This study included 9 RCTs involving a total of 445 participants. Key findings:
Though some of the study findings seemed to favor prebiotics, all evidence was of very low certainty.
“There may be no difference in occurrence of clinical relapse when adjuvant treatment with prebiotics is compared with adjuvant treatment with placebo for maintenance of remission in UC.”
“Adjuvant treatment with prebiotics may result in more total adverse events when compared to adjuvant treatment with placebo for maintenance of remission. The evidence was of low certainty.”
My take: Currently, there is no solid evidence to recommend prebiotics in patients with ulcerative colitis.
In this Swedish study with 294 randomized participants who had with moderate to severe I.B.S, 96 assigned to the LFTD (low FODMAPs with IBS advice) diet, 97 to the low-carbohydrate diet, and 101 to optimised medical treatment. Response was defined as a reduction of 50 or more in IBS-SSS compared with baseline.
Key findings:
Response rate after 4 weeks: 73 (76%) of 96 participants in the LFTD diet group, 69 (71%) of 97 participants in the low-carbohydrate diet group, and 59 (58%) of 101 participants in the optimised medical treatment group
An excerpt: “A new study suggests that certain dietary changes may be more effective than medication..When she checked on the participants during the trial, one from the low-FODMAP group cried when she described how much better she felt on the diet. Another in the low-carbohydrate group said she “never in her life had felt so good in her stomach,” Dr. Nybacka said…
Dr. Chey said the study was well done and provided “real data” to support what many doctors have observed: That “diet therapy is at least as good and probably better” than medication.
My take: Dietary therapies and psychological therapies are underutilized in the management of IBS. For those using dietary therapies, counseling with a nutritionist is a good idea.
“GLP-1 RAs (eg, semaglutide, tirzepatide, exenatide, liraglutide, albiglutide, dulaglutide, and lixisneatide) mimic incretins, which are hormones released after eating that prompt glucose-dependent insulin release from the pancreatic islets, stimulate satiety centers, inhibit glucagon release, and result in diminished gastric emptying.”
Because GLP-1 RAs diminish gastric emptying, they can increase the risk of residual gastric contents prior to surgery and endoscopy.
AGA Recommendations:
“If patients taking GLP-1 RAs solely for weight loss can be identified beforehand, a dose of the medication could be withheld before endoscopy with likely little harm, although this should not be considered mandatory or evidence-based. Nevertheless, it is unclear if withholding the medication for only one dose would be reliably adequate for an individual’s gastric motility to return to normal. ..there is insufficient evidence to suggest this practice be performed for patients taking these medications to treat diabetes”
“Generally, in patients on GLP-1 RAs who have followed standard perioperative procedures (typically an 8-hour solid-food fast and a 2-hour liquid fast) and who do not have symptoms of nausea, vomiting, dyspepsia, or abdominal distention, we advise proceeding with upper and/or lower endoscopy.”
“When possible, placing patients on a liquid diet the day before sedated procedures may be a more acceptable strategy, in lieu of stopping GLP-1 RAs.”
My take: This guidance provides useful advice given the increasing use of GLP-1 RAs. If these medications are being used for obesity, holding a dose prior to endoscopy is a good idea.
Related article: S Sen et al. JAMA Surgery 2024; doi:10.1001/jamasurg.2024.0111.Glucagon-Like Peptide-1 Receptor Agonist Use and Residual Gastric Content Before AnesthesiaKey finding: Use of a GLP-1 RA was independently associated with increased residual gastric content (1.5 mL/kg of clear liquids on gastric ultrasonography) on preprocedural gastric ultrasonography: 56% (35 of 62) in patients with GLP-1 RA use (exposure group) compared with 19% (12 of 62) in patients who were not taking a GLP-1 RA drug (control group).
This is at the entrance to the Westside Reservoir Park. I had the chance to go there as part of a Westside Beltline Tour in Atlanta.This reservoir is as deep as the Statue of Liberty is tall and can hold 2.4 billion gallons of water for the city of Atlanta
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
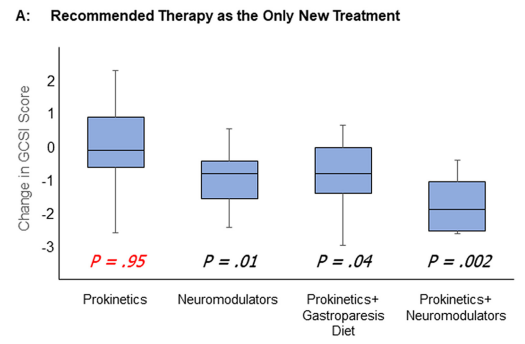
Methods: In this prospective study of patients (n=129) with suspected gastroparesis, the authors examined longitudinal outcomes focusing on responses to prokinetics and other therapies. This included gastroparesis diets and neuromodulators. Patients underwent validated gastric emptying testing (wireless motility capsule and gastric emptying scan) before recommending new treatments.
Prokinetics included dopamine antagonists, motilin agonists, acetylcholinesterase inhibitors, and pyloric botulinum toxin injection.
Key findings:
“Initiating prokinetics as solo new therapy had little benefit for patients with symptoms of gastroparesis.”
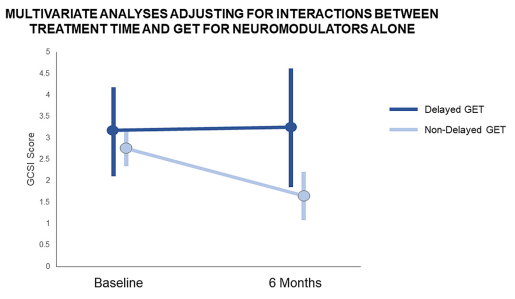
“Neuromodulators as the only new therapy decreased symptoms other than nausea and vomiting”
Combination therapy of a prokinetic with a neuromodulator appeared to be the most effective
Neuromodulators were mainly effective in those without delayed gastric emptying times
My take: Our therapies for gastroparesis are not very good. And, neuromodulators are likely to be more helpful than prokinetics.
Like yesterday’s article on GTs, this is another terrific review with plenty of helpful images and advice regarding ostomy management.
Background: “There are upwards of 1 million people living with ostomies (ostomates) in the United States.” “Approximately 75% of all ostomies in the pediatric population are created in the neonatal or infant patient.”
Table 1 lists the purposes and types of ostomies including gastrostomy, jejunostomy, ileostomy, appendicostomy (Malone), cecostomy, colostomy and urinary diversions (eg. Mitrofanoff).
Surgical considerations are reviewed including optimizing nutrition preoperatively and minimizing corticosteroids. Biologics: “The most recent evidence does not support a delay in gastrointestinal surgery for children with IBD receiving biological therapy…[and] typically, biological therapy can be resumed 14 to 28 days after the operation.” For oral small molecules (with short half-lives), these may be restarted sooner if indicated.
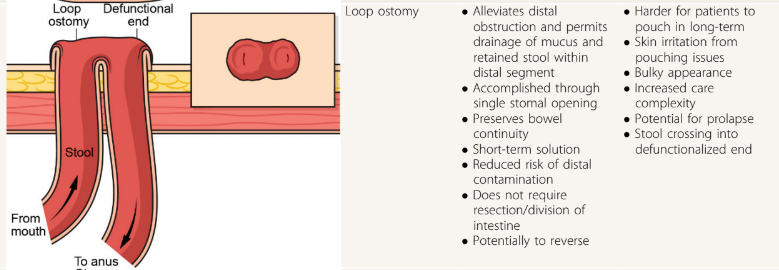
Table 2 provides pictures of the lower ostomies. For example:
Postoperative care is discussed including healing times, need for wound ostomy nurse input, and addressing self-image. Patients with motility disorders are “more likely to experience postoperative complications”
Table 4 details the products for pouch care including pouching systems, skin barriers, pouch liner, gas vent, pouch lubricant, pouch covers, and adhesive remover.
Table 5 summarized ostomy-related complications and treatments. Complications include stomal necrosis, stomal bleeding, stomal retraction, mucocutaneous separation, parastomal hernia, stoma prolapse (can apply cool compresses, apply osmotic agent (sugar) or manually reduce), stoma stenosis, and dermatitis.
Table 6 addresses medical management issues like odor, blockage, diarrhea, and constipation. This table also provides recipes for antegrade enemas (see below) and links including a very useful bowel management guide for families (28 pg from Boston Children’s) and enema ingredients and supplies (2 pg from Seattle Children’s); the latter has some overlapping information with the former.
At the conclusion of the article, there is further discussion of systemic and ostomy-related complications (much of which is summarized in Table 5). The article references the Ostomy Skin Tool as a metric to follow the clinical state of the ostomy. The United Ostomy Associations of America (ostomy.org) is listed as a good resource (which it is!).
My take: This is a very useful resource. Even a quick read will make clinicians appreciative of having the assistance wound ostomy nurses.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Thanks to Patrick Reeves for sharing this reference. While reading this article, I was reminded of Debbie Mason RN. She worked mainly for Colin Rudolph when I was a fellow at Cincinnati. She would teach the fellows the ‘ins and outs’ regarding gastrostomy tubes (GTs).
Some of the points from this article:
Background: In one large study, 25% of hospitalized pediatric patients in 63 U.S. hospitals required a temporary NG tube. GTs “preferred for longer-term access due to being less prone to accidental dislodgement, blockage, and interruption of feeds. They are also more durable, discrete, and avoid nasal trauma.” They are probably safer too for longer-term use. (An omission in the article: AMT bridles can help maintain NGs.)
Indications: Reviews the extensive list of reasons for GT placement, most related to inadequate nutritional intake (related to many chronic disease processes)
Contraindications are reviewed. “Absolute contraindications include active sepsis or peritonitis, massive ascites, uncorrectable coagulopathy, portal hypertension with significant varices, and history of total gastrectomy.” Transoral PEG tube is contraindicated, as well, if pharyngeal or esophageal obstruction, malrotation, or colonic interposition.
Preprocedural evaluation is described. Some have recommended UGI prior to placement in those with congenital anomalies. Others have stated that “even congenital anomalies should not mandate an upper GI series given how rare malrotation is in general.” Many children benefit from NG feeding trials prior to GT placement which can also improve nutritional status preoperatively.
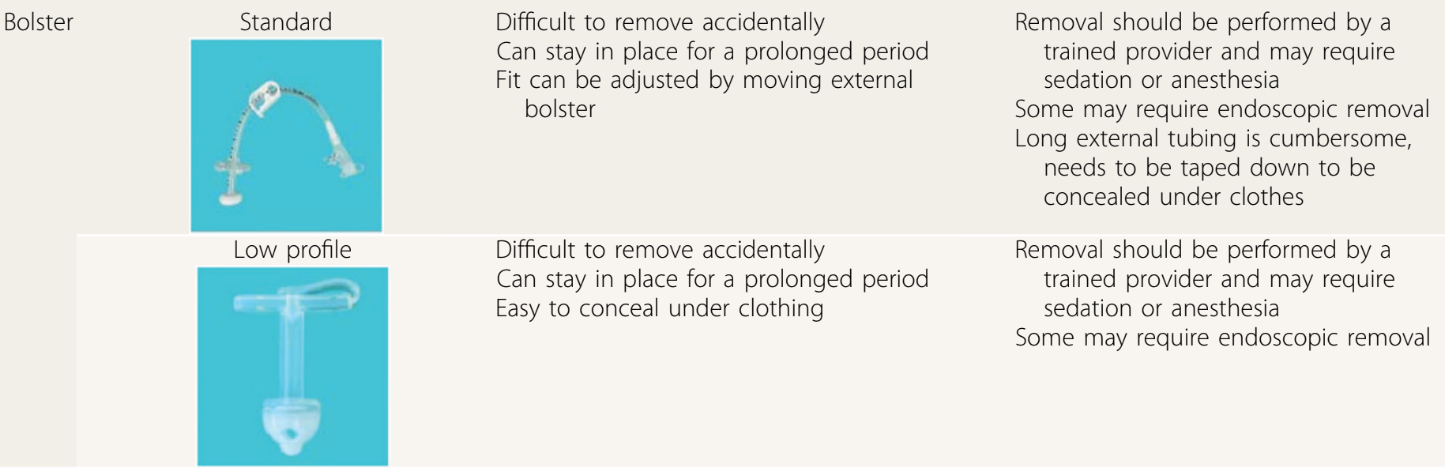
The placement methods and types of GTs are reviewed. “As of now, there is no clearly identified optimal technique” (eg. laparoscopic GT vs PEG). The others note a meta-analysis of 22 studies (n >5000) found a higher rate of major complications with PEG placement. The authors recommend T-fasteners if GT balloon is used for initial placement.
Examples of bolster-type (non-balloon) GTs:
GT complications are discussed including infection, peritonitis, bleeding (rare to need a transfusion), injury to adjacent organs, pneumoperitoneum (usually benign and transient), hypergranulation, cellulitis (often treated with a first-generation cephalosporin or topical mupirocin), dislodgement, tube migration, and buried bumper syndrome. For early dislodgement (especially first 4-6 weeks after placement), blind reinsertion should be avoided.
GT care: The authors recommend starting feeds “not more than 3 to 6 hours” after placement to monitor for immediate postoperative complications, and cleaning site with warm water, saline or soap. Once the site has healed showering and bathing can resume; swimming can be permitted a few weeks after placement. Medications should be given via gastric port (if GJ) for better absorption of medications and lessen risk of tube clogging.
Troubleshooting: This is the most useful part of this article. Advice on peristomal leakage: “Placing larger tubes should be avoided because this will only enlarge the stoma tract…removal of the tube for a few hours can be considered because this permits the tract to start closing.” Leakage is often due to issues with balloon volume, poor fit, gastric pressure (eg dysmotility, gastroparesis) and poor wound healing. Clogging: “Carbonated beverages, juices, and meat tenderizer…studies have not shown these to be effective.” Lukewarm water, left to stand 20 minutes, is the first line agent for declogging. Other options include commercial enzymatic decloggers, and mechanical decloggers.
GT removal is discussed and I disagree with the authors that “persistent gastrocutaneous fistulas are rare after removal” (though the majority will close with conservative management). The authors do not recommend cutting GT bolsters due to risk of obstruction and note that endoscopic removal is often necessary.
My take: This article would be well-positioned as part of any GI fellows’ required curriculum and has a bunch of pointers for experienced clinicians as well. It could easily be used for material for ABP questions too. The article is much more detailed than the summary I have provided.
Also, another relevant resource (not discussed in article): Oley Foundation (oley.org). This foundation aims to help those living with home IV nutrition or tube feeding through advocacy, education, community and innovation.
Methods: Retrospective cohort study (n=195) including consecutive CD patients starting treatment with IFX. Rates of transmural remission were compared between patients with and without therapeutic drug monitoring (target level: 5-7 µg/mL).
Key findings:
The rates of transmural remission were higher in patients under proactive therapeutic drug monitoring (37.2% vs 18.3%; P = .004) with similar results in the propensity score–matched analysis (34.2% vs 17.1%; P = .025).
In multivariate analysis, proactive therapeutic drug monitoring was independently associated with transmural remission (odds ratio, 2.95)
My take: Proactive therapeutic monitoring is beneficial in improving outcomes in patients with Crohn’s disease. Higher drug levels are likely to be particularly important to achieve adequate tissue penetration in transmural Crohn’s disease.
Methods: Using Swedish histopathology and register-based data, we identified 27,262 patients with CD diagnosed in 2002–2017 and 132,922 age- and sex-matched general population comparators.
Key Findings:
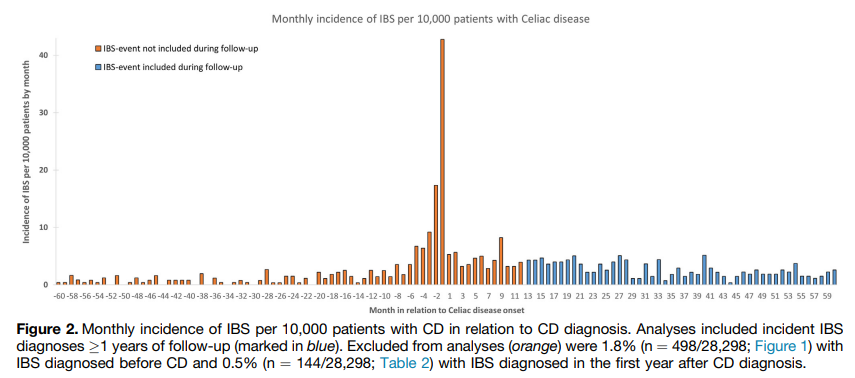
During an average of 11.1 years of follow-up, 732 celiac patients (2.7%) were diagnosed with IBS vs 1131 matched general population comparators (0.9%).
Compared with siblings (n= 32,010), celiac patients (n = 19,211) had >/= 2-fold risk of later IBS (aHR, 2.42)
Compared with celiac patients with mucosal healing, those with persistent villus atrophy on follow-up biopsy were less likely to be diagnosed with IBS (aHR, 0.66)
Interpretation of findings:
“We found celiac patients with persistent villus atrophy on follow-up biopsy less likely to be diagnosed with IBS than those with mucosal healing. Traditionally, physicians have hesitated to diagnose IBS in patients with an organic gastrointestinal disorder (eg, CD), possibly underestimating the observed IBS risk in CD. This reluctance to diagnose IBS may be particularly true for celiac patients who have not achieved mucosal healing, because persistent villus atrophy may indicate that ongoing symptoms are due to gluten exposure instead of IBS.”
“Surveillance bias is another challenge of studies associating IBS with CD. From the outset of diagnosing and managing these conditions, they are often mutually excluded (eg, CD-specific serology tests are often part of the workup of IBS-like symptoms). Consequently, the strength of the association between these conditions may be overestimated.” This is why the authors focused on IBS events beyond the first year of CD diagnosis and there continue to be an increased risk of IBS 10 years of follow-up.
Another limitation of this study: “a large proportion of IBS patients are cared for in primary care or never seek care at all, and hence our study may have had a low sensitivity for IBS, particularly mild IBS.”
My take: While recurrent symptoms in patients with CD could indicate ongoing gluten exposure, recurrent symptoms can also be due to IBS which can occur even with mucosal healing.
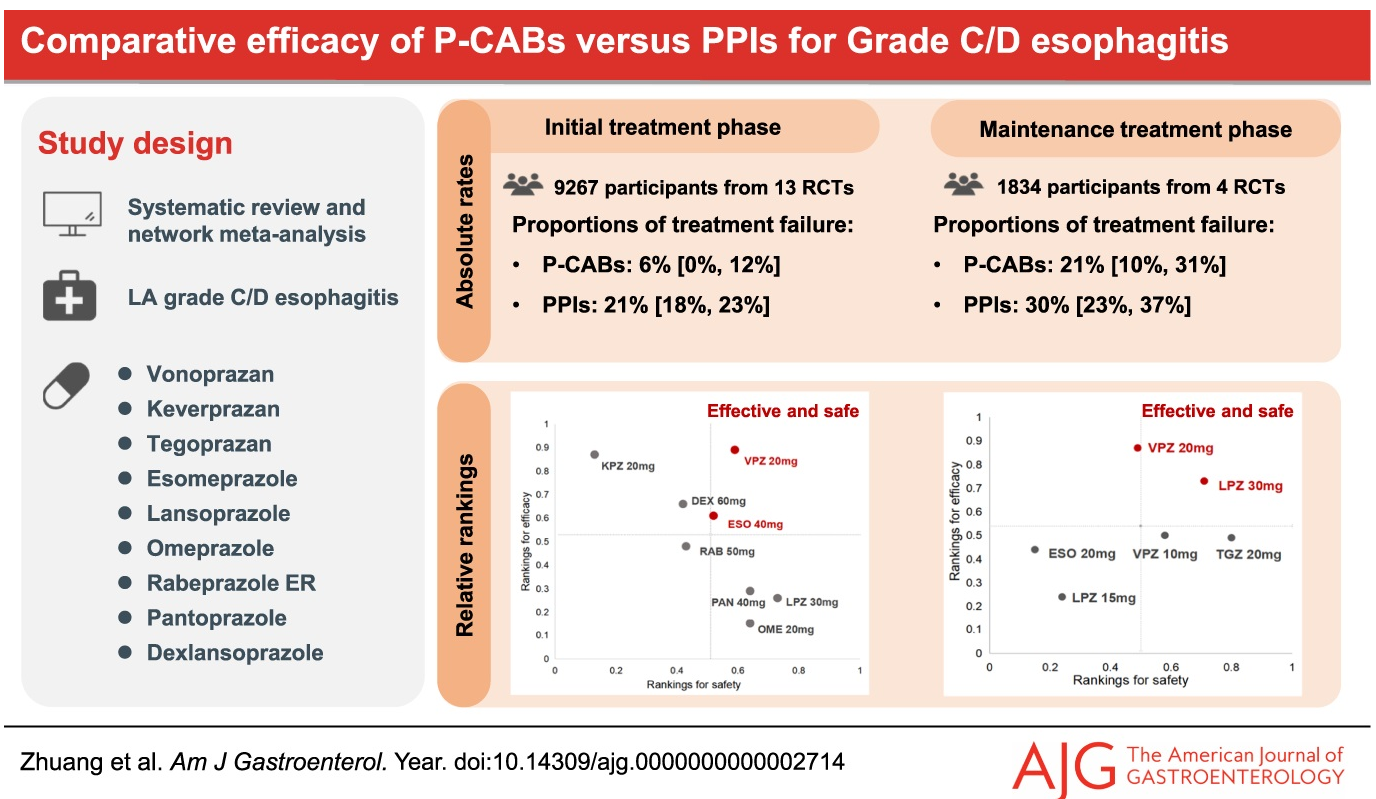
In this meta-analysis, 24 studies met criteria. Key findings:
Vonoprazan (20 mg) had the lowest rates of treatment failure: 6% in the initial treatment phase, and 21% in the maintenance phase of healing of grade C/D esophagitis
Vonoprazan had similar risk of incurring adverse events, severe adverse events, and withdrawal to drug when compared with PPI.
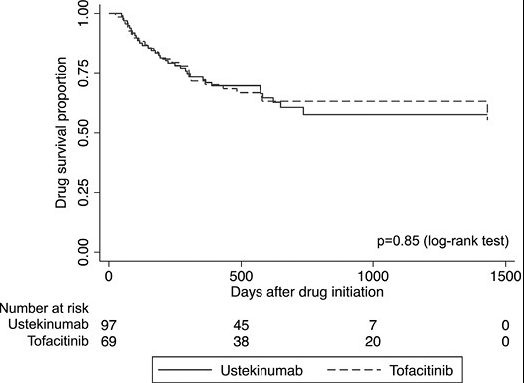
In this real-world cohort of anti-TNF-exposed patients with ulcerative colitis, tofacitinib (n=69) and ustekinumab (n=97) demonstrated similar effectiveness in achieving steroid-free clinical remission (SCFR) at 12 and 52 weeks. The median follow-up was 88.0 and 62.0 week, respectively. 35 of 66 in the tofacitinib cohort had dose reduction from the starting dose of 10 mg twice daily. This reduction occurred at a mean of 144 days. 59 of 97 in the ustekinumab cohort received either Q4W dosing (n=43) or Q6W (n=16).
Key findings:
53% of patients receiving tofacitinib and 32% of patients receiving ustekinumab achieved SFCR at 12 weeks. Tofacitinib-treated patients had higher baseline Mayo endoscopic subscores and CRPs.
At 52 weeks, approximately 50% of patients in both treatment groups achieved SFCR. There were also high proportions (>60%) of patients in both treatment groups who had endoscopic response within 52 weeks.
Both drugs were well-tolerated, as only 1 patient in each treatment group discontinued therapy due to an AE during >260 patient-years of follow-up.
My take: This shows similar response to either tofacitinib and ustekinumab in a cohort that had refractory disease as patients were anti-TNF failures and most had prior vedolizumab as well.