I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Key finding: This case report documents two cases of medically-treated necrotizing enterocolitis (NEC) that developed shortly after Onasemnogen Abeparvovec which was administered at ~3 weeks of life in two full term infants (born at 40 and 41 weeks).
My take: Consider the diagnosis of NEC in full term infants with SMA who have received gene therapy.
Views from Bike Trail near Ospedaletti, ItalyWhile grabbing a snack & taking a break from our bike ride, we saw all of these wind surfers. The wind on this day was crazy and these surfers looked like they were going 30-40 mph
In this retrospective review, among 1671 colonoscopies (2014-2020), 13% (n=219) were in children less than 6 year of age (Median 3.9 yrs). Key findings:
Most common indications in preschoolers were rectal bleeding 35% (n = 78), inflammatory bowel disease 24% (n = 53), diarrhea 13% (n = 30), iron-deficiency anemia 11% (n = 25), and abdominal pain 7% (n = 16).
Ileal intubation rate (IIR) and cecal intubation rate (CIR) were lower in preschoolers (2 to <6 yrs) compared to older children, 81% vs 92% (P = 0.0001), and 93% vs 96.4% (P = 0.02), respectively, and even lower in those aged <2 years, 48.1% IIR (P = 0.0001) and 85.1% CIR.
Diagnostic yield was highest for rectal bleeding at 41% (32/78) including juvenile polyps in 27. The diagnostic yield was 37% for those with diarrhea (12/30) and 36% (9/25) for those with iron deficiency anemia. Overall, diagnostic yield was 40% (87/219)
10 patients (5% of total and 11.5% of those with abnormalities) had findings limited to right colon and/or ileum; thus, incomplete evaluation would have missed these findings.
The authors suggest modifying the PEnQuIN goal of IIR >/= 85% in young children. However, this is unnecessary as most endoscopists are not separating their cases by age.
My take: This study shows that colonoscopy is often more difficult to complete in younger children. Achieving high IIR improves the yield of colonoscopy. Overall, the findings in this report mirror our experience in which colonoscopy had a diagnostic yield of 42% (in non-folllowup colonoscopies) and findings isolated to ileum were noted in 6% (and additional 4% with grossly normal/abnormal histology).
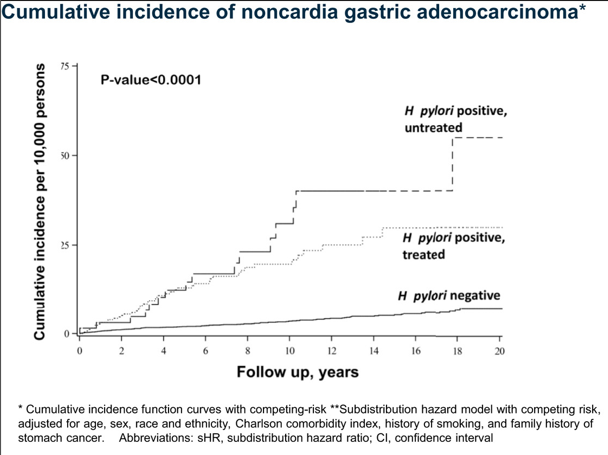
The authors examined a retrospective cohort study of Kaiser Permanente Northern California members (716,567 individuals) who underwent testing and/or treatment for H pylori between 1997 and 2015 and were followed through December 31, 2018. Key findings:
The adjusted subdistribution hazard ratios of NCGA for H pylori–positive/untreated and H pylori–positive/treated individuals were 6.07 and 2.68, respectively, compared with H pylori–negative individuals.
When compared directly with H pylori–positive/untreated individuals, subdistribution hazard ratios for NCGA in H pylori–positive/treated were 0.95 at <8 years and 0.37 ≥8 years of follow-up.
My take (borrowed from authors): H pylori eradication therapy was associated with a significantly reduced incidence of gastric cancer after 8 years compared with no treatment. The risk among treated individuals became lower than the general population after 7 to 10 years of follow-up. The findings support the potential for substantial gastric cancer prevention in the United States through H pylori eradication.
This article is a good review detailing the management of restrictive eating disorders, including anorexia nervosa, atypical anorexia nervosa (weight in normal range despite significant loss) and avoidant/restrictive food intake disorder. The tables provide diagnostic criteria, medical complications, and clinical factors supporting admission.
The authors also delve into the topic of refeeding syndrome. Key points:
“Contrary to prior belief, HCR [high calorie restriction] does not carry a significant risk of RS [refeeding syndrome] when close electrolyte surveillance and supplementations are implemented. Furthermore, LCR is associated with poor inpatient weight gain…and longer hospital admissions.”
“The evidence in our progress report supports an HCR strategy of initiating inpatient refeeding at 2000-2400 kcal/day…and increasing by 200 kcal/day in patients with an admission BMI of >60% mBMI.”
The authors recommend daily electrolyte assessment for first 7 days, followed by every other day for duration of admission.
Daily caloric requirements “often exceed 3000 kcal/day in the initial weeks of refeeding”
My take: While the authors focus on restrictive eating disorders, their approach to refeeding implies consideration in other disorders associated with moderate malnutrition.
A dog walks into the bar, jumps up on the stool and says to the bartender, “Hey barkeep, it’s my birthday today. How ’bout a free drink?” The bartender turns, looks at the dog and nods his head, “Sure pal, toilet’s right down the hall.”
And
A dog walks into a bar. Bartender nods and says, “Hey dog, haven’t seen you in a while, how are things going?” Dog looks at him sadly and replies, “Ruff.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
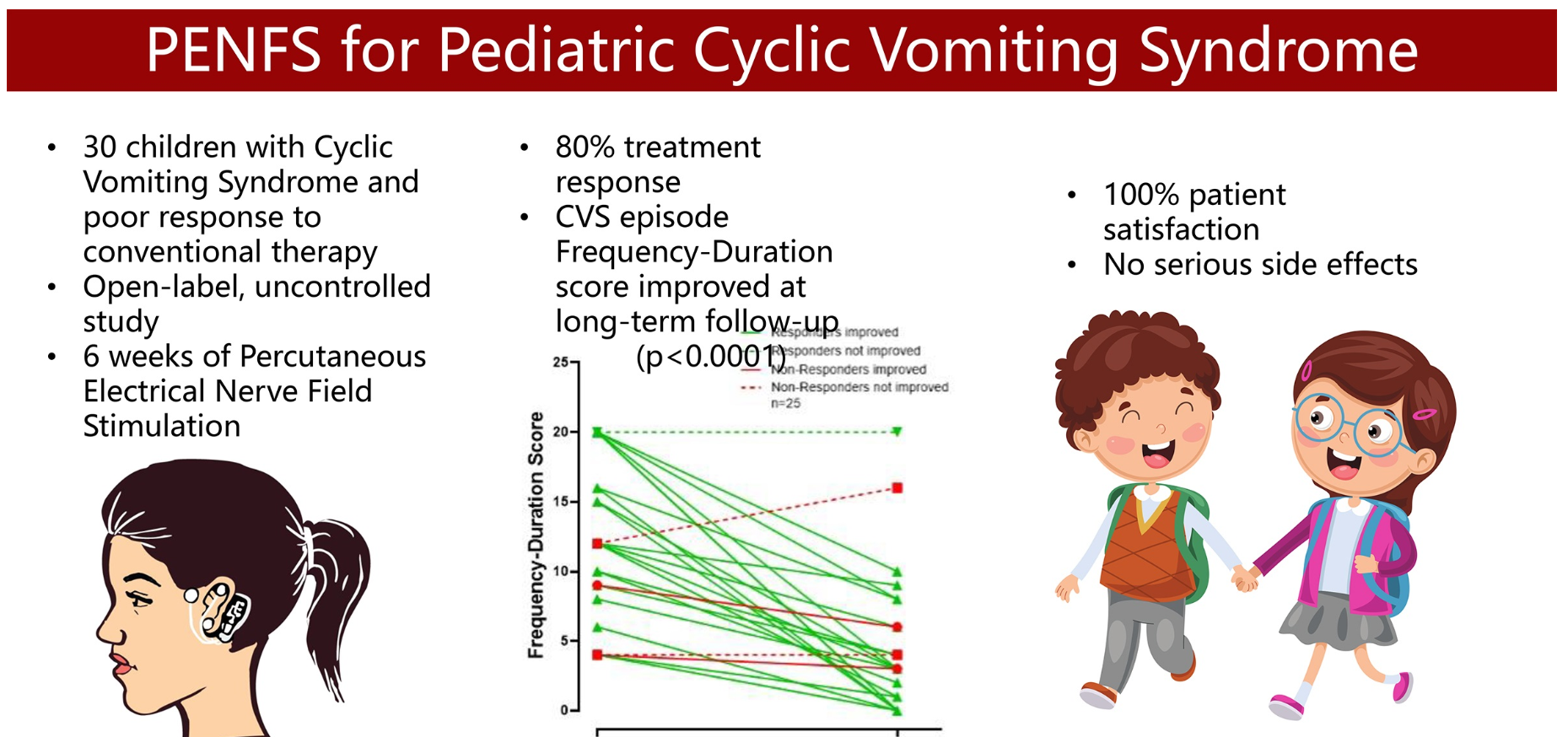
K Karrento et al. JPGN 2023; 77: 347-353. Percutaneous Electrical Nerve Field Stimulation for Drug-Refractory Pediatric Cyclic Vomiting Syndrome
In this prospective study with 30 children with drug-refractory CVS, response was classified as ≥50% improvement in either frequency or duration of attacks at extended follow-up.
Key findings:
At follow-up, 80% met criteria for treatment response with a median (IQR) response duration of 113 (61–182) days.
At end of therapy, 66% and 55% patients reported global response of at least “moderately better” and “a good deal better,” respectively.
There were no serious side effects.
Limitations: episodic nature of CVS, no control group, hx/o strong placebo control group and lack of validated assessment tool
My take: 1. As with the drug therapies with CVS, it is difficult to know how effective PENFS is for CVS. At the same time, its good safety profile makes this therapy an intriguing option in those not responding to more typical treatments. 2. The visual abstract is funny -mainly due to the two laughing kids holding hands. Though it would be even better if the person on the left was puking a lot instead of having a PENFS device.
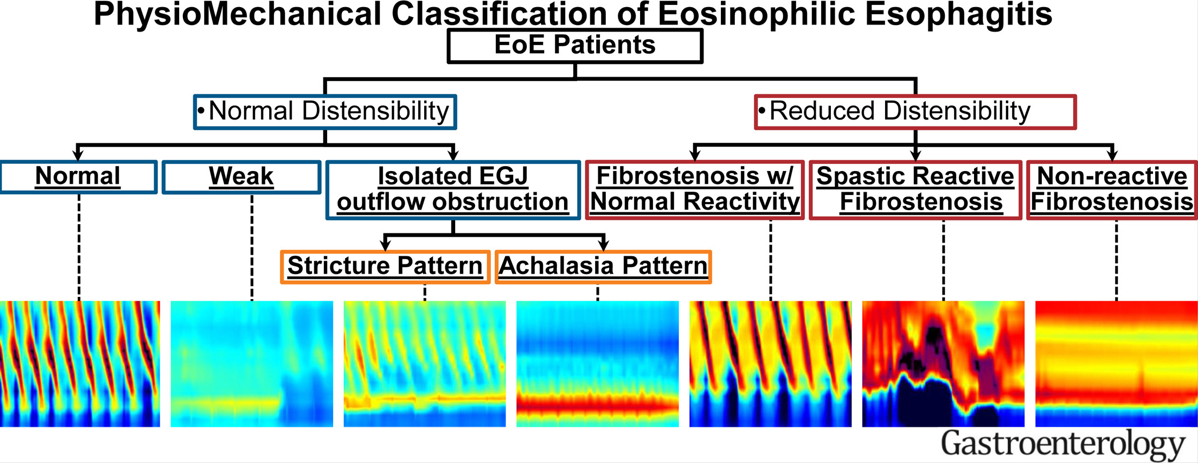
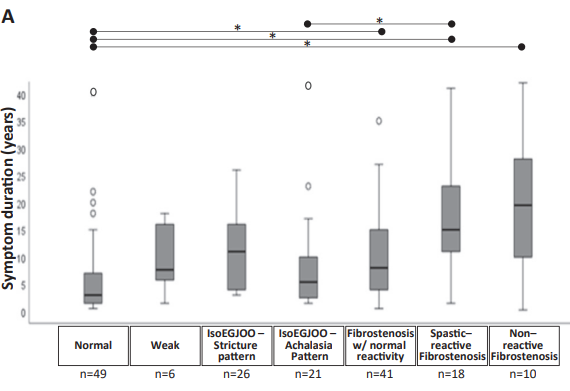
215 adults with EoE who completed FLIP during endoscopy were included in a cross-sectional study. FLIP helped separate the physiomechanical properties of esophageal function in this cohort. The criteria used to define the PhysioMechanical classification in EoE with a representative FLIP panometry image for each classification. Normal compliance was defined as a DP >17 mm and body compliance >450 mm3/mm Hg; reduced compliance (fibrostenosis) was defined by DP ≤17 mm or compliance ≤450 mm3/mm Hg. Normal EGJ opening was defined as a maximum EGJ diameter ≥16 mm; reduced as maximum EGJ diameter <16 mm. ∗Spastic-reactive contractile response (SRCR) with normal body distensibility and normal EGJ opening was assigned as “achalasia pattern” (n = 1 in this cohort).
Key findings:
FLIP was normal in 50 (23%), weak pattern in 7 (3%), IsoEGJOO stricture pattern in 27 (13%), IsoEGJOO achalasia pattern in 26 (12%), Fibrostenosis with normal reactivity in 61 (28%), spastic reactive fibrostenosis with normal reactivity in 30 (14%), and noreactive fibrostenosis in 14 (7%)
My take: FLIP testing helps define the mechanism of esophageal dysfunction in patients with EoE. Longer duration of symptoms was associated with more severe esophageal dysfunction.
In this study, the authors analyzed laboratory testing results from pediatric patients newly diagnosed with celiac disease (2018-2021) to determine the usefulness of each test derived from recommended guidelines (J Snyder et al. Pediatrics 2016; 138: e20153147). Screening protocols in their center resulted in an estimated cost of approximately $320,000 during the study. Tests at diagnosis included hemoglobin, alanine/aspartate aminotransferase, ferritin, iron, TSH, Free T4, and vitamin D screening. These screening tests were done in ~80% of 468 patients.
Key findings:
Ferritin was abnormal in 29%, hemoglobin was abnormal in 12%, and iron was abnormal in 22%. Abnormal ferritin captured all patients in this cohort with an abnormal iron. If ferritin was used as an isolated screen with reflective iron testing, this would have reduced costs by about $12,000
AST and ALT were abnormal in 2% and 11% respectively
25-OH Vitamin D was abnormal in 14%. Recent data indicated that low Vit D levels are similar among patients with and without celiac disease (R Ahlawat et al. JPGN 2019; 69: 449-454)
TSH and Free T4 were abnormal in 7% and 0.3% respectively. For thyroid disease, TSH and free T4 testing did not lead to any new diagnosis of thyroid disease (7 carried a preexisting diagnosis). There were 19 additional patients with abnormal lab values who had more testing due to initial abnormalities. If TSH alone were used for screening, costs savings would be about $29,000. If no thyroid testing were done, this would have reduced costs by about $40,000.
Hepatitis B immunity was NOT present in 69%. However, recent studies have shown similar levels of immunity in those with and without celiac disease. In addition, it is not clear that a low level hepatitis B surface antibody always indicates a lack of immunity. Eliminating hepatitis B screening would have reduced costs by about $63,000.
The authors note that the cost savings by adopting their recommendations would have saved about $104,000 (out of $320,000).
My take: This is a very useful study and indicates that curtailing initial testing for celiac disease could reduce costs substantially and without compromising care. This would include notchecking a serum iron, a free T4, or hepatitis B studies. The authors note that the value of Vit D testing is also questionable but may be worthwhile due to increased risk of bone disease in individuals with celiac disease.
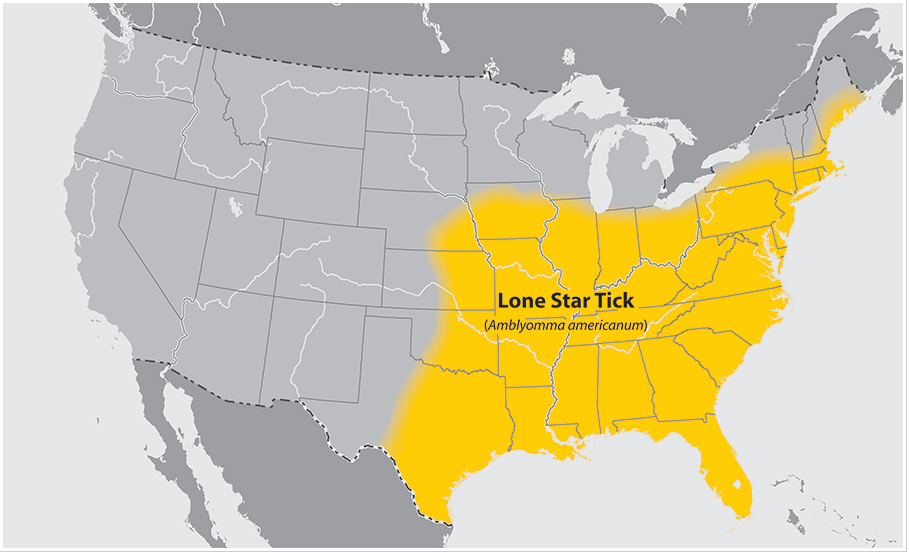
Background: A CDC report showed that between 2010 and 2022, more than 110,000 suspected cases of alpha-gal syndrome were identified. The majority of cases are linked to bites from the lone star tick which affects much of the U.S. (map below) as well as Central and South America, Asia, Africa, Australia and parts of Europe.
Findings: This study reports 3 pediatric patients who presented with only nonanaphylactic symptoms of alpha-gal syndrome. These patients with recurrent gastrointestinal distress and emesis after consuming mammalian meat, even in the absence of an anaphylactic reaction.
The diagnosis in these three patients was established by history, serum alpha-gal immunoglobulin E elevation and response to avoidance of red meat.
My take: Checking a serum Alpha-gal IgE seems like a good idea in some children with unexplained abdominal pain with episodic exacerbation with vomiting, especially if tick exposure. Anecdotally, I have checked this a few times and so far I have not I identified a case. Most cases of Alpha-gal will be associated with urticaria.
CDC:Alpha-gal syndrome “Symptoms commonly appear 2-6 hours after eating meat or dairy products, or after exposure to products containing alpha-gal (for example, gelatin-coated medications).”
CDC: Food products that may contain alpha-gal: Mammalian meat (such as beef, pork, lamb, venison, rabbit, etc.) can contain high amounts of alpha-gal. Food products that contain milk and milk products typically contain alpha-gal (though many patients tolerate dairy products)
Foods that do NOT contain alpha-gal (unless cross contamination):
Case history: A well-nourished previously healthy 20 month old was admitted to the hospital with a one week history of frequent vomiting. He had a history of frequent lint ingestion. He had been seen by three different health care providers during the week prior to his admission.
At the time of admission, he had numerous electrolyte derangements (Na 124, K 3.2, CL 76) and acute kidney dysfunction with a BUN of 118 and Creatinine of 3.06. He had severe multisystem disease including severe ventricular dysfunction (BNP 2196). He needed an oscillator ventilator, dialysis and cardiac medications (including epinephrine, and milrinone).
He had an extensive evaluation. After he had stabilized and then markedly improved (12 days after admission), an UGI study demonstrated an obstruction near the 2nd-3rd portion of the duodenum with a dilated proximal duodenum.
UGI study:
Due to the obstruction which was thought to be anatomic, the GI service deferred management to pediatric surgery. The surgical service requested GI inspection with endoscopy immediately prior to surgery. If a bezoar was identified, the surgical plan was for a mini-laparotomy. If not, the surgical plan was for laparoscopy repair.
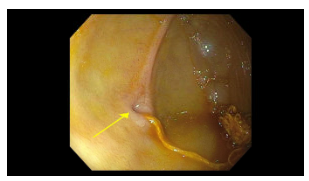
Endoscopy findings: There was a narrowed opening (different orientation of same narrowing in both pictures) with a string-like material.
Surgical findings: A duodenal web with a piece of lint was identified. The patient had a laparoscopic wedge excision with a transverse closure of the duodenotomy. The lint may have occluded the tiny opening of the web that he had been living with since he was born.
My take: This is the first time I have seen the endoscopic appearance of a duodenal web.
In my view, this was a ‘great case.’ In a commentary by Jerome Groopman (N Engl J Med 2004; 351:2043-2045), his wife noted that a case is “a great case because you not only make the diagnosis — you do something fundamental about it. You can really help.” However, Dr. Groopman stopped using the words, ‘a great case’ after his personal experience when his son was severely ill as an infant with a bowel obstruction due to intussusception: “For me and for Pam, the experience had no resonance of “a great case.” There was no intellectual pleasure in solving a clinical puzzle, no charge of exhilaration from the drama of the operation. Instead, there was terror, raw and palpable, as we realized how close we had come to burying our first son….I still find myself unable, except in retrospect, to retrieve the language of my youth and speak about “a great case.” It is as if medicine at this stage of my life has split into two streams — a current of marvelous biology and an undertow that pulls at the soul.”