A recent study (SD Delshad, CV Almario et al. Gastroenterol 2020; 158: 1250-61) used survey data from an APP, MyGiHealth, to assess prevalence of reflux symptoms and symptoms that had not responded to proton pump inhibitor treatment.
Key findings:
- In 2015, among 71,812 participants, 32,878 (44.1%) reported reflux symptoms previously and 23,039 (30.9%) reported reflux symptoms in previous week
- 35% with reflux symptoms were currently receiving treatment: 55% PPIs, 24% H2RAs, and 24% antacids
- Of the 3229 taking daily PPIs, 54% reported persistent reflux symptoms (≥2 days per week)
- Age range of respondents was 33% for 18-29, 27% for 30-39, 17% for 40-49, 15% for 50-59, and 8% ≥60
Limitations:
- Potential selection bias as there was only a 5.5% response rate among the entire eligible population of 1.3 million
- Reflux symptoms frequently is not due to reflux disease
My take: There are a lot of folks with reflux symptoms and many have ongoing symptoms despite treatment; hence, lots of opportunity to help (and job security)
Related blog posts:
- What’s Going On in Patients with Reflux Who Fail Proton Pump Inhibitors
- How to Make a Study Look Favorable for Reflux Surgery Compared to Medical Treatment | gutsandgrowth
- Which PPIs are most potent?
- Impedance May Help in Borderline Reflux Disease Assessment | gutsandgrowth
- Deconstructing PPI Risks with 8 Billion Data Points
- How Many Kids with Reflux Actually Have Reflux?
- Why didn’t patient with documented reflux get better with PPI …
- Failure of PPI test | gutsandgrowth
- Guidelines on Functional Heartburn
- Better to do a coin toss than an ENT exam to determine reflux
- How Likely is Reflux in Infants with “Reflux-like … – gutsandgrowth
- PPI Webinar
- The Connection Between Anxiety and Gastroesophageal Reflux Disease
- PPIs: Good News on Safety Large randomized double-blind study of pantoprazole: “we found that pantoprazole is not associated with any adverse event when used for 3 years, with the possible exception of an increased risk of enteric infections.”
Also from NY Times: Coronavirus Ravaged a Choir. But Isolation Helped Contain It.
“One sick singer attended choir practice, infecting 52 others, two of whom died. A study released by the C.D.C. shows that self-isolation and tracing efforts helped contain the outbreak.” Only 8 of the 61 choir members did not get sick.
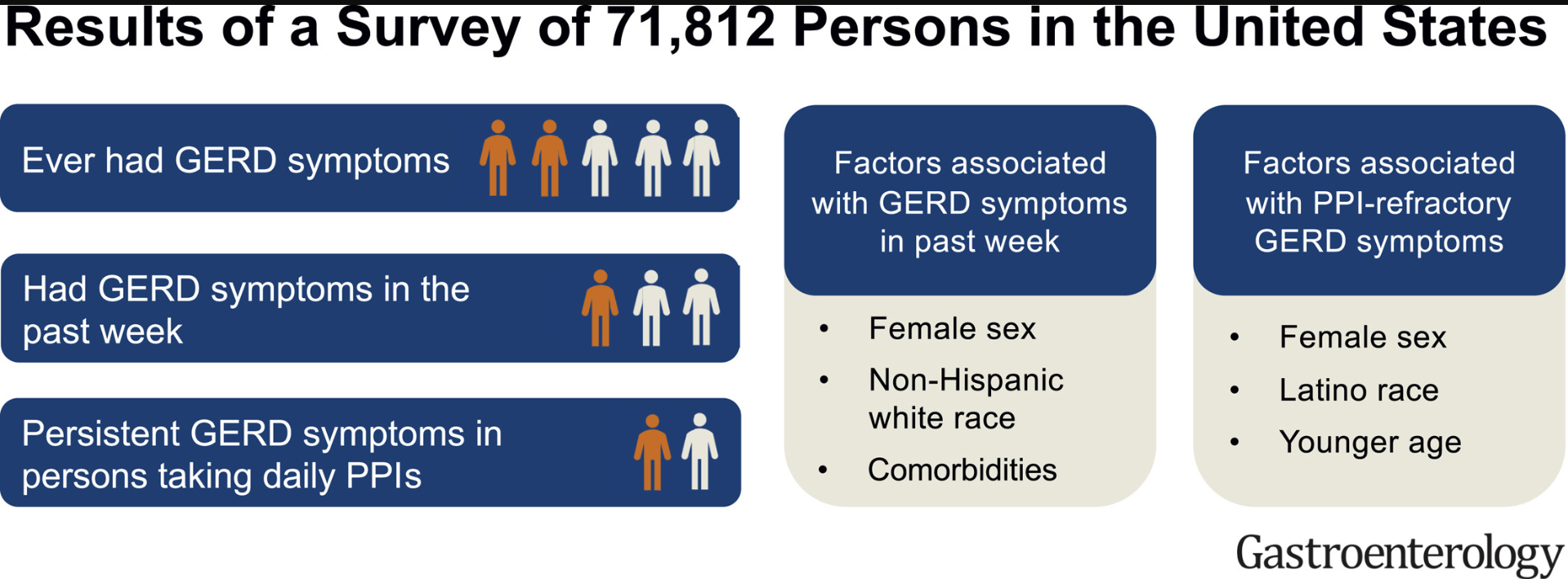
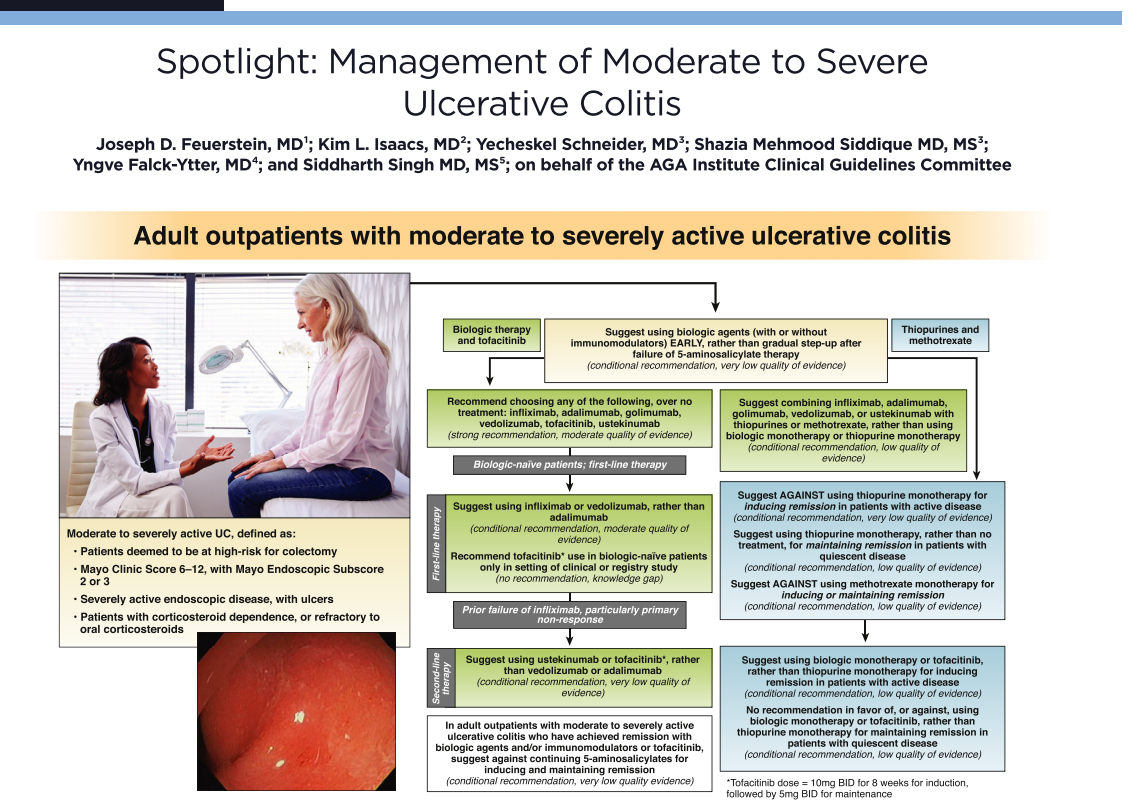
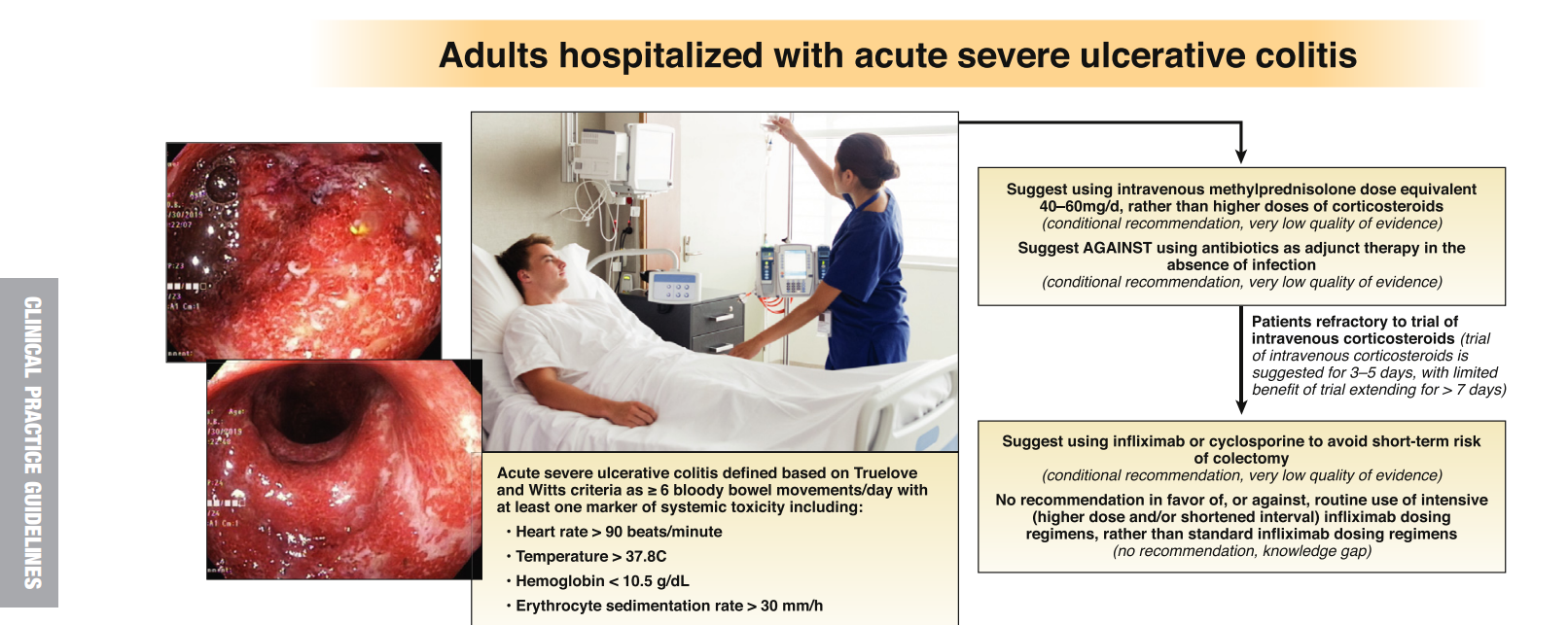
Graphical Abstract