I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
This retrospective study from Finland details the bone health of children with biliary atresia (BA). Key findings:
Out of 49 patients, 7 (14%) were diagnosed with rickets during infancy. Clearance of jaundice [odds ratio 0.055, 95% confidence interval [CI] 0.00266–0.393; P < 0.01] was a protective factor against rickets.
In DXA measurements, median lumbar spine aBMD anthropometrically adjusted z-scores were as follows:
in native liver survivors 0.8 (interquartile range [IQR] −1.9 to 1.4) at 5 and −0.3 (IQR −1.3 to 0.8) at 10 years
in liver transplanted patients 0.4 (IQR −0.2 to 1.1) at 5 and 0.6 (IQR −0.1 to 1.3) at 10 year.
Most BA patients have aBMD within normal range between 5 and 10 years of age irrespective of liver transplantation status.
My take: This study shows that early in life there is frequent bone impairment in children with BA. This generally improves in most children as cholestasis resolves (with or without liver transplantation).
This was a small study with 15 patients, with 9 patients having very elevated fecal calprotectin (FC) (>250) and the median level was 713 mcg/g for the entire cohort at baseline. After treatment with lumacaftor/Ivacaftor, median FC level was 102 mcg/g.
This pilot study is intriguing and makes the point that intestinal inflammation is commonly seen in children with cystic fibrosis. However, this study has some striking differences from prior studies.
My take: This study suggests that Lumacaftor/Ivacaftor is associated with a significant decrease in intestinal inflammation. When one looks at prior studies, the FC values presented in this study at baseline are much greater which could indicate significant selection bias.
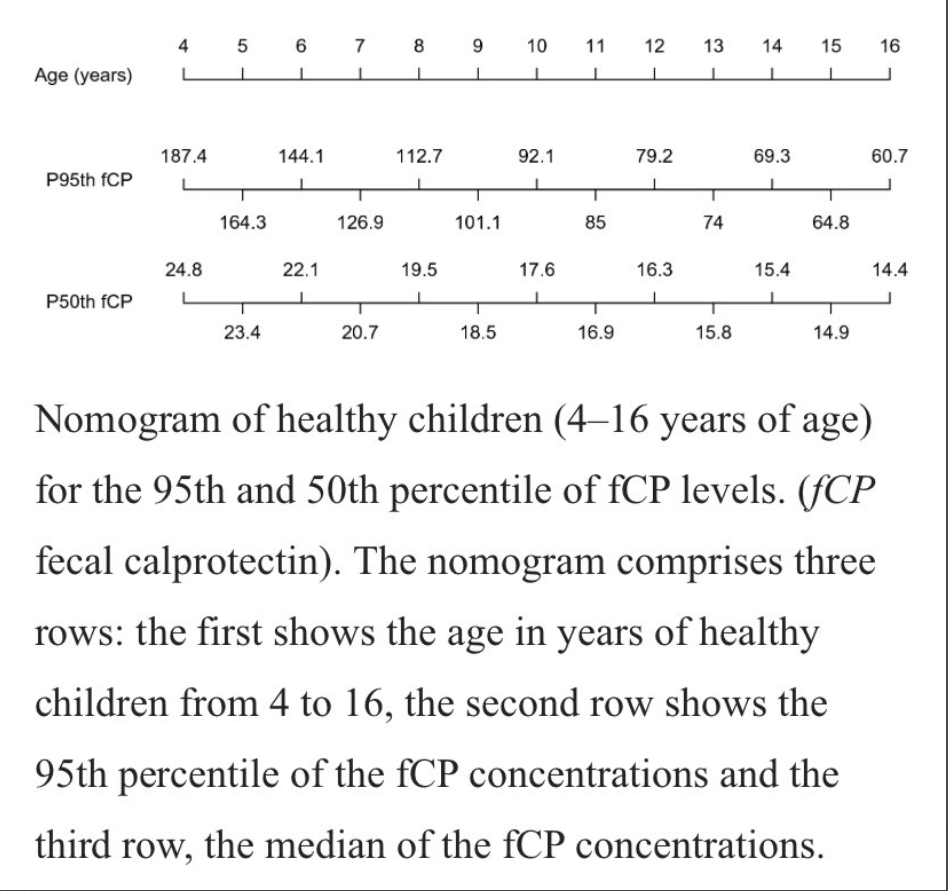
This study collected prospective data from 212 children. Key finding: The median and 95th percentile for fCP were 18.8 mg/kg and 104.5 mg/kg, respectively. “We found a statistically significant association between the 95th percentile of fCP concentrations and age (p < 0.001).”
My take: This is another study showing that calprotectin cut off values need to be higher in younger children.
The study and associated editorial highlight the effectiveness of GLP-2 in a prospective cohort of 17 patients with short bowel syndrome. It is noted that Dr. Hill has received funding from the pharmaceutical manufacturer of the product.
Key findings:
A total of 12 of 17 patients achieved parenteral independence: 3 patients after 3 months of treatment, 4 patients at 6 months, and 5 after 12 months.
The percentage able to wean off parenteral nutrition was 17%, 44%, and 60% at 3, 6, and 12 months respectively. Only 1 patient did not exhibit improvement
Plasma citrulline levels, a marker for enteral autonomy, increased from a baseline average of 20 micromol/l to 37.5, 46.75, and37.9at 3, 6, and 12 months respectively.
Adverse reactions included abdominal pain 30%, nauseas 18%, injection-site reactions 22%, and headache 16%.
Both the editorial and the study comment briefly on the cost of the therapy. The editorial also notes the current recommendation for surveillance endoscopy in view of a hypothetical risk of malignancy.
My take: Is GLP2 Worth the Cost? It probably depends on who is paying and long-term safety data. Perhaps, we will develop tools to improve prediction of which patients will achieve enteral autonomy with GLP2 who would otherwise require ongoing parenteral nutrition.
Methods: A state-transition model of chronic HCV was developed to conduct a cost-effectiveness analysis comparing treatment at age 6 years vs delaying treatment until age 18 years
Key findings:
After 20 years, treating 10 000 children early would prevent 330 cases of cirrhosis, 18 cases of hepatocellular carcinoma, and 48 liver-related deaths
The incremental cost-effectiveness ratio of early treatment compared to delayed treatment was approximately $12 690/quality-adjusted life-years gained and considered cost-effective
My take (=conclusion from authors): Delaying treatment until age 18 years results in an increased lifetime risk of late-stage liver complications. Early treatment in children is cost effective. Our work supports clinical and health policies that broaden HCV treatment access to young children.
Related blog posts:
Hepatitis C in 2020: NASPGHAN Position Paper -includes the following: “We recommend treatment be considered and offered to all children with chronic HCV as early as 3 years of age with currently approved and anticipated DAA combination therapies”
The authors compared deaths from 2014-2020 using data from the National Center for Health Statistics and US Census Bureau.
Key findings:
Between March 1 and August 1, 2020, 1 336 561 deaths occurred in the US, a 20% increase over expected deaths (1 111 031 [95% CI, 1 110 364 to 1 111 697]).
Of the 225 530 excess deaths, 150 541 (67%) were attributed to COVID-19
The authors conclude that the excess deaths attributed to causes other than COVID-19 could reflect deaths from unrecognized or undocumented infection with severe acute respiratory syndrome coronavirus 2 or deaths among uninfected patients resulting from disruptions produced by the pandemic
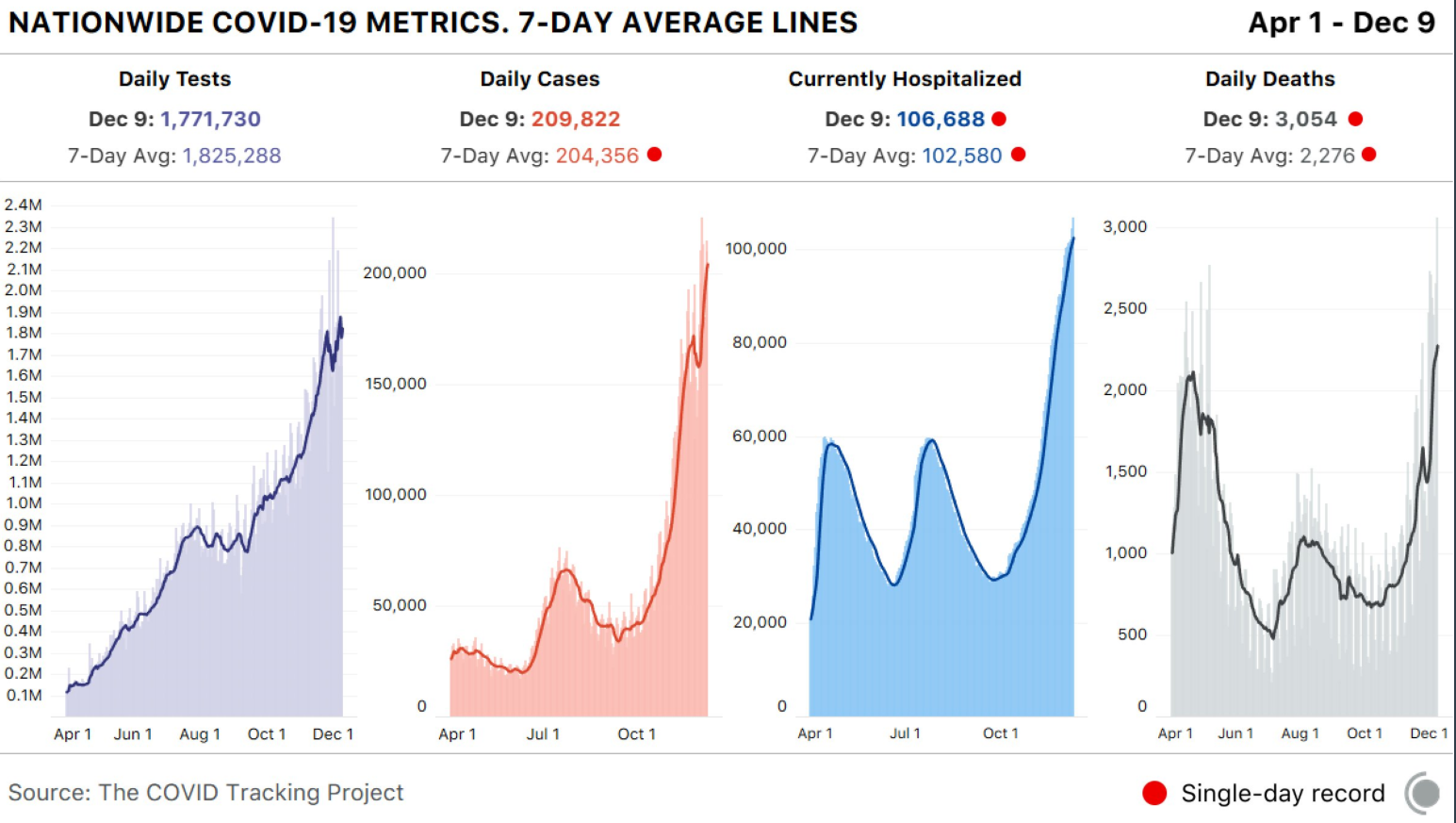
My take: The COVID-19 situation has worsened considerably in the past 2 months and the final toll from this infection will be truly staggering; this unfortunately will include its indirect effects due to deferral of care
When the 10th Circuit Court, with judges Gorsuch, Ebel, and Bacharah, rolled back high-powered magnet regulations in 2016, it was expected that this would result in more suffering in children. The referenced article by Reeves et al documents the effects of this decision.
Background: In 2016, the Zen Magnets decision resulted in magnets returning to the market with warning labels “but not performance standards favored by NASPGHAN (ie, making magnets either too large to swallow or too weak to cause harm).” In this study, the authors used data from the National Electronic Injury Surveillance System (NEISS), a database of consumer product injuries.
Key findings:
When stratified by time period, suspected magnet ingestion (SMI)per year was 1598 during off-market period (when product was banned) compared with 2826 during on-market period.
An estimated 23,756 children (59% males, 42% < 5 years old) presented with a SMI from 2009 to 2019.
There was an average annual case increase of 6.1% (P = 0.01).
After 2017, there was a 5-fold increase in the escalation of care for multiple magnet ingestions (estimated n = 1094; CI 505–1686). “Escalation of care” refers to cases designated as ‘treated and transferred,’ ‘treated and admitted/hospitalized,’ or ‘held for observation.’
My take: Regulatory action is needed to prevent harm in children from these high-powered magnets.There are two companion bills in Congress which are in committee, one entitled “Magnet Injury Prevention Act.” These are clearly needed given previous judicial branch ruling.
Using UK Biobank data with 120 075 participants with 271 who had severe COVID-19, key findings:
Relative to non-essential workers, healthcare workers (RR 7.43, 95% CI 5.52 to 10.00), social and education workers (RR 1.84, 95% CI 1.21 to 2.82) and other essential workers (RR 1.60, 95% CI 1.05 to 2.45) had a higher risk of severe COVID-19.
More specifically, healthcare professionals (doctors, psychologists, pharmacists) (RR 6.19, 95% CI 3.68 to 10.43). The higher risk of severe COVID-19 among healthcare workers was not reduced after adjustment for socioeconomic, work-related, or health and lifestyle-related factors
Using more detailed groupings, medical support staff (RR 8.70, 95% CI 4.87 to 15.55), social care (RR 2.46, 95% CI 1.47 to 4.14) and transport workers (RR 2.20, 95% CI 1.21 to 4.00) had the highest risk within the broader groups.
Compared with white non-essential workers, non-white non-essential workers had a higher risk (RR 3.27, 95% CI 1.90 to 5.62) and non-white essential workers had the highest risk (RR 8.34, 95% CI 5.17 to 13.47).
My take: This study shows the increased risk of severe COVID-19 among essential workers, particularly in healthcare field and non-white ethnicity was associated with further increased risk.
This article describes the worsening situation with global wildfires and their direct/indirect effects on human health. In addition, “the interplay between wildfires and climate change is likely to form a reinforcing feedback loop, making wildfires and their health consequences increasingly severe.” The authors conclude that “societal action is requisite… to limit the global temperature increase” and reduce the severity of wildfires and other effects of climate change.
Specific health risks:
Direct health effects include burns, injuries, mental health effects, and death due to exposure to flames or radiant heat
There is consistent evidence of an increased risk of respiratory events, including hospitalizations and emergency department visits due to asthma, chronic obstructive pulmonary disease, and respiratory infection.
Heavy smoke can cause eye irritation and corneal abrasions and can substantially reduce visibility, increasing the risk of traffic accidents.
Owing to traumatic experiences, property loss, and displacement, residents in areas affected by wildfires are at an increased risk for mental illness, including post-traumatic stress disorder, depression, and insomnia. The psychological consequences of wildfire events can persist for years, and children and adolescents are particularly vulnerable.
Risks of low birth weight and preterm birth are increased
“The fires sweeping across millions of acres in California aren’t just incinerating trees and houses. They’re also filling the lungs of California’s children with smoke, with potentially grave effects over the course of their lives.” This article goes on to detail the personal effects of wildfires on 5 families.