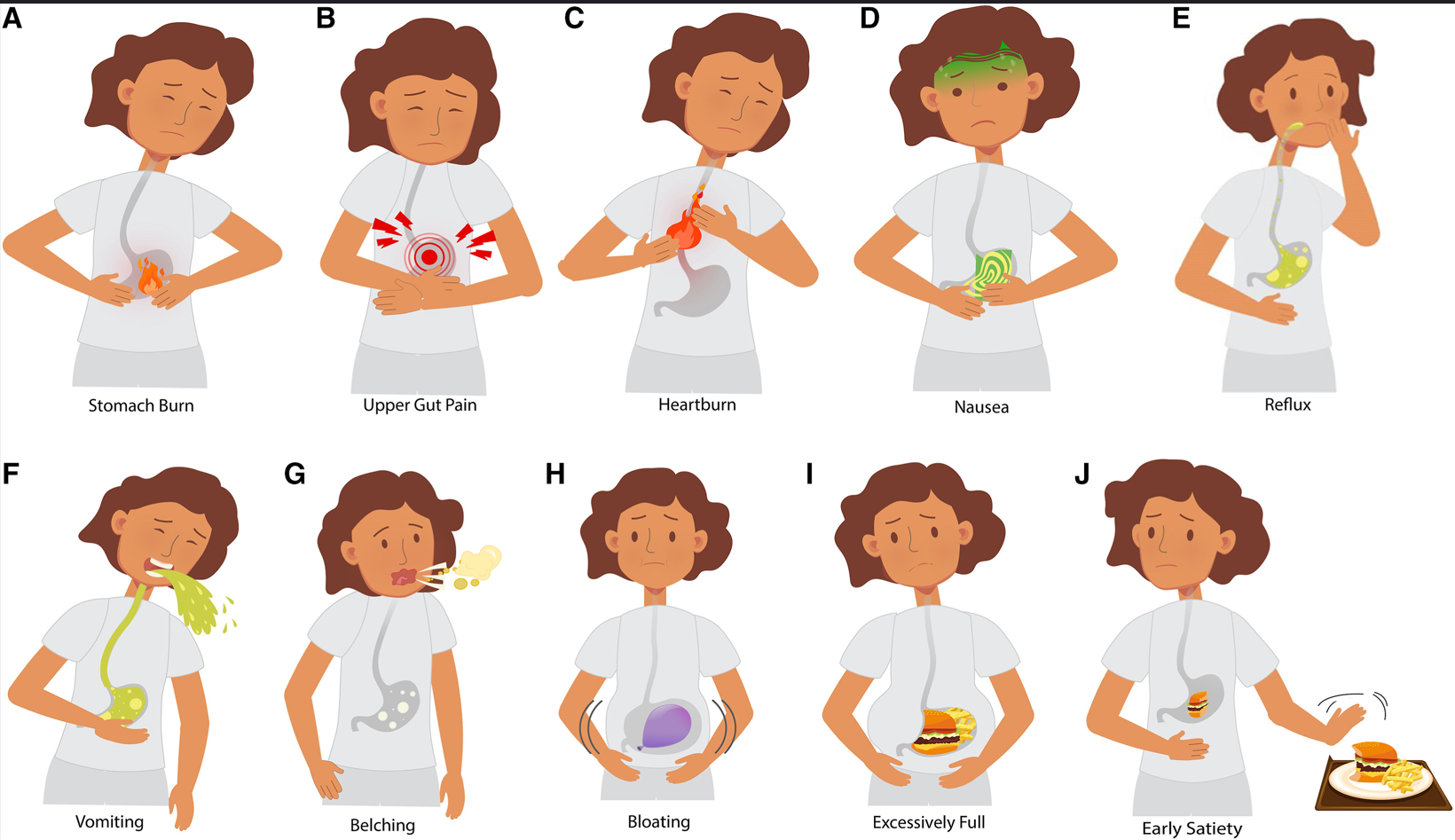
The authors attempted to develop useful pictograms to help enable standardization of symptom reporting in children with gastroduodenal disorders.
Figure 2: Pediatric gastroduodenal symptom pictograms. A, stomach burn; B, upper gut pain; C, heartburn; D, nausea; E, reflux; F, vomiting; G, belching; H, bloating; I, excessively full; and J, early satiety. (The same images were used to create the animated set).
Key findings:
Face and content validity were higher for the pediatric static and animated pictogram sets compared with pre-existing adult pictograms (78% vs 78% vs 61%).
Participants with worse gastric symptoms had superior comprehension of the pediatric pictograms (χ2 [8, N = 118] P < .001)
“Little significant comprehension was gained by having the animated pictograms.”
My take: Some research while worthwhile does not pan out. This is what I was thinking when I read this study. Upper GI symptoms are difficult to convey in pictures; in addition, some patients will have multiple overlapping symptoms. This is why the validity percentages are not higher. I don’t foresee using these pictograms in clinical practice.
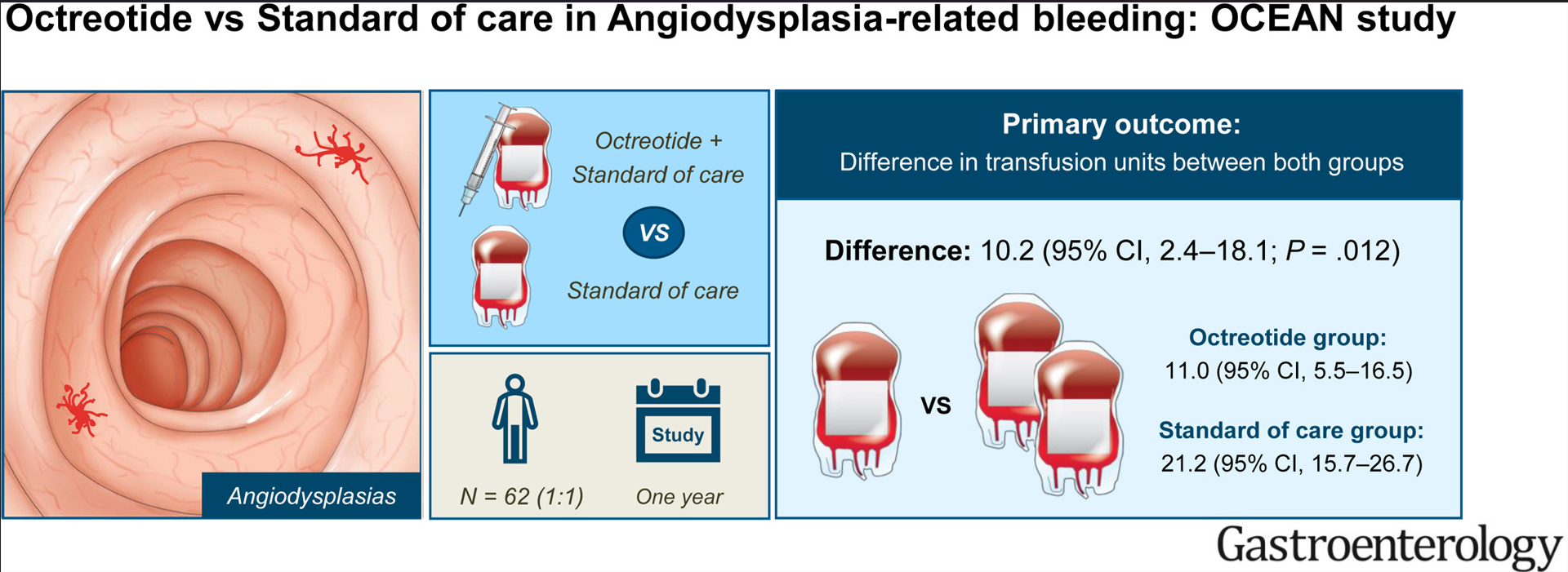
Methods: The study was designed as a multicenter, open-label, randomized controlled trial. Patients with angiodysplasia bleeding were required to have had at least 4 red blood cell (RBC) units or parental iron infusions, or both, in the year preceding randomization. Patients were allocated (1:1) to 40-mg octreotide long-acting release intramuscular every 28 days or standard of care, including endoscopic therapy.
Key findings:
Baseline: Patients (n=62, with mean age 72 years) required a mean number of 20.3 transfusion units and 2.4 endoscopic procedures in the year before enrollment.
During Study: The total number of transfusions was lower with octreotide (11.0) compared with standard of care (21.2). Octreotide reduced the annual volume of endoscopic procedures by 0.9.
Adverse events: Octreotide-related AEs were common (65%);however, these AEs were mild and self-limiting nature. They “rarely elicit treatment discontinuation.”
mean number of transfusion units patients in the octreotide group and standard of care group
My take: Fortunately (for me), angiodysplasia is quite rare in the pediatric age group. In adults, octreotide helps reduce transfusions and need for endoscopy.
This lengthy article details “a little-known data analytics firm called MultiPlan. It works with UnitedHealthcare, Cigna, Aetna and other big insurers to decide how much so-called out-of-network medical providers should be paid. It promises to help contain medical costs using fair and independent analysis.”
“But a New York Times investigation, based on interviews and confidential documents, shows that MultiPlan and the insurance companies have a large and mostly hidden financial incentive to cut those reimbursements as much as possible, even if it means saddling patients with large bills. The formula for MultiPlan and the insurance companies is simple: The smaller the reimbursement, the larger their fee.”
The backdrop on MultiPlan was a scandal 15 years ago. The NY Attorney General concluded that the insurance companies had “a payment system riddled with conflicts of interest had been shortchanging patients, and at its core was a data company called Ingenix. Insurers used the company, a UnitedHealth subsidiary, to unfairly lower their payments and shift costs to patients, the probe found…UnitedHealthcare, Cigna, Aetna and other major insurers agreed to replace Ingenix with a nonprofit that would provide independent pricing data…The companies were required to use the nonprofit database for only five years.” Subsequently, the insurance companies turned to Multiplan. In a 2015 email, a Cigna risk officer:: “We cannot develop these charges internally (think of when Ingenix was sued for creating out-of-network reimbursements). We need someone (external to Cigna) to develop acceptable” rates, she wrote.
Some of the examples of out-of-network charges in the article included:
Gail Larson had surgery on a non-healing chest wound. “UnitedHealthcare, advising that Dr. Rabinowitz would be paid $5,449.27 — a small fraction of what he had billed the insurance company. That left Ms. Lawson with a bill of more than $100,000.”
“Kelsey Toney, who provides behavioral therapy for children with autism, who was receiving a payment of half the medicaid rate for providing care.”
“Cari Campbell, who received fertility treatment in Minnesota, was charged thousands of dollars.”
“Justin Dynlacht, who has Crohn’s disease, paid extra for a plan that covered such visits. After seeing two in-network doctors about persistent abdominal pain, he went to an outside specialist who discovered a hernia containing abdominal tissue. Aetna sent the specialist’s claims to MultiPlan, and Mr. Dynlacht was left with thousands of dollars in bills.”
My take: Insurance companies in coordination with Multiplan rip off their policy holders by not providing reasonable coverage for their out-of-network medical care. Ultimately, patients will be increasingly affected as many physicians/hospitals walk away from insurers who are offering low reimbursement rates to in-network providers too. Insurance companies are incentivized to not care.
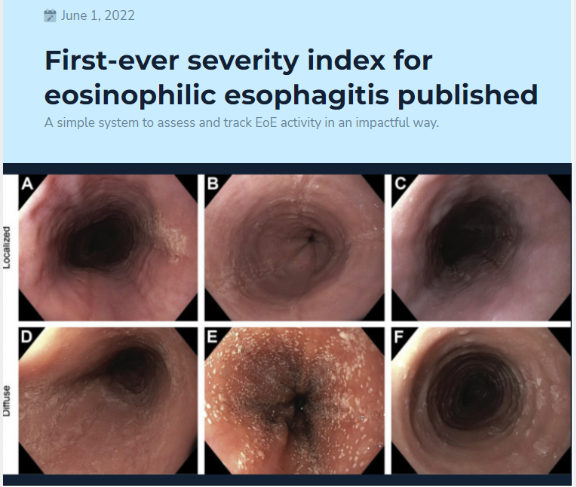
This was a retrospective analysis on a prospectively enrolled cohort of children at a single center who were treated as part of routine clinical care. I-SEE was calculated at the diagnostic and follow-up endoscopies over a mean of 6.6 years.
Key findings:
Of 67 children who met study criteria of at least 3 endoscopies over at least 2 years of follow-up time, 43%, 36%, and 21% had mild, moderate, and severe I-SEE scores at baseline, respectively.
By the last instance, the overall I-SEE score dropped to 3.9 (P < .001). Body mass index <5% and poor feeding were more common in the children with severe I-SEE scores at baseline, and both improved by the last instance.
The discussion notes that I-SEE metric was developed to determine EoE severity and for tracking purposes to gauge effectiveness of therapy. They note that most patients improved but a score of 0, indicating deep remission, was difficult to achieve at the population level. They also anticipate further modifications to I-SEE “such as age or an assessment of symptoms that reflects inflammatory or fibrotic disease.”
My take: I-SEE provides a way to objectively assess and follow EoE severity at all ages.
Like yesterday’s article on GTs, this is another terrific review with plenty of helpful images and advice regarding ostomy management.
Background: “There are upwards of 1 million people living with ostomies (ostomates) in the United States.” “Approximately 75% of all ostomies in the pediatric population are created in the neonatal or infant patient.”
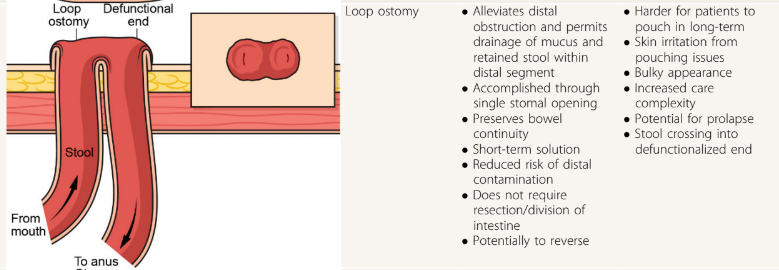
Table 1 lists the purposes and types of ostomies including gastrostomy, jejunostomy, ileostomy, appendicostomy (Malone), cecostomy, colostomy and urinary diversions (eg. Mitrofanoff).
Surgical considerations are reviewed including optimizing nutrition preoperatively and minimizing corticosteroids. Biologics: “The most recent evidence does not support a delay in gastrointestinal surgery for children with IBD receiving biological therapy…[and] typically, biological therapy can be resumed 14 to 28 days after the operation.” For oral small molecules (with short half-lives), these may be restarted sooner if indicated.
Table 2 provides pictures of the lower ostomies. For example:
Postoperative care is discussed including healing times, need for wound ostomy nurse input, and addressing self-image. Patients with motility disorders are “more likely to experience postoperative complications”
Table 4 details the products for pouch care including pouching systems, skin barriers, pouch liner, gas vent, pouch lubricant, pouch covers, and adhesive remover.
Table 5 summarized ostomy-related complications and treatments. Complications include stomal necrosis, stomal bleeding, stomal retraction, mucocutaneous separation, parastomal hernia, stoma prolapse (can apply cool compresses, apply osmotic agent (sugar) or manually reduce), stoma stenosis, and dermatitis.
Table 6 addresses medical management issues like odor, blockage, diarrhea, and constipation. This table also provides recipes for antegrade enemas (see below) and links including a very useful bowel management guide for families (28 pg from Boston Children’s) and enema ingredients and supplies (2 pg from Seattle Children’s); the latter has some overlapping information with the former.
At the conclusion of the article, there is further discussion of systemic and ostomy-related complications (much of which is summarized in Table 5). The article references the Ostomy Skin Tool as a metric to follow the clinical state of the ostomy. The United Ostomy Associations of America (ostomy.org) is listed as a good resource (which it is!).
My take: This is a very useful resource. Even a quick read will make clinicians appreciative of having the assistance wound ostomy nurses.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Thanks to Patrick Reeves for sharing this reference. While reading this article, I was reminded of Debbie Mason RN. She worked mainly for Colin Rudolph when I was a fellow at Cincinnati. She would teach the fellows the ‘ins and outs’ regarding gastrostomy tubes (GTs).
Some of the points from this article:
Background: In one large study, 25% of hospitalized pediatric patients in 63 U.S. hospitals required a temporary NG tube. GTs “preferred for longer-term access due to being less prone to accidental dislodgement, blockage, and interruption of feeds. They are also more durable, discrete, and avoid nasal trauma.” They are probably safer too for longer-term use. (An omission in the article: AMT bridles can help maintain NGs.)
Indications: Reviews the extensive list of reasons for GT placement, most related to inadequate nutritional intake (related to many chronic disease processes)
Contraindications are reviewed. “Absolute contraindications include active sepsis or peritonitis, massive ascites, uncorrectable coagulopathy, portal hypertension with significant varices, and history of total gastrectomy.” Transoral PEG tube is contraindicated, as well, if pharyngeal or esophageal obstruction, malrotation, or colonic interposition.
Preprocedural evaluation is described. Some have recommended UGI prior to placement in those with congenital anomalies. Others have stated that “even congenital anomalies should not mandate an upper GI series given how rare malrotation is in general.” Many children benefit from NG feeding trials prior to GT placement which can also improve nutritional status preoperatively.
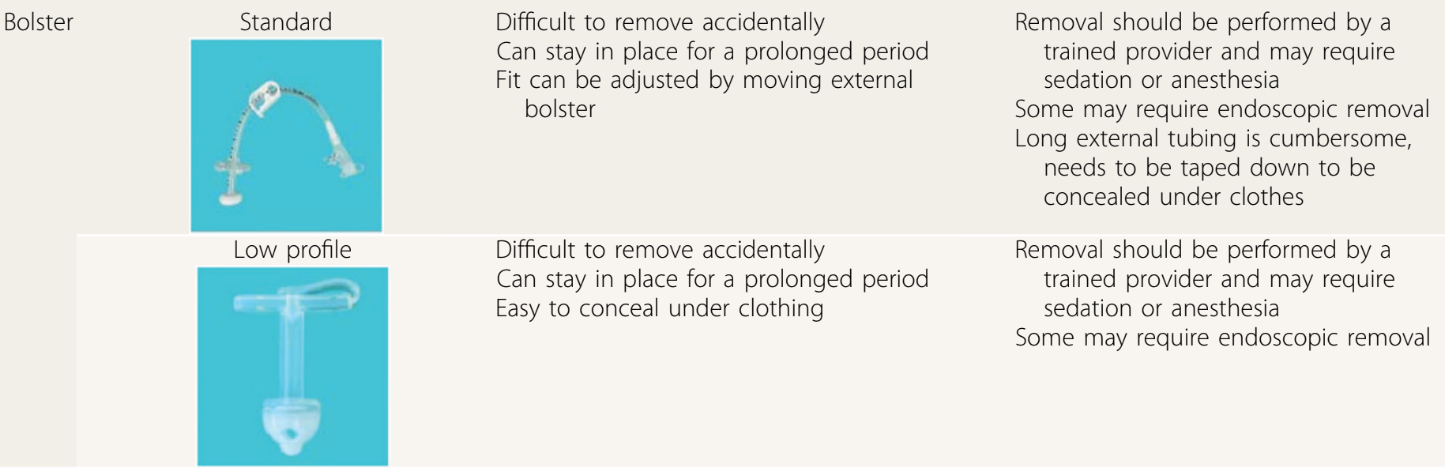
The placement methods and types of GTs are reviewed. “As of now, there is no clearly identified optimal technique” (eg. laparoscopic GT vs PEG). The others note a meta-analysis of 22 studies (n >5000) found a higher rate of major complications with PEG placement. The authors recommend T-fasteners if GT balloon is used for initial placement.
Examples of bolster-type (non-balloon) GTs:
GT complications are discussed including infection, peritonitis, bleeding (rare to need a transfusion), injury to adjacent organs, pneumoperitoneum (usually benign and transient), hypergranulation, cellulitis (often treated with a first-generation cephalosporin or topical mupirocin), dislodgement, tube migration, and buried bumper syndrome. For early dislodgement (especially first 4-6 weeks after placement), blind reinsertion should be avoided.
GT care: The authors recommend starting feeds “not more than 3 to 6 hours” after placement to monitor for immediate postoperative complications, and cleaning site with warm water, saline or soap. Once the site has healed showering and bathing can resume; swimming can be permitted a few weeks after placement. Medications should be given via gastric port (if GJ) for better absorption of medications and lessen risk of tube clogging.
Troubleshooting: This is the most useful part of this article. Advice on peristomal leakage: “Placing larger tubes should be avoided because this will only enlarge the stoma tract…removal of the tube for a few hours can be considered because this permits the tract to start closing.” Leakage is often due to issues with balloon volume, poor fit, gastric pressure (eg dysmotility, gastroparesis) and poor wound healing. Clogging: “Carbonated beverages, juices, and meat tenderizer…studies have not shown these to be effective.” Lukewarm water, left to stand 20 minutes, is the first line agent for declogging. Other options include commercial enzymatic decloggers, and mechanical decloggers.
GT removal is discussed and I disagree with the authors that “persistent gastrocutaneous fistulas are rare after removal” (though the majority will close with conservative management). The authors do not recommend cutting GT bolsters due to risk of obstruction and note that endoscopic removal is often necessary.
My take: This article would be well-positioned as part of any GI fellows’ required curriculum and has a bunch of pointers for experienced clinicians as well. It could easily be used for material for ABP questions too. The article is much more detailed than the summary I have provided.
Also, another relevant resource (not discussed in article): Oley Foundation (oley.org). This foundation aims to help those living with home IV nutrition or tube feeding through advocacy, education, community and innovation.
Dr. Joel Rosh gave our group an excellent update on sequencing therapy for ulcerative colitis (UC). My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of his slides.
There are only two FDA-approved biologics in pediatric Ulcerative Colitis. It typically takes 8-10 years for a medication with approval in adults to receive FDA approval in children
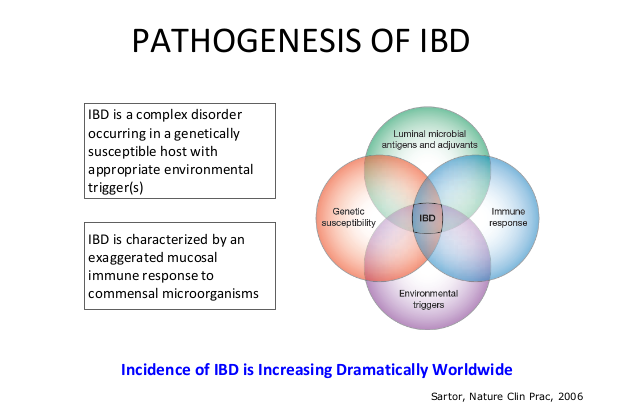
The concept of IBD as two diseases, Crohn’s disease and UC, is flawed; there are more than 200 susceptibility genes for inflammatory bowel disease
There has been an increasing incidence and prevalence of IBD. Some of this increase is likely due to our diet and its effects on the microbiome
Ultrasound is a nice tool to see what is going on in real time and shows that UC is really a transmural disease. UC changes in the bowel can result in fibrosis
Consider cytokine-basis for disease as a way to conceptualize disease presentation compared to organ-based disease. Many autoimmune diseases (eg. JIA, RA, Psoriasis) are different manifestations related to cytokine-based autoimmunity
Almost all pediatric IBD can be considered higher risk based on known risk factors including disease extent (>80% of pediatric UC is pancolitis) and disease age of onset
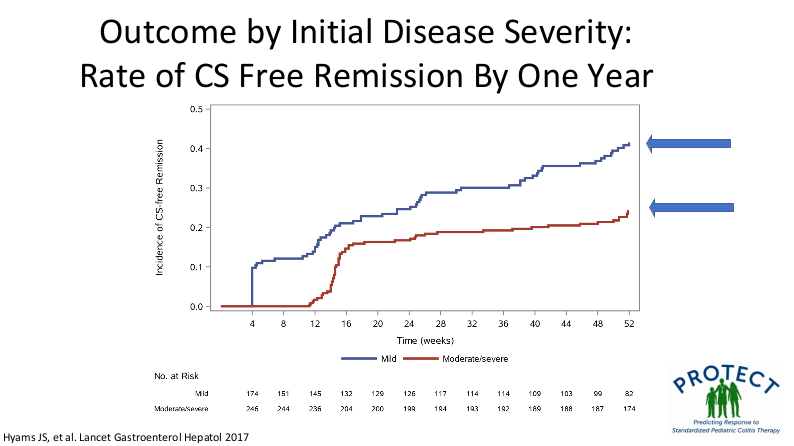
Mesalamine steroid-free clinical remission rates are about 1/3rd after 1 year of treatment
Overall, there has been an improvement in colectomy rates since 2001; there still appears to be a bump in the colectomy rate after having UC for more than 10 years
Elevated CRP is less common in patients with UC, compared to Crohn’s disease, and is a marker for more severe disease activity
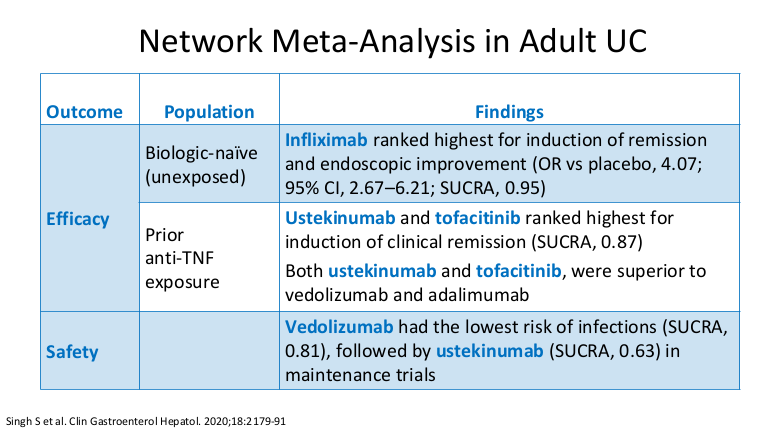
Dr. Rosh prefers to avoid some terms including biologic-naive and steroid failure; he favors biologic-unexposed for the former. For the latter, he tries to make it clear that the patient was not a steroid failure. Steroids failed the patient rather than the patient failing the steroids
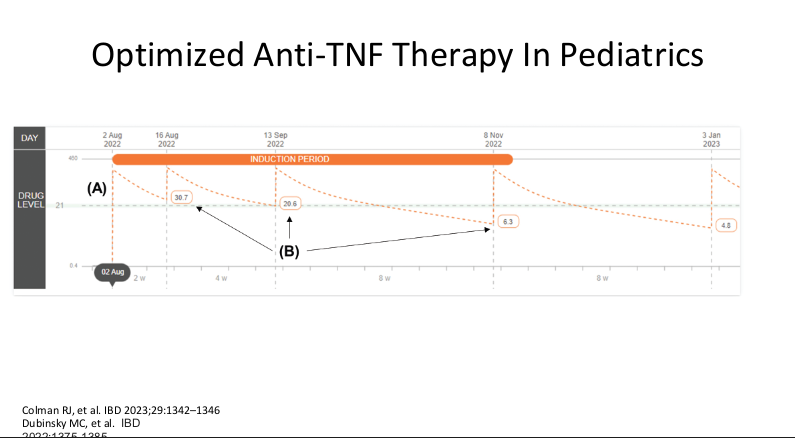
Therapeutic drug monitoring (TDM) is mainly beneficial for anti-TNF agents at this time. Use of TDM can help monotherapy achieve similar results as combination therapy. For infliximab, Dr. Rosh’s ‘rule of thumb’ is 28-18-8 for 2 week trough, 6 week trough, and maintenance trough. Therapeutic levels will meet or exceed these trough levels.
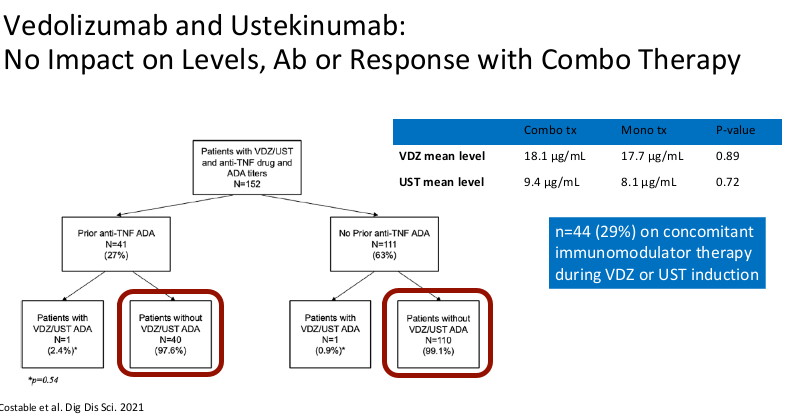
Combination therapy has not been shown to improve pharmacokinetics for vedolizumab or ustekinumab
Generally, a washout period is not needed when changing biologic therapies. In fact, having some overlap in the medications may have some therapeutic benefit
Upadacitinib (Rinvoq) appears to be the most effective JAK for IBD. It is labelled for use as a 2nd-line agent but may be superior for some sicker patients. Rinvoq could be considered as a ‘bridge’ medication in patients with acute severe ulcerative colitis with transition to another biologic like vedolizumab
It is important for families to be informed that there is a black box warning for the use of JAK inhibitors. However, major cardiac adverse events (MACE) do not appear to be increased in patients without preexisting cardiac disease risk factors
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“In 1868, the German physician Adolph Kussmaul looked inside the stomach of a human being. He chose to peruse the stomach of a professional sword-swallower, someone who was able to tolerate, although probably not to enjoy, a straight, 47-cm long metal tube with a diameter of 13 mm.1 This marked the beginning of the first era of endoscopy, the era of rigid endoscopy…encountered 2 fundamental problems. One, although a metal tube is straight, the gastrointestinal tract is not. And, two, the inside of the human body is dark.”
“Rudolf Schindler, working in Munich, realized that the rigid gastroscope “never could be routinely used.”2 In 1932 he designed a semiflexible endoscope, an invention that marked the beginning of the second era of endoscopy…[after surviving Dachau concentration camp], he settled at the University of Chicago.3“
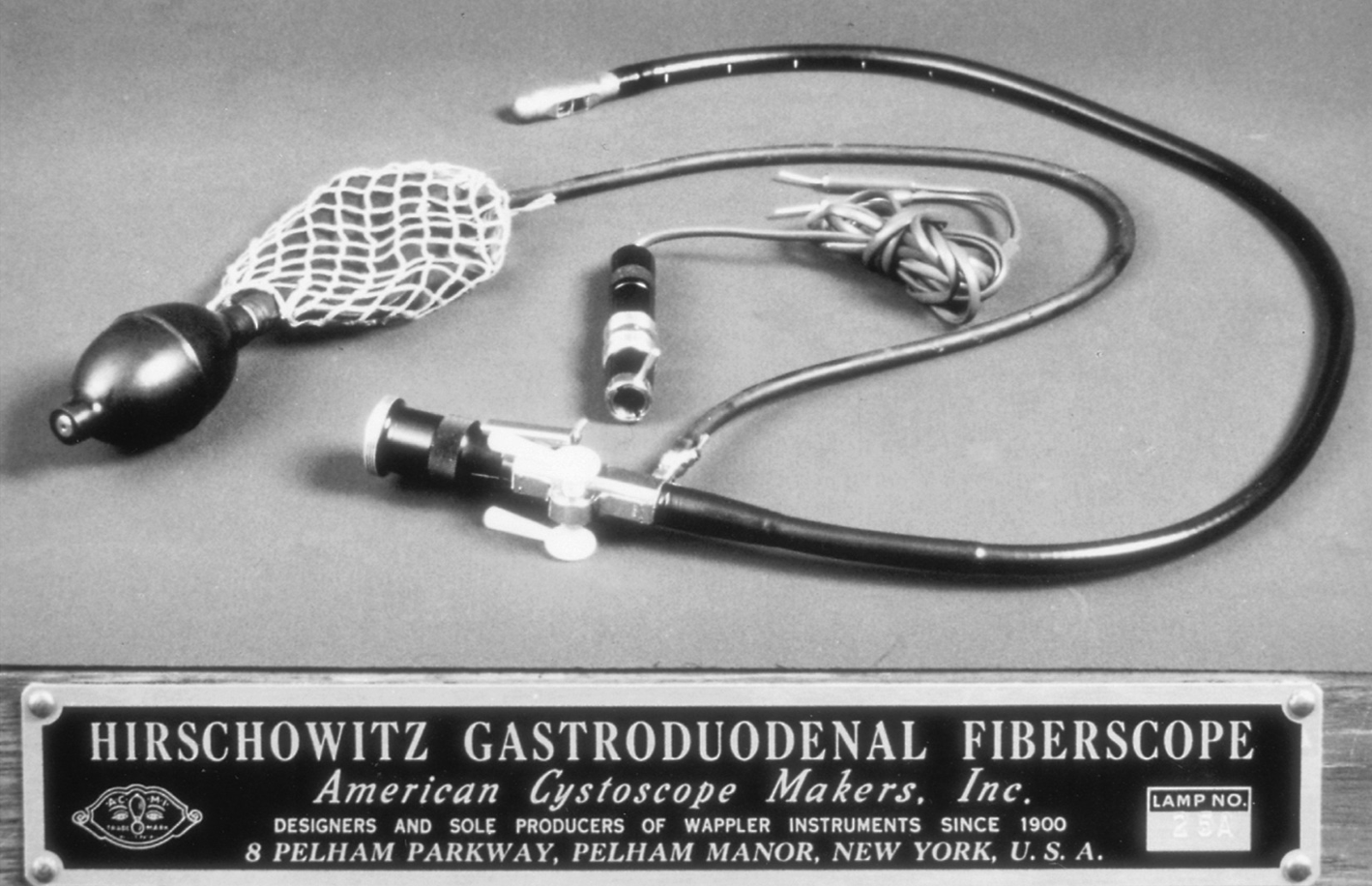
“In 1954, [Basil] Hirschowitz learned that it might be possible to create a device that could transmit optical images along a flexible axis. Working with 2 colleagues from the University of Michigan Physics Department, which was located not far from the Medical School, he created a prototype device for looking into the stomach.”
Related blog posts:
538: Gut Science Week describes Alexis St Martin (in 1822) who had a persistent gastrocutaneous fistula which enabled his doctor William Beaumont to do more than 200 experiments over 8 years on digestion.
My take: This guidance likely was derived from patients having sensitive exams without permission while under anesthesia. While this guidance is directed at hospital settings and hospital-based outpatient clinics where written consent is now needed, practitioners in the outpatient setting likely will need to better document permission prior to rectal examination and assure appropriate use of chaperones.
Resources:
CMS Revisions and clarifications to Hospital Interpretive Guidelines for Informed Consent Based on increasing concerns about the absence of informed patient consent prior to allowing practitioners or supervised medical, advanced practice provider, or other applicable students to perform training- and education-related examinations outside the medically necessary procedure (such as breast, pelvic, prostate, and rectal examinations), particularly on anesthetized patients, we are reinforcing hospitals’ informed consent obligations.
Methods: Retrospective cohort study (n=195) including consecutive CD patients starting treatment with IFX. Rates of transmural remission were compared between patients with and without therapeutic drug monitoring (target level: 5-7 µg/mL).
Key findings:
The rates of transmural remission were higher in patients under proactive therapeutic drug monitoring (37.2% vs 18.3%; P = .004) with similar results in the propensity score–matched analysis (34.2% vs 17.1%; P = .025).
In multivariate analysis, proactive therapeutic drug monitoring was independently associated with transmural remission (odds ratio, 2.95)
My take: Proactive therapeutic monitoring is beneficial in improving outcomes in patients with Crohn’s disease. Higher drug levels are likely to be particularly important to achieve adequate tissue penetration in transmural Crohn’s disease.