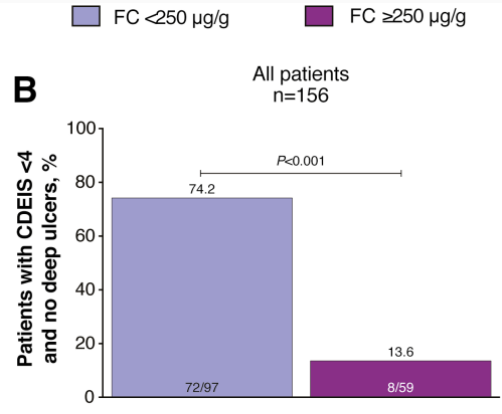
The proportion of patients who achieved the primary end point CDEIS <4 and no deep ulcers was significantly greater for those with FC <250 µg/g (74%; P < 0.001)
Fecal calprotectin <250 µg/g, CRP <5 mg/L, and CDAI <150 gave a sensitivity/specificity of 72%/63% and positive/negative predictive values of 86%/42% for CDEIS <4 and no deep ulcers 48 weeks after randomization
My take: Fecal calprotectin levels are useful for monitoring mucosal healing. Levels less than 250 are encouraging. Levels less than 100 are better.
Proportion of patients achieving mucosal healing (CDEIS <4) and no deep ulcers in (B) all patients by FC cutoff at week 48 after randomization
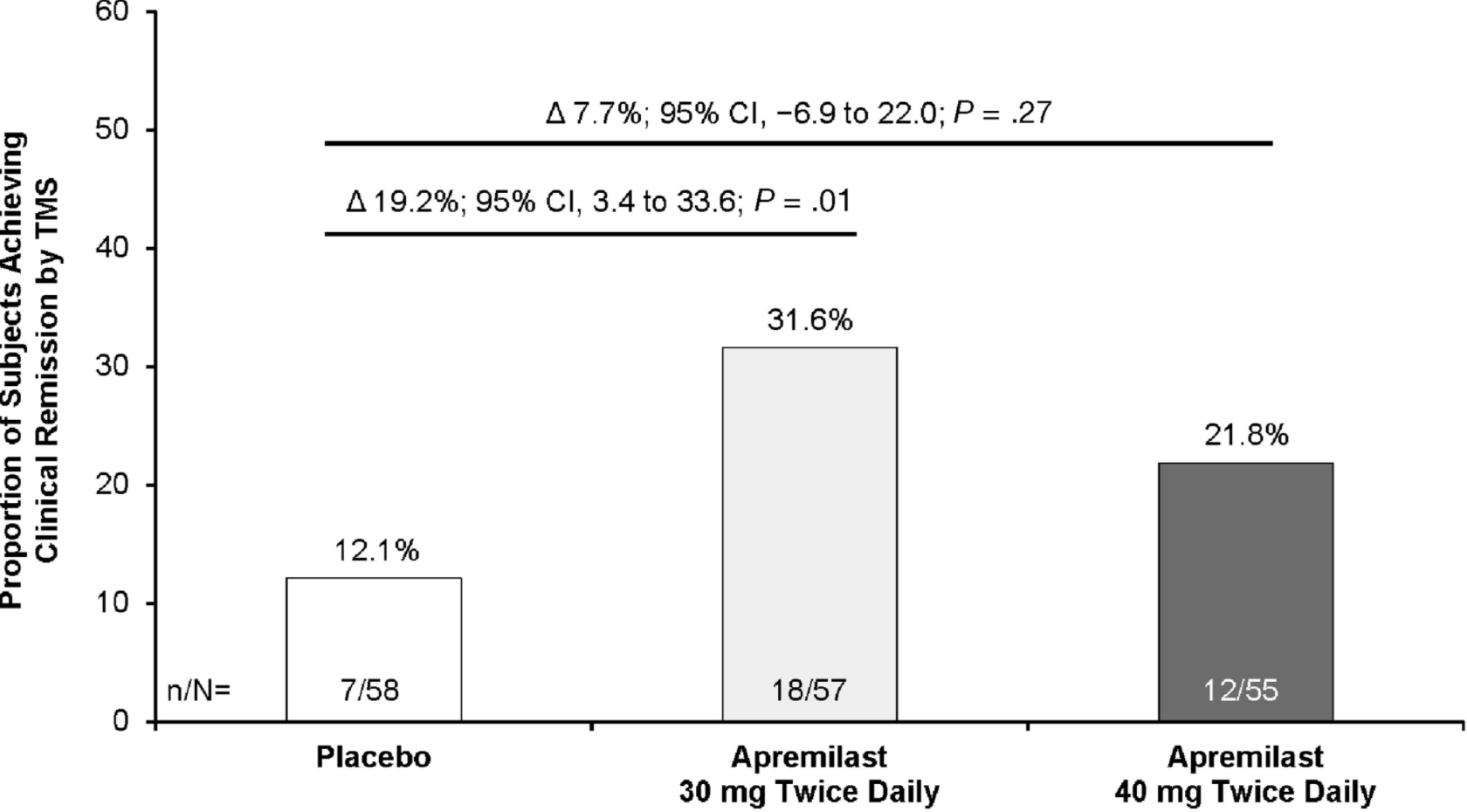
Clinical remission was achieved at week 12 by 31.6% of patients in the 30 mg apremilast group and 12.1% of patients in the placebo group (P = .01). However, only 21.8% of patients in the 40 mg apremilast group achieved clinical remission at week 12 (P = .27 compared with placebo)
At week 52, clinical remission was achieved by 40.4% of patients initially assigned to the apremilast 30 mg group and 32.7% of patients initially assigned to the apremilast 40 mg group.
Methods: Microbiota was prospectively analyzed in 49 patients with active CD at baseline, week 6, and week 30
Key Findings:
Increased proportions of Lachnospiraceae and Blautia were associated with IFX efficacy; the combined increase of these taxa at week 6 showed 83.4% and 84.2% accuracy in predicting clinical response at weeks 14 and 30, respectively, with a predictive value of 89.1% in predicting endoscopic response at week 30
IFX diminished CD-related gut microbial dysbiosis by modifying microbiota composition and function
“We found histologic evidence of UC activity (Geboes score ≥ 2B.1) in biopsies from 182 patients (65%) and endoscopic evidence of UC activity in 149 patients (53%) (substantial agreement, κ = 0.60).”
“Histologic features of UC activity were associated with increased rates of systemic corticosteroid use, colectomy, and hospitalization in the entire cohort (P < .05 for all) and associated with increased rates of systemic corticosteroid use in an analysis limited to patients in endoscopic remission (P < .001).”
At ileo-colonoscopy, 63% of patients had endoscopic healing and 55% had histologic evidence of healing. The level of agreement between endoscopic and histologic activity was fair (62%, K = 0.2250, P = .0064)
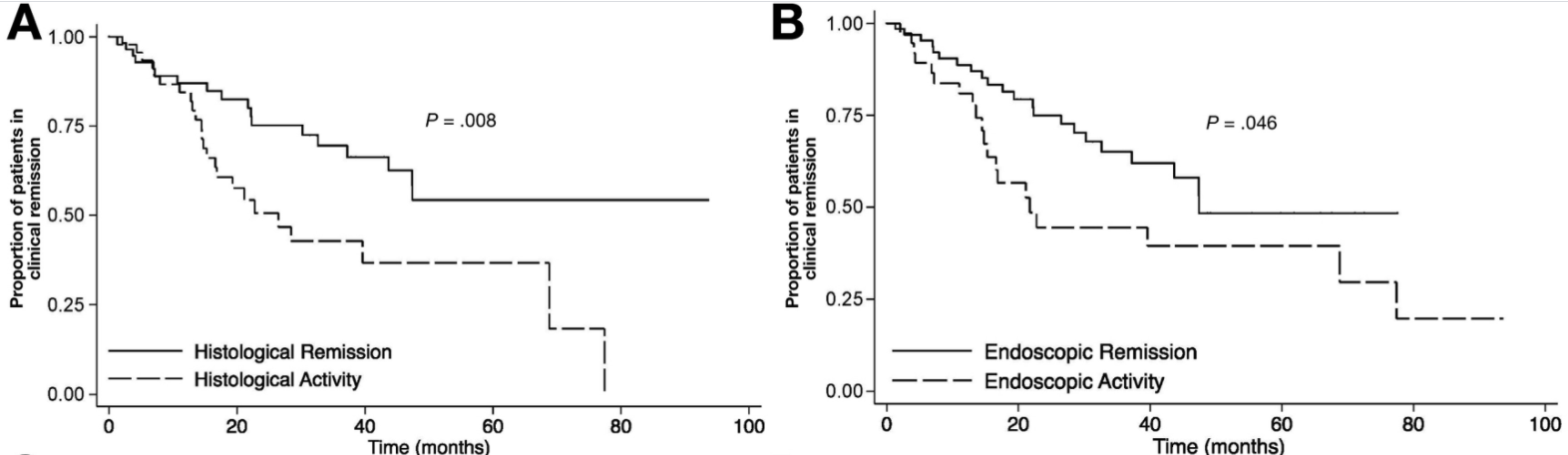
On multivariate analysis, only histologic healing was associated with decreased risk of clinical relapse (hazard ratio [HR], 2.05; 95% CI, 1.07–3.94; P = .031), medication escalation (HR, 2.17; 95% CI, 1.2–3.96; P = .011), and corticosteroid use (HR, 2.44; 95% CI, 1.17–5.09; P = .018).
Kaplan-Meier analysis of effect of endoscopic and histologic activity on (A) clinical relapse-free survival versus histologic healing, (B) clinical relapse-free survival versus endoscopic healing
D Kevans et al. Inflamm Bowel Dis 2020; 26: 1722-1729. Histological Markers of Clinical Relapse in Endoscopically Quiescent Ulcerative Colitis Key finding: In endoscopically quiescent UC (n=76), active histological inflammation …[is] adjunctive histological marker associated with increased likelihood of disease relapse. The associated editorial (1730-32 by Asher Kornbluth) quotes Voltaire: “A wise Italian says that the best is the enemy of the good.” He notes that there is “a very real risk of abandoning an effective drug while chasing the goal of some yet to be universally defined histologic remission.” Currently organizational guidelines (ACG, AGA, ECCO, IOIBD) do NOT suggest the use of histologic normalization as an endpoint at this point.
My take: These studies show that histologic healing in ileal Crohn’s disease and in ulcerative colitis are associated with better outcomes that endoscopic appearance. However, there are a lot questions because many patients, possibly a majority, will not achieve histologic healing despite aggressive treatment. Related technical issues include how many biopsies are needed to assess histology and having a validated histologic assessment.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: AK002 (lirentelimab) is an anti-Siglec-8 antibody that depletes eosinophils and inhibits mast cells.
Methods: In this phase 2 trial, the authors randomly assigned adults (n=65) who had symptomatic eosinophilic gastritis, eosinophilic duodenitis, or both conditions in a 1:1:1 ratio to receive four monthly infusions of low-dose AK002, high-dose AK002, or placebo
Key findings:
The mean percentage change in gastrointestinal eosinophil count was −86% in the combined AK002 group, as compared with 9% in the placebo group
Treatment response (>30% reduction in total symptom score and >75% reduction in gastrointestinal eosinophil count) occurred in 63% of the patients who received AK002 and in 5% of the patients who received placebo
The authors note that AK002 “also resulted in alleviation of dysphagia in patients with a history of concomitant eosinophilic esophagitis.”
Limitations: Small study and 10% developed antibodies to drug
My take: Larger phase 3 studies with AK002 are underway (NCT04322604 & NCT04322708). AK002 looks promising for eosinophilic gastrointestinal diseases.
Change in total symptom score over 14 weeks. “Shown is the least-squares mean percentage change from baseline in total symptom score over time.” The total symptom score ranges from 0 to 80, with higher scores indicating greater symptom severity. Each of eight symptoms are given a score of 0 to 10: abdominal pain, nausea, vomiting, early satiety, loss of appetite, abdominal cramping, bloating and diarrhea.
I did not have the opportunity to hear this #NASPGHAN20 lecture but Dr. Benchimol has shared his slides. Link to Dropbox Slides: IBD Clinical Science: Year in Review
Some of the key points on slides (links to articles below):
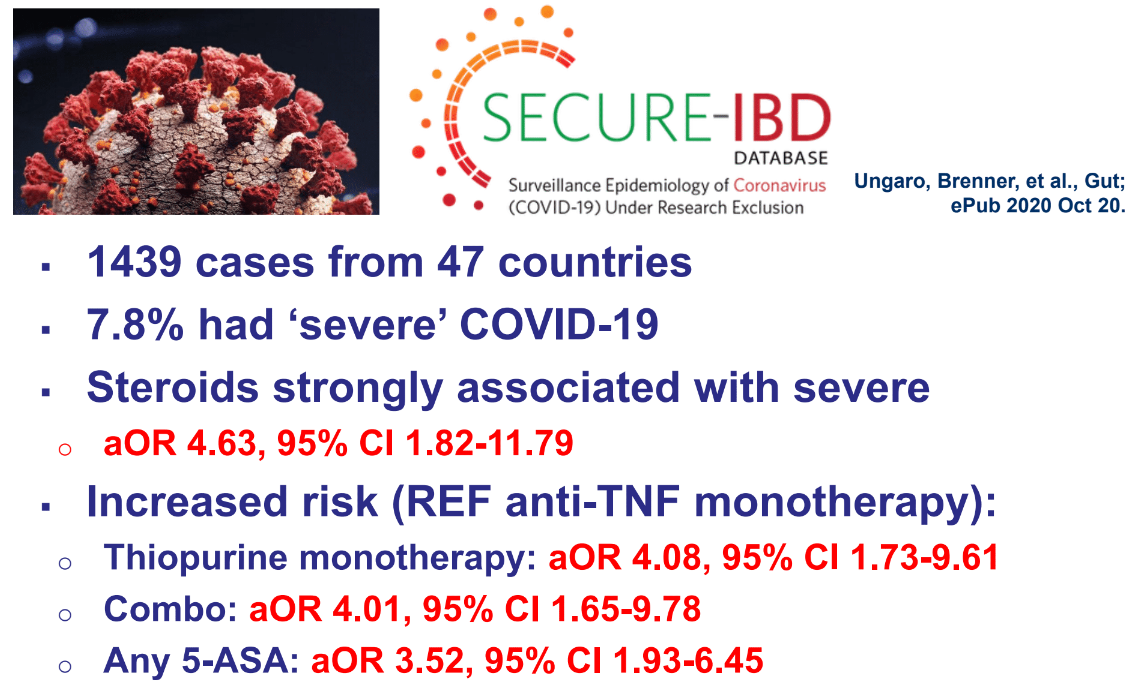
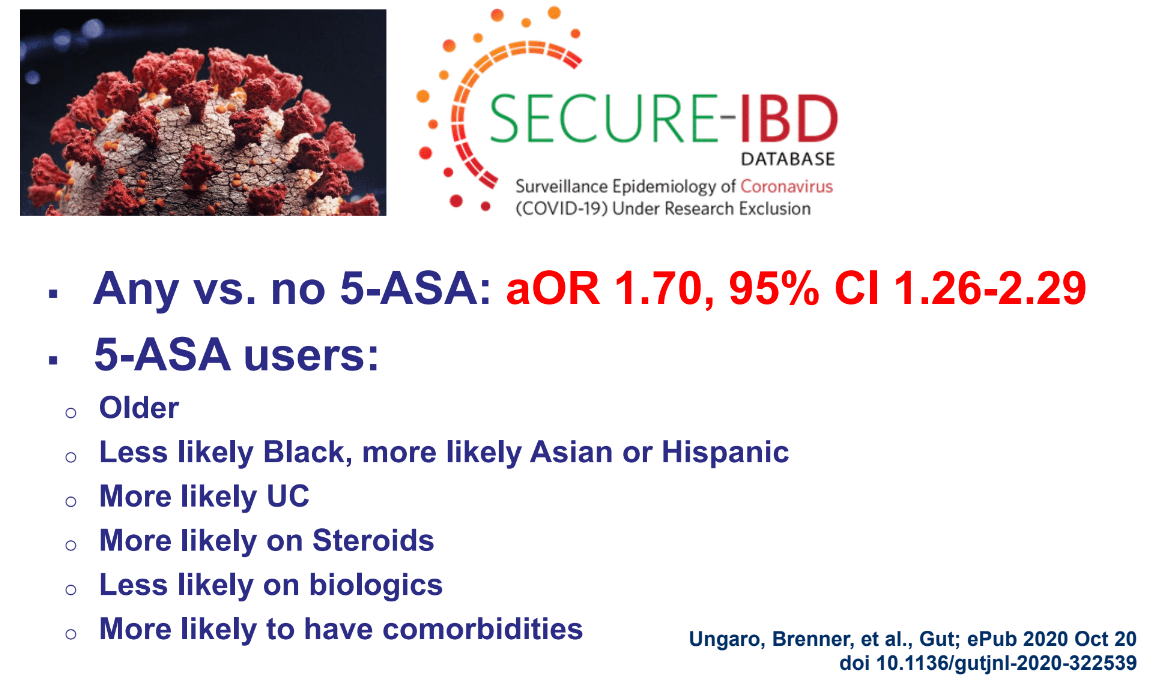
Lots of data on COVID-19 and IBD. Steroids and Thiopurines are associated with more severe disease whereas anti-TNF agents are not
Lower intestinal barrier function is associated with increased risk for development of Crohn’s disease
More greenspace associated with lower rates of development of IBD
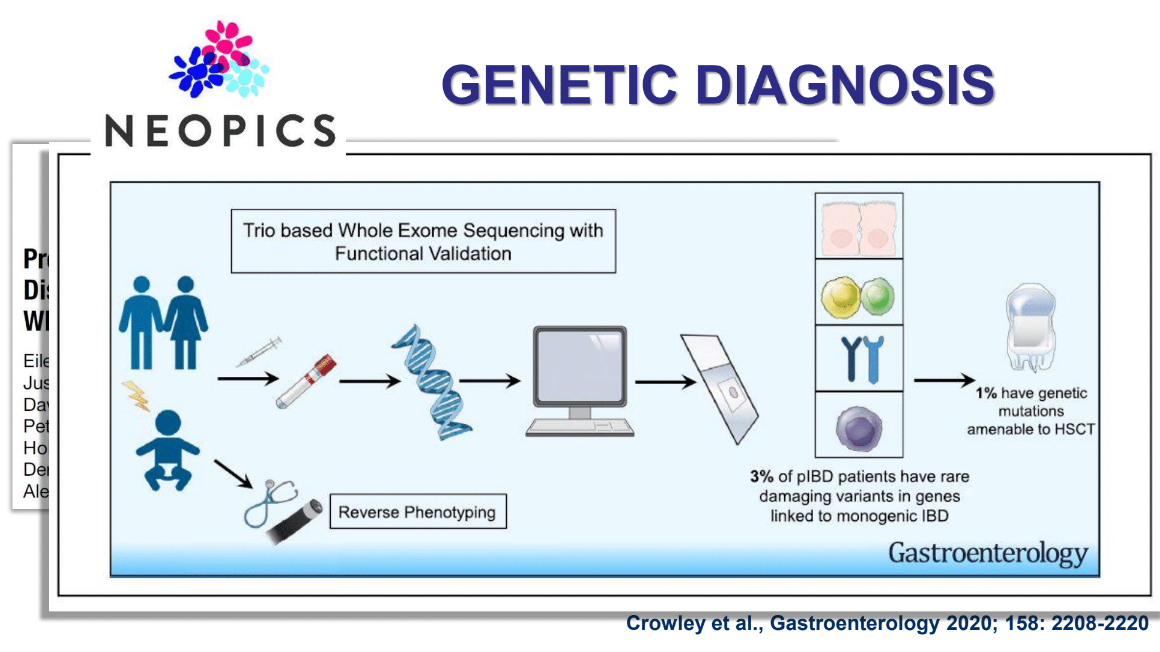
Exome sequencing has shown ~3% of pIBD with genetic mutations linked to monogenetic IBD & 1% with mutations which could benefit from HSCT. Identifying specific defects may lead to other treatments as well (eg. Leflunomide for TTC7A deficiency). Related blog posts:
Early biologic therapy associated with better long-term outcomes in adult and pediatric IBD
Reviewed data on adalimumab showing improvement in growth and relationship between good titers and clinical response (related post: IBD Update -September 2020)
Also, there will be a webinar for both patients and health care providers on November 19 with the SECURE-IBD steering committee as guests to go over the new data.
Aubrey Gordon provides personal insight into the issue of weight stigma in her opinion piece: NY Times Leave Overweight Kids Alone
Here a few excepts:
The war on childhood obesity reached its zenith with the 2010 introduction of the national “Let’s Move!” campaign, “dedicated to solving the problem of obesity within a generation.” It was a campaign against “childhood obesity” — not specific health conditions or the behaviors that may contribute to those health conditions. It wasn’t a campaign against foods with little nutritional value, or against the unchecked poverty that called for such low-cost, shelf-stable foods. It was a campaign against a body type — specifically, children’s body types.
In 2012, Georgia began its Strong4Life campaign aimed at reducing children’s weight and lowering the state’s national ranking: second in childhood obesity. Run by the pediatric hospital Children’s Healthcare of Atlanta, it was inspired in part by a previous anti-meth campaign. Now, instead of targeting addiction in adults, the billboards targeted fatness in children…The billboards purported to warn parents of the danger of childhood fatness, but to many they appeared to be public ridicule of fat kids…
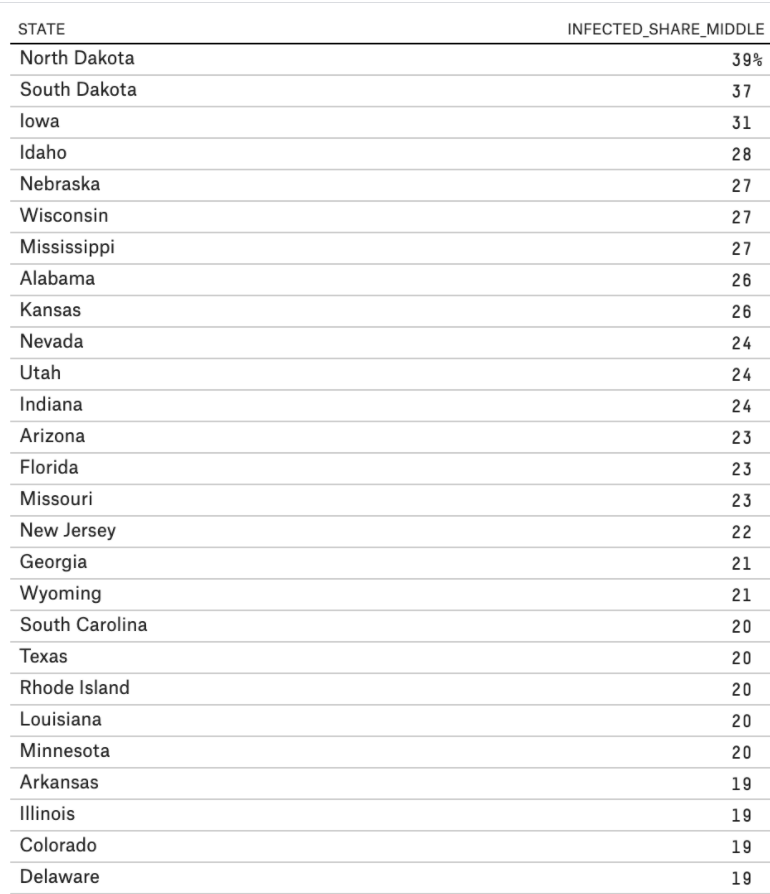
Despite ample federal and state funding, multiple national public health campaigns and a slew of television shows, the war on obesity does not appear to be lowering Americans’ B.M.I.s. According to the Centers for Disease Control and Prevention, since 1999 there has been a 39 percent increase in adult obesity and a 33.1 percent increase in obesity among children.
Weight stigma kick-starts what for many will become lifelong cycles of shame..Yet, despite its demonstrated ineffectiveness, the so-called war on childhood obesity rages on. This holiday season, for the sake of children who are told You’re not beautiful. You’re indulging too much. Your body is wrong. You must have done it, I hope some parents will declare a cease-fire.
Listed below are the 10 ‘Best Practice Advice’ recommendations. I think the acknowledgement that “hemostatic powder should be preferentially used as a rescue therapy and not for primary hemostasis, except in cases of malignant bleeding or massive bleeding with inability to perform thermal therapy or hemoclip placement” (#7) is very useful.
“Best Practice Advice:”
Endoscopic therapy should achieve hemostasis in the majority of patients with NVUGIB.
This may include clips, thermal (heater probes, bipolar/multipolar catheters, hemostatic forceps), diluted epinephrine injection, and hemostatic spray
Initial management of the patient with NVUGIB should focus on resuscitation, triage, and preparation for upper endoscopy. After stabilization, patients with NVUGIB should undergo endoscopy with endoscopic treatment of sites with active bleeding or high-risk stigmata for rebleeding.
Endoscopists should be familiar with the indications, efficacy, and limitations of currently available tools and techniques for endoscopic hemostasis, and be comfortable applying conventional thermal therapy and placing hemoclips.
Monopolar hemostatic forceps with low-voltage coagulation can be an effective alternative to other mechanical and thermal treatments for NVUGIB, particularly for ulcers in difficult locations or those with a rigid and fibrotic base.
Hemostasis using an over-the-scope clip should be considered in select patients with NVUGIB, in whom conventional electrosurgical coagulation and hemostatic clips are unsuccessful or predicted to be ineffective.
Hemostatic powders are a noncontact endoscopic option that may be considered in cases of massive bleeding with poor visualization, for salvage therapy, and for diffuse bleeding from malignancy.
Hemostatic powder should be preferentially used as a rescue therapy and not for primary hemostasis, except in cases of malignant bleeding or massive bleeding with inability to perform thermal therapy or hemoclip placement.
Endoscopists should understand the risk of bleeding from therapeutic endoscopic interventions (eg, endoluminal resection and endoscopic sphincterotomy) and be familiar with the endoscopic tools and techniques to treat intraprocedural bleeding and minimize the risk of delayed bleeding.
In patients with endoscopically refractory NVUGIB, the etiology of bleeding (peptic ulcer disease, unknown source, post surgical); patient factors (hemodynamic instability, coagulopathy, multi-organ failure, surgical history); risk of rebleeding; and potential adverse events should be taken into consideration when deciding on a case-by-case basis between transcatheter arterial embolization and surgery.
Prophylactic transcatheter arterial embolization of high-risk ulcers after successful endoscopic therapy is not encouraged.