The authors retrospectively utilized the University of Manitoba IBD Epidemiology Database includes all Manitobans diagnosed with IBD between 1984 and 2018 (n=5920). Key findings:
Rates of PPI use in control subjects increased gradually from 1.5% to 6.5% over 15 years
Persons with IBD had a higher rate of PPI use, peaking up to 17% within 1 year of IBD diagnosis with a rate ratio (RR) of 3.1
The authors noted an abrupt increase in PPI use within 6 months of an IBD diagnosis which could indicate that IBD-related symptoms are being mistakenly treated with a PPI or that IBD may increase reflux-related symptoms. Given the higher rate of PPI use in pre-IBD diagnosis patients, compared to controls, the authors note that “it is possible that their [PPI] use enhances the likelihood of an IBD diagnosis by their role in altering the gut microbiota.” In addition, they note that “a case-control study found that PPIs were associated with an increased risk of pediatric IBD” (NR Schwartz et al. J Pediatr Pharmacol Ther 2019; 24: 489-496).
My take: PPIs are being used more frequently. Whether PPIs are detrimental before or after a diagnosis with IBD is not clear.
JCT Lai et al. NEJM 2023; 389: 2377-2385. Case 39-2023: A 43-Year-Old Woman with Chronic Diarrhea, Hair Loss, and Nail and Skin Changes
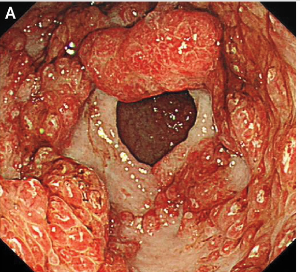
This case presents a polyposis disorder seen in adults and provides a useful differential diagnosis: autoimmune disorders including IBD, vasculitis, and celiac, primary adrenal insufficiency, heavy metal poisoning, amyloidosis, and cancer. This rare disorder has a reported “5-year mortality of 55%, mostly due to complications such as sepsis and gastrointestinal bleeding”
A few of the images from Figure 2:
Numerous sessile polyps in colonFrom Stomach
ChatGPT’s explanation of Cronkhite-Canada Syndrome:
Cronkhite-Canada syndrome (CCS) is a rare, noninherited, sporadic gastrointestinal polyposis syndrome that affects various parts of the digestive system. It is characterized by the presence of multiple polyps in the stomach and colon, as well as other distinctive features.
Epidemiology: Cronkhite-Canada syndrome is a very rare disorder, with only a few hundred cases reported worldwide. It typically affects older adults, with an average age of onset around 60 years, and there is no known genetic predisposition.
Clinical Presentation: Patients with Cronkhite-Canada syndrome often present with a combination of gastrointestinal and dermatological symptoms. The gastrointestinal manifestations include diarrhea, abdominal pain, weight loss, and protein-losing enteropathy. The dermatological symptoms consist of characteristic changes such as nail atrophy, hyperpigmentation, alopecia (hair loss), and skin hyperpigmentation.
Gastrointestinal Findings:
Polyposis: Multiple [hamartomotous] polyps are found in the stomach and colon. These polyps can vary in size and number.
Diarrhea and Abdominal Pain: Chronic diarrhea and abdominal pain are common symptoms due to the involvement of the digestive tract.
Dermatological Findings:
Nail Changes: Nail atrophy, ridges, and splitting are commonly observed.
Skin Changes: Hyperpigmentation of the skin, especially on the palms and soles, is a distinctive feature.
Alopecia: Hair loss is often present.
Laboratory Findings: Patients with Cronkhite-Canada syndrome may exhibit laboratory abnormalities, including hypoalbuminemia (low levels of albumin in the blood), hypoproteinemia, and electrolyte imbalances due to protein loss in the gastrointestinal tract.
Diagnosis: Diagnosis is based on a combination of clinical presentation, endoscopic findings, and pathology results from biopsies of the affected gastrointestinal tissue.
Treatment: Management of Cronkhite-Canada syndrome involves a multidisciplinary approach. Nutritional support is essential, and patients may require supplementation of protein and nutrients. Corticosteroids are often used to suppress inflammation, and immunosuppressive agents may be considered in refractory cases. Regular surveillance endoscopy is necessary to monitor polyp growth and assess response to treatment.
Patients diagnosed with nonerosive gastroesophageal reflux disease did not have a higher incidence of esophageal adenocarcinoma than the general population in a new study published in the BMJ.
This extensive population-based cohort study leveraged data spanning over three decades from national healthcare registries in Denmark, Finland and Sweden, known for their broad scope and high quality…
The incidence rate of EAC [esophageal adenocarcinoma] among 285,811 patients with nonerosive GERD (no esophagitis, Barrett’s esophagus or other esophageal condition), was 11.0 per 100,000 person-years, similar to that of the general population (BMJ 2023;382:e076017). Moreover, the rate remained stable regardless of the length of follow-up…
Harish K. Gagneja, MD, FACG, AGAF, FASGE, who was not involved in the research, commented that “patients with nonerosive GERD don’t require additional follow-up endoscopies unless they have alarm symptoms such as dysphagia, weight loss or anemia, etc.”…
The findings will need to be confirmed in well-designed studies from other countries. But the large sample size, population-based design, substantial duration of follow-up and inclusion of a contrasting erosive GERD cohort for validation are just some of the study’s strengths, supporting the validity of its findings.
My take: This study indicates that nonerosive reflux was not associated with an increased risk of esophageal adenocarcinoma.
Chen H, et al. NEJM 2023; 389: 1649-1659. Thalidomide for Recurrent Bleeding Due to Small-Intestinal Angiodysplasia
In this multicenter, double-blind, randomized, placebo-controlled trial, 150 adult patients underwent randomization: 51 to the 100-mg thalidomide group, 49 to the 50-mg thalidomide group, and 50 to the placebo group. Thalidomide has antiangiogenic activity, with inhibition of VEGF. It also has many adverse effects of thalidomide including peripheral neuropathy, fatigue, and teratogenic effects.
Key finding:
The percentages of patients with an effective response in the 100-mg thalidomide group, 50-mg thalidomide group, and placebo group were 68.6%, 51.0%, and 16.0%, respectively
Discussion points -(from the associated editorial by Loren Laine): The data for thalidomide for small-intestinal angiodysplasia is “of higher quality than evidence for any other therapy for this indication. In addition,….thalidomide may be disease-modifying, with efficacy persisting after discontinuation. However, many clinicians will still use somatostatin analogues first” due to convenience and safety.
My take: I am glad this is a rare problem in pediatrics. I am not at all excited about using thalidomide.
Background/Methods: The QUASAR Phase 2b Induction Study evaluated the efficacy and safety of guselkumab, an interleukin-23p19 subunit antagonist, in patients with moderately to severely active ulcerative colitis (UC) with prior inadequate response and/or intolerance to corticosteroids, immunosuppressants, and/or advanced therapy. In this double-blind, placebo-controlled, dose-ranging, induction study, adult patients (n=313), with median disease duration of 7.5 years, were randomized (1:1:1) to receive intravenous guselkumab 200 or 400 mg or placebo at weeks 0/4/8.
Key findings:
Week-12 clinical response percentage was greater with guselkumab 200 mg (61.4%) and 400 mg (60.7%) vs placebo (27.6%; both P < .001). (Patients received IV induction at 0,4, and 8 weeks)
Greater proportions of guselkumab-treated vs placebo-treated patients achieved all major secondary endpoints (clinical remission, symptomatic remission, endoscopic improvement, histo-endoscopic mucosal improvement, and endoscopic normalization) at week 12
Among guselkumab week-12 clinical nonresponders, 54.3% and 50.0% of patients in the 200- and 400-mg groups, respectively, achieved clinical response at week 24 (after another dose of guselkumab (2nd dose SC). Thus, by week 24, 80.2% (81/101) of patients in the 200 mg IV induction and 78.5% *84/107) in the 400 mg IV induction had a clinical response.
Clinical response was noted as early as 2 weeks (first timepoint assessed)
Safety was similar among guselkumab and placebo groups.
My take: This is an era with rapidly expanding medical treatments for inflammatory bowel disease; it should help reduce the problem of individuals who are refractory to available treatments.
In October, the FDA approved etrasimod (Velsipity, Pfizer) for moderate to severe active UC in adults. Etrasimod, an oral sphingosine-1-phosphate (S1P) receptor, binds with high affinity to receptors 1, 4, and 5. It is the second agent in the S1P class approved for UC. The other agent, ozanimod (Zeposia, Bristol-Myers Squibb), which was approved for moderate to severe active UC in May 2021, is an S1P receptor modulator that is selective for the S1P1 and S1P5 receptors located on endothelial cells and oligodendrocytes, respectively.
Etrasimod’s approval was based on safety and efficacy data from two randomized, double-blind, placebo-controlled phase 3 trials ― ELEVATE UC 52 trial, and ELEVATE UC 12 trial. The Lancet published full results from the two trials on March 2. Both trials enrolled patients with UC who had previously failed or were intolerant of at least one conventional, biologic, or Janus kinase (JAK) inhibitor therapy.
In ELEVATE UC 52, clinical remission at 12 weeks occurred in 27% of patients taking etrasimod, vs 7% of patients taking a placebo (20% difference; P ˂.001). At week 52, remission rates were 32% with active treatment, vs. 7% with placebo (26% difference; P ˂ .001).
In ELEVATE UC 12, clinical remission was achieved among 26% of patients who received etrasimod, vs 15.0% of patients who received placebo (11% difference; P < .05).
The approved recommended dose is 2 mg once daily. The most common side effects of etrasimod are headache, elevated values on liver tests, worsening of UC, SARS-CoV-2 infection, dizziness, pyrexia, arthralgia, abdominal pain, and nausea
My take: It is not exactly clear where etrasimod or ozanimod should be positioned for ulcerative colitis therapy as several other drug classes have much higher response rates.
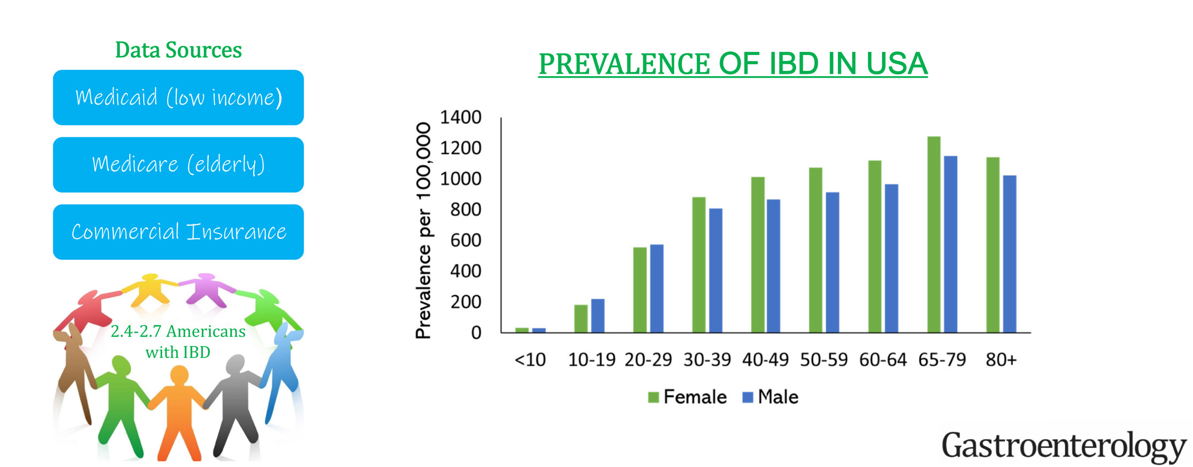
This “INPUT” (INcidence, Prevalence, Treatment and OUTome in Patients with IBD) study used 4 different data sets to provide “the clearest depiction to date of IBD [epidemiology] in the U.S.
Key findings:
The age-, sex- and insurance-standardized prevalence of IBD was 721 per 100,000 population. This equates to estimated 2.39 million Americans with IBD.
Sub-category prevalence: the prevalence of IBD per 100,000 population was 812 in White, 504 in Black, 403 in Asian, and 458 in Hispanic Americans.
My take: The prevalence of IBD continues to increase and the U.S. has one of the highest rates in the world.
On May 30, 2018, the US Food and Drug Administration (FDA) expanded the indication of tofacitinib (Xeljanz; Pfizer), an oral Janus kinase (JAK) inhibitor, for the treatment of adults with moderately to severely active ulcerative colitis. However, the optimal dosing remains unclear.
In this “real-world” study by Yu et al, a retrospective review of 162 patients was conducted (2012-2022). 52% continued 10 mg twice daily while 48% underwent dose de-escalation to 5 mg twice daily. The primary outcome was evidence of UC disease activity–related events: hospitalization/surgery, corticosteroid initiation, tofacitinib dose increase, or therapy switch.
Key findings:
Cumulative incidence rates of UC events at 12 months were similar in patients with and without dose de-escalation (56% vs 58%; P = .81)
An induction course with 10 mg twice daily for more than 16 weeks was protective of UC events (hazard ratio [HR], 0.37) while ongoing severe disease (Mayo 3) was associated with UC events (HR, 6.41)
Twenty-nine percent of patients with UC events had their dose re-escalated to 10 mg twice daily, with only 63% able to recapture clinical response at 12 months
Discussion Points:
“Although the product label recommends dose de-escalation after 8 or 16 weeks, clinical practice is variable in the real-world setting… In this retrospective real-world study of moderate to severe UC patients with almost half undergoing dose de-escalation, we observed that more than half of patients experienced a UC disease activity–related event within 12 months after dose de-escalation, particularly in patients with an induction course of fewer than 16 weeks and active endoscopic disease at 6 months after induction…”
” Although dose de-escalation is preferable for long-term maintenance therapy to reduce the potential lifetime risk of medication-related adverse events [eg. VTE], it must be balanced with sustained remission to prevent short- and long-term disease-related complications.”
“In the OCTAVE study which reported higher rates of long-term remission, patients de-escalated only after having shown clinical and endoscopic remission after 52 weeks on tofacitinib 10 mg twice daily”
My take (borrowed from authors): “Emphasis should be placed on clinical and endoscopic evidence of improvement before consideration of dose de-escalation to ensure the highest probability of treatment success.” This advice, though, may conflict with product labelling which states that “tofacitinib induction with 10 mg twice daily beyond 16 weeks is not recommended; in fact, it is recommended to stop after 16 weeks if adequate response has not been achieved.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
On meta-analysis of 13 studies (3756 patients; median follow-up, 12 months; 41% with variants), HLA-DQA1∗05 variants were associated with 75% higher risk of immunogenicity compared with non-carriers (relative risk, 1.75) with considerable heterogeneity (I2 = 62%) (low certainty evidence).
In addition, patients with HLA-QQA1*05 variants had clinical loss of response (LOR) in 67% compared to 30% in those without this variant (wild-type); thus, a 124% higher risk of LOR.
Positive and negative predictive values of HLA-DQA1∗05 variants for predicting immunogenicity were 30% and 80%, respectively
Proactive therapeutic drug monitoring, but not concomitant use of IMMs, IMIDs, and TNF-α antagonist-type, modified this association.
My take:
The ~40% of individuals with HLA-DQA1*05 variants are at higher risk of LOR and are more likely to benefit from both therapeutic drug monitoring and probably from use of combination (with immunomodulator) therapy.
The positive predictive value (30%) is low indicating that the majority of patients with these variants will not develop anti-drug antibodies within 12 months.
In those with negative testing for HLA-DQA1*05 (~60%), the higher negative predictive value indicates a patient is more likely to do well with monotherapy.
HLA-DQA1*05 testing is available commercially (usually part of Celiac HLA typing).
This is the Initiation Well at Quinta da Regaleira in Sintra, Portugal. It is pretty cool because it seems to start at ground level and then goes down many floors. There is an exit to a number of tunnels at the lower level.
Methods: A systematic search was conducted from August 1999 to July 2021 for studies (50 studies identified) reporting loss of response and dose escalation during infliximab and/or adalimumab use in ulcerative colitis patients with primary response
Key findings:
Annual loss of response was 10% for infliximab and 13% for adalimumab, with higher rates during the first year.
The annual LOR incidences were higher during the first 65 weeks of treatment for both IFX (14%) and ADA (23%).
Annual dose escalation rates were 14% (infliximab) and 21% (adalimumab), with clinical benefit in 72% and 52%, respectively
Key finding: 4 patients (age 18-25 yrs) received upadacitinib for acute severe ulcerative colitis (ASUC) after failing to respond to infliximab and IV steroids. 3 of 4 responded to treatment (45 mg/day) between 4 to 8 days. Three months later, two of these patients were in steroid-free clinical-endoscopic remission and one had maintained a clinical response.
In their discussion, the authors note a similar response rate to tofacitinib, another JAK inhibitor, for ASUC; though, the authors speculate that upadacitinib may be efficacious.
In a a prospective cohort study of 133,137 individuals between the ages of 20 and 80 from 24 countries, the authors examined the relationship between exposures to antibiotics, NSAIDs and hormonal therapies with the development of IBD over a median 11 year period.
Key findings:
Incident IBD was associated significantly with baseline antibiotic (aOR, 2.81; P = .0001) and hormonal medication use (aOR, 4.43; P = .001).
Nonsteroidal anti-inflammatory drug users also were observed to have increased odds of IBD (aOR, 1.80 P = .002), which was driven by long-term use (aOR, 5.58; P < .001)